Muller-Weiss disease


Definition
Spontaneous osteonecrosis of the navicular
Spontaneous osteonecrosis of the navicular
Osteoarthritis
- abnormal morphology
- loss of head neck offset
- bony impingement on acetabulum
AVN

Osteonecrosis of the navicular
Present at age 4-6 years
- same as Perthes disease
M:F 5:1
Bilateral in 20%
Repetitive trauma to maturing ossific nucleus
< 60 with good bone stock and preserved joint space
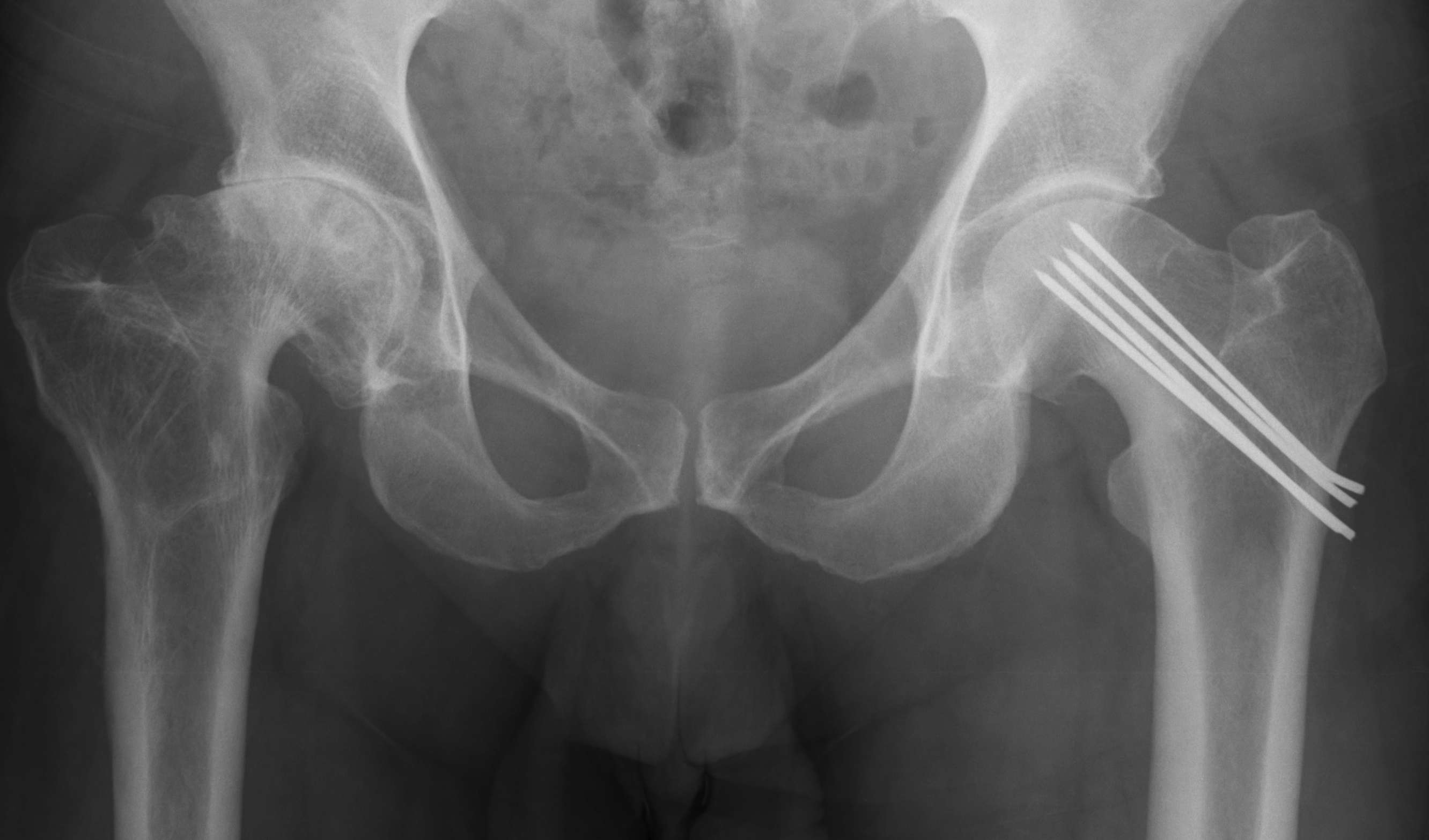
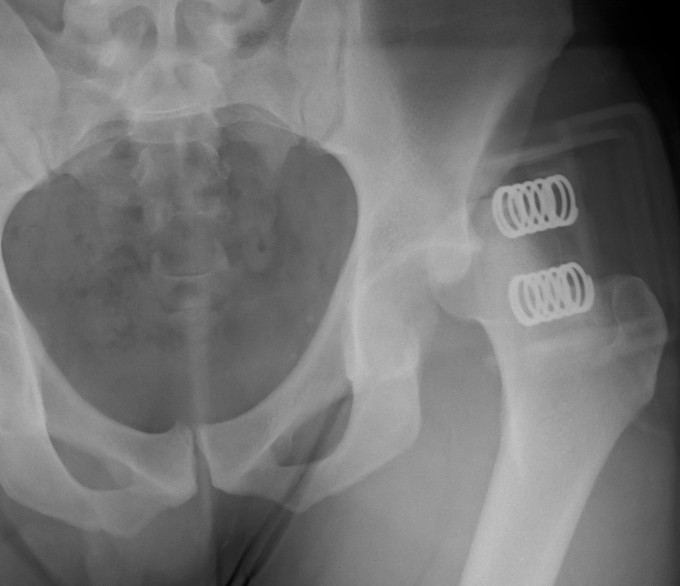
Union rates increased with anatomical reduction
Options
- closed reduction
- open reduction / if closed reduction fails
Accept
- no varus
- < 15o valgus
- < 10o AP plane
Education regarding shoe wear
- extra wide / large toe box
Insoles
- longitudinal arch support
- pre MT dome for metatarsalgia
- podiatry to attend to callosities
Toe spacers
Analgesia
1. Continued pain and discomfort
2. Difficulties with shoe wear
Young men
Posterior / Anterior 9:1
High velocity injury
- head direction at impact decides direction of dislocation
Anterior Dislocation
Externally rotated & abducted leg
- flexion = inferior dislocation
Stage 0
Natural history mixed
- depends on size of lesion and diagnosis
- treat if becomes asymptomatic
- may benefit from bisphosphonates
Stage 1 / Normal X-ray, abnormal MRI
Forage: 80% G/E
Bisphosphonates
Stage 2 / Abnormal X-ray with cysts and sclerosis
A: As for Stage I

Non-traumatic or traumatic condition of femoral head with bone death
20 - 50 yo (average 38)
- M: F 4:1
70-80% with AVN will progress within 1 year
Largely related to degree of displacement
Hawkins Type I
- 0% to 13%

Hawkins Type II
- 20% to 50%
- usually only patchy and not a problem (rarely collapses)
Xray
- sclerosis


CT