
Anatomy
Size
Strength
- 2 x strong as ACL
Length
- about the same as ACL
- 38 mm
Cross sectional area
- 150% of ACL
- 13 mm diameter
2 Bundles
1. Anterolateral
- most important
- double the size of the posteromedial
- tight in flexion
- try to reconstruct this bundle
2. Posteromedial
- tight in extension
Femoral insertion
Half moon
- anterolateral aspect MFC
- much more anterior than the origin of ACL
- inserts 5mm posterior to articular margin of MFC
- midpoint is 1 cm posterior to articular margin of MFC
- 1 or 11 o'clock
Radiographic anatomy of femoral PCL insertion
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3874986/pdf/aob-21-323.pdf
Tibial insertion
PCL facet
- 1 cm below joint line
Radiographic anatomy of the tibial insertion of PCL insertion
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4519663/pdf/main.pdf
Menisco-femoral ligaments
Both insert onto femur with PCL
Originate from posterior horn lateral meniscus
At least one present in > half of all knees
Humphrey
- <1/3 diameter of PCL
- anterior
Wrisberg Ligament
- half the diameter of the PCL
- posterior to the PCL
Ligament of Wrisberg MRI
Arterial supply
Middle genicular artery
Nerve Supply
Tibial nerve
Function
Primary restraint to posterior tibial translation
- secondary restraints are posterolateral corner
- posterior translation increased even further if PLC and PCL deficient
Secondary restraint to ER and varus
Incidence
10x less common ACL
Aetiology
Direct trauma
- posteriorly directed force on flexed knee
- dashboard injury
Indirect
- forced knee hyper-extension
Associated Injuries
Multi-ligament knee injury
- posterolateral corner
- posteromedial corner
- ACL
Clinical
Injury often unremarkable
- knee doesn't feel right
- don't feel pop or tear
- posterior knee pain
May complain of difficulties walking down stairs in chronic situation
Examination
Excessive Recurvatum

Positive Lachman's
Will be positive with both ACL and PCL
Posterior sag
- place knee at 90 degrees
- tibia will sag posteriorly
- loss of tibial step off (normal 1cm)

Posterior drawer
Restore step off first (tibia 1 cm anterior to femur) then push tibia back
- Grade 1: < 5mm
- Grade 2: 5 - 10mm
- Grade 3: > 10mm


Quadriceps Active Test
- patients contracts quadriceps with foot stabilised
- the tibia is reduced anteriorly from its subluxed position by the quadriceps
Exclude Associated Ligament injury
PLC instability
1. Posterolateral draw with foot ER
2. Dial test
- patient prone, external rotation
- > 10 - 15o compared with other side abnormal
- asymmetry 30o posterolateral corner only
- asymmetry 30 and 90o, PCL and posterolateral corner

Bony Avulsion


Chronic bony avulsion PCL
Posterior subluxation of tibia

Grade 3 PCL disruption - posterior tibia subluxed behind posterior aspect femoral condyles
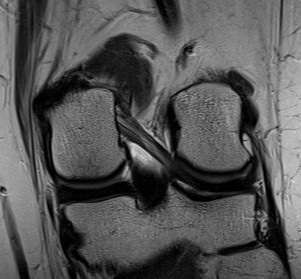
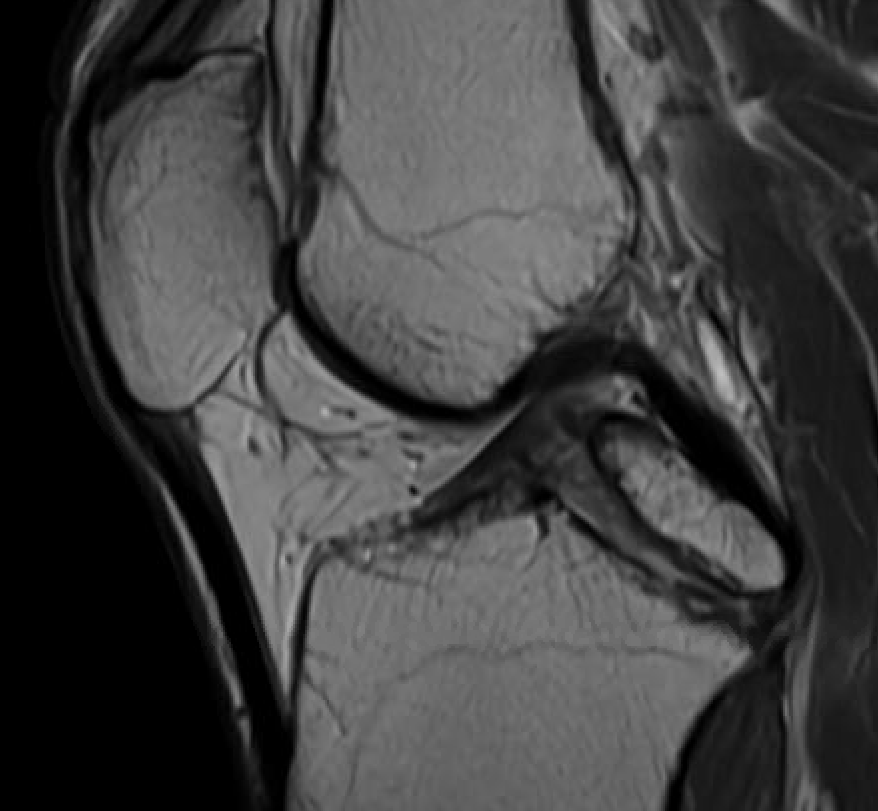
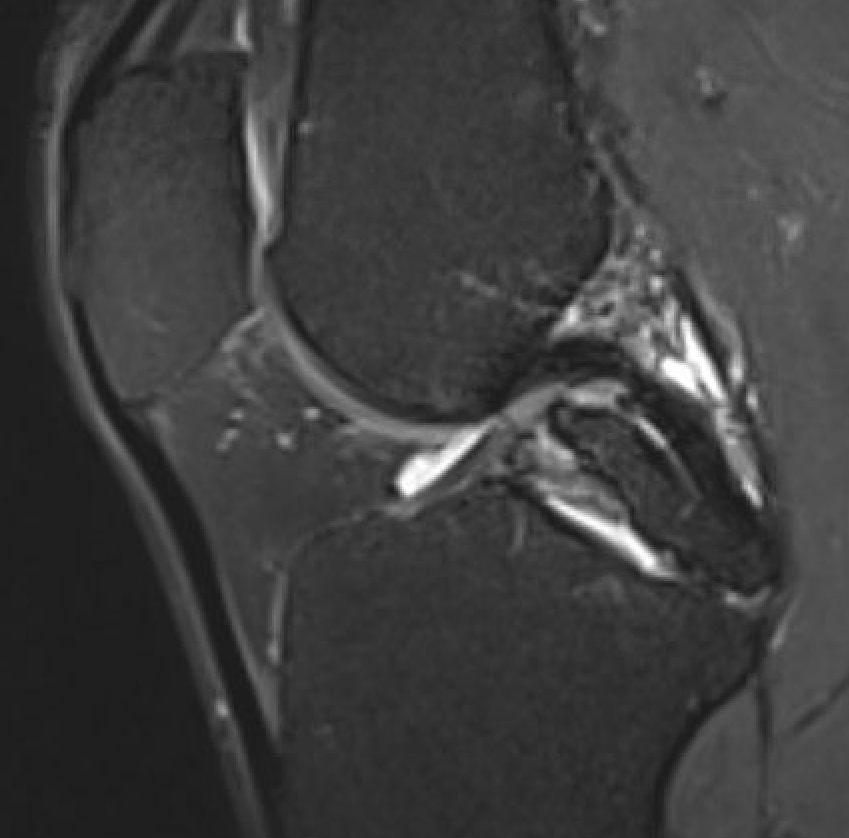
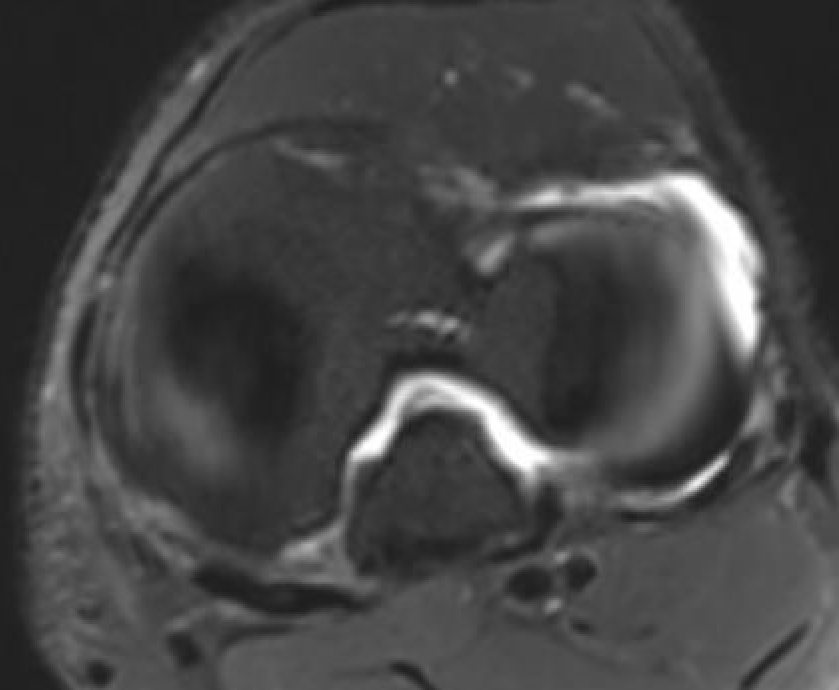
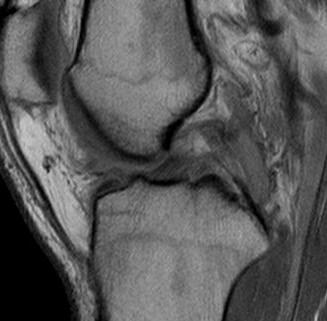
MRI
PCL completely torn

PCL midsubstance tear with lengthening
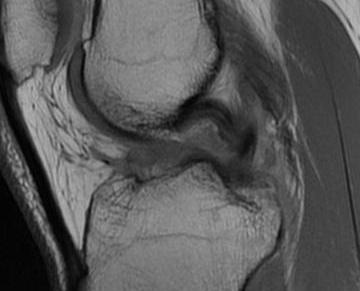
PCL tibial avulsion
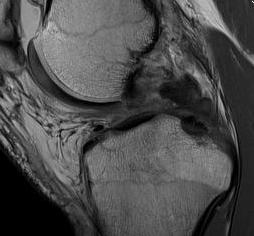
PCL femoral avulsion
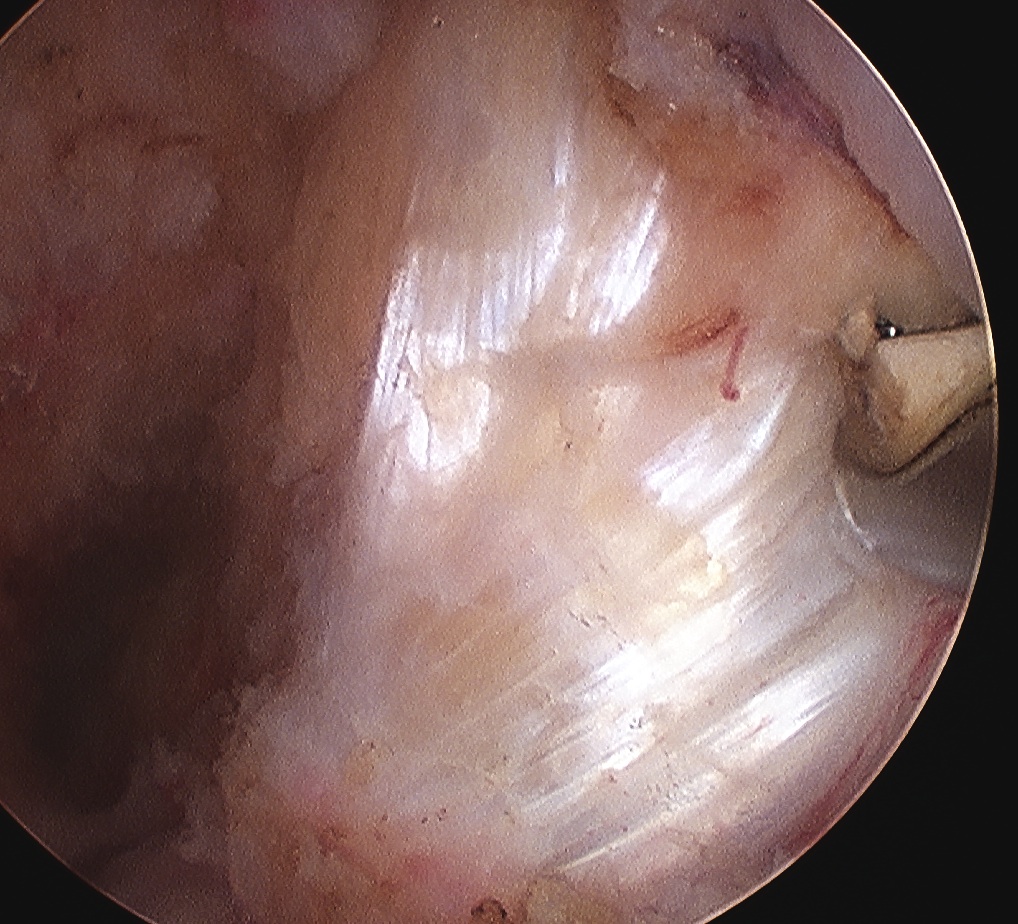
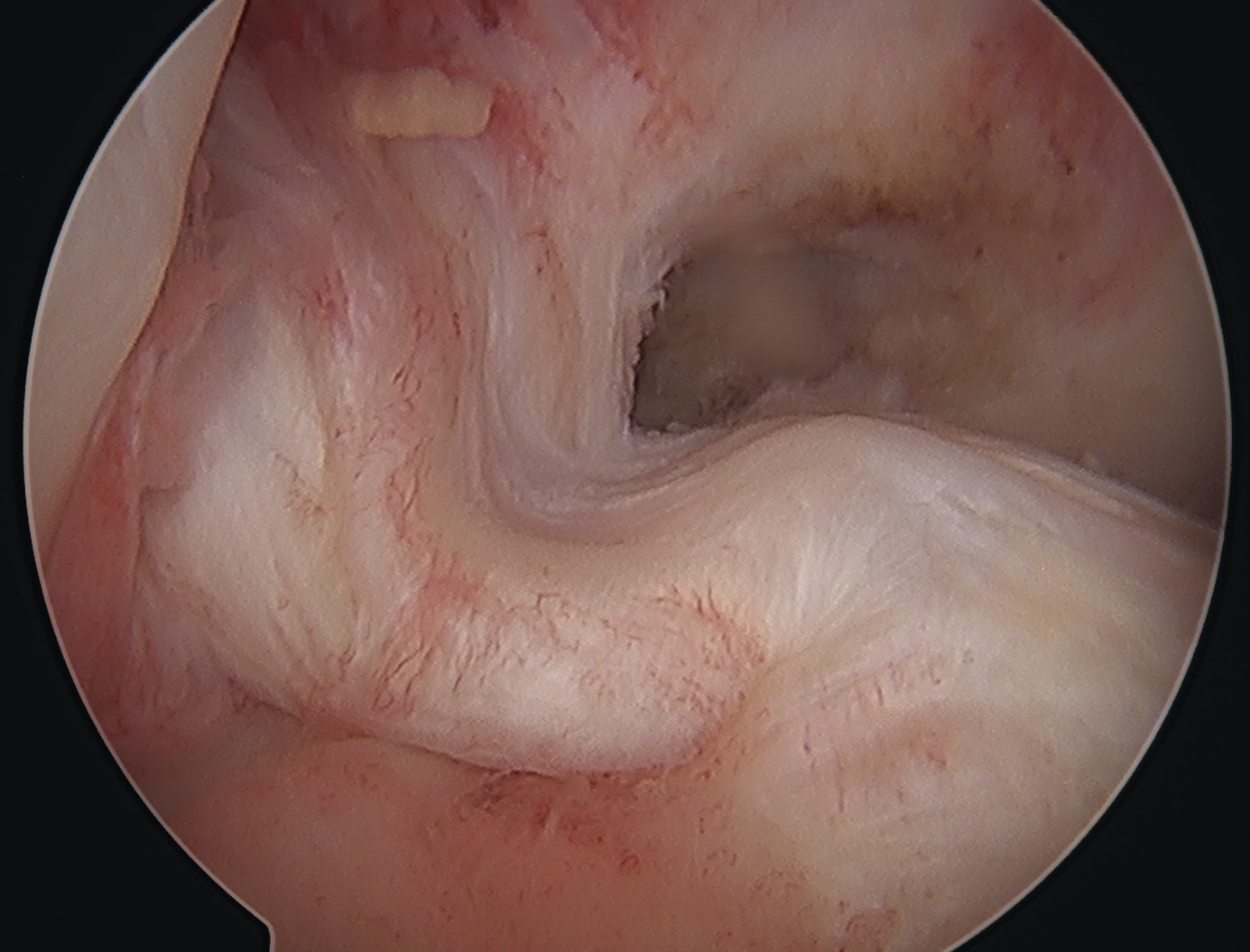
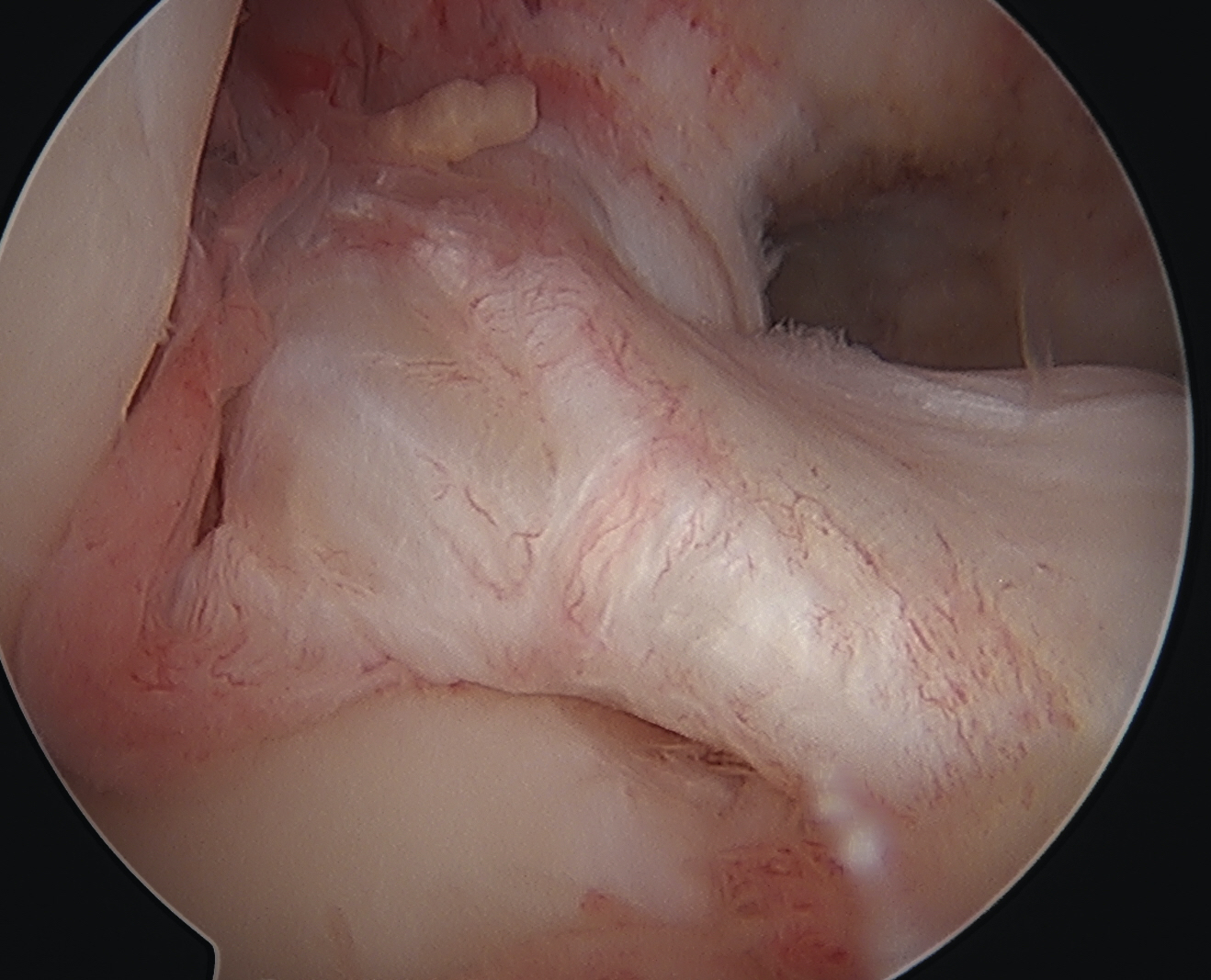
Arthroscopy
May miss tear as is extra-synovial
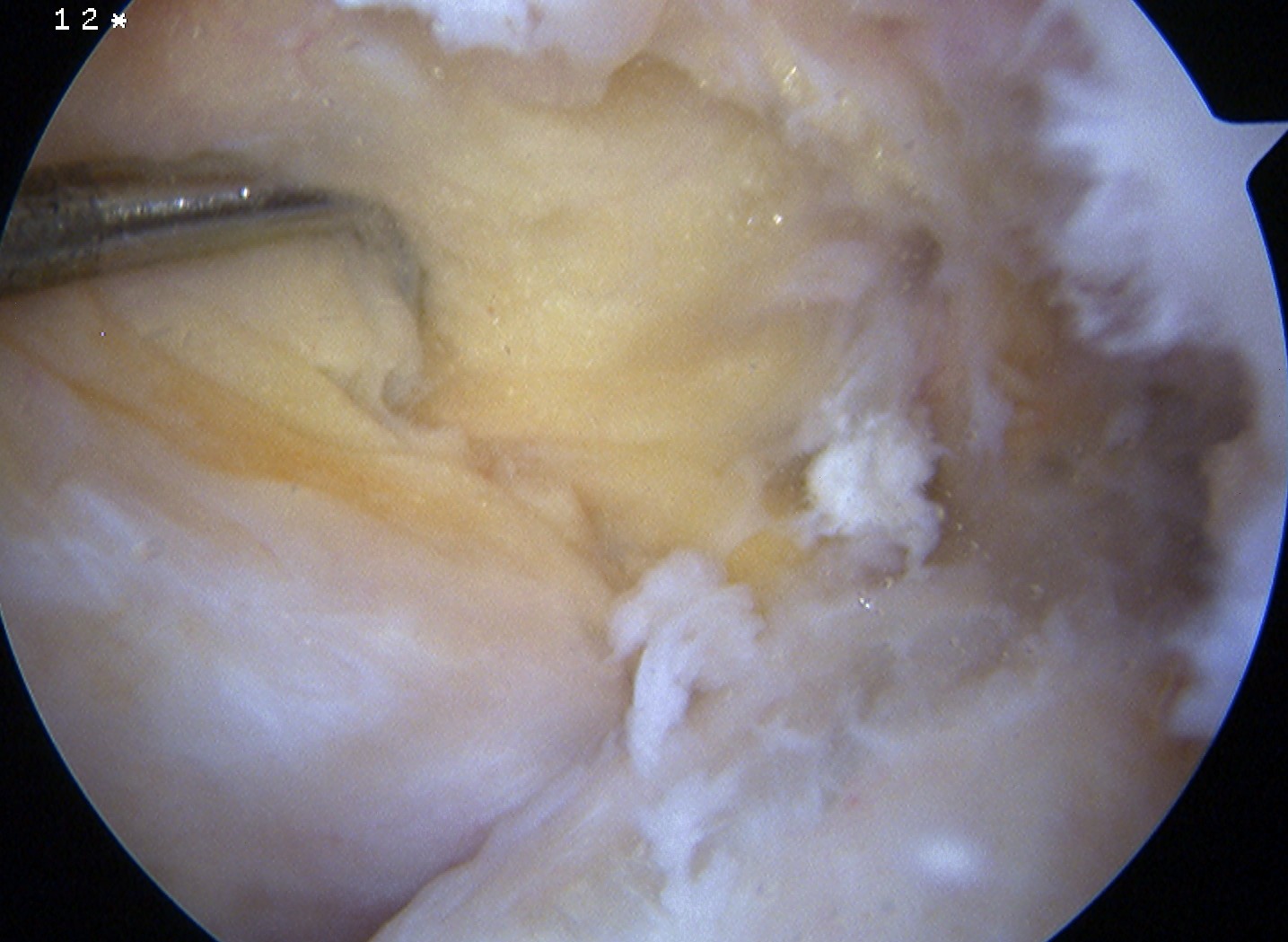
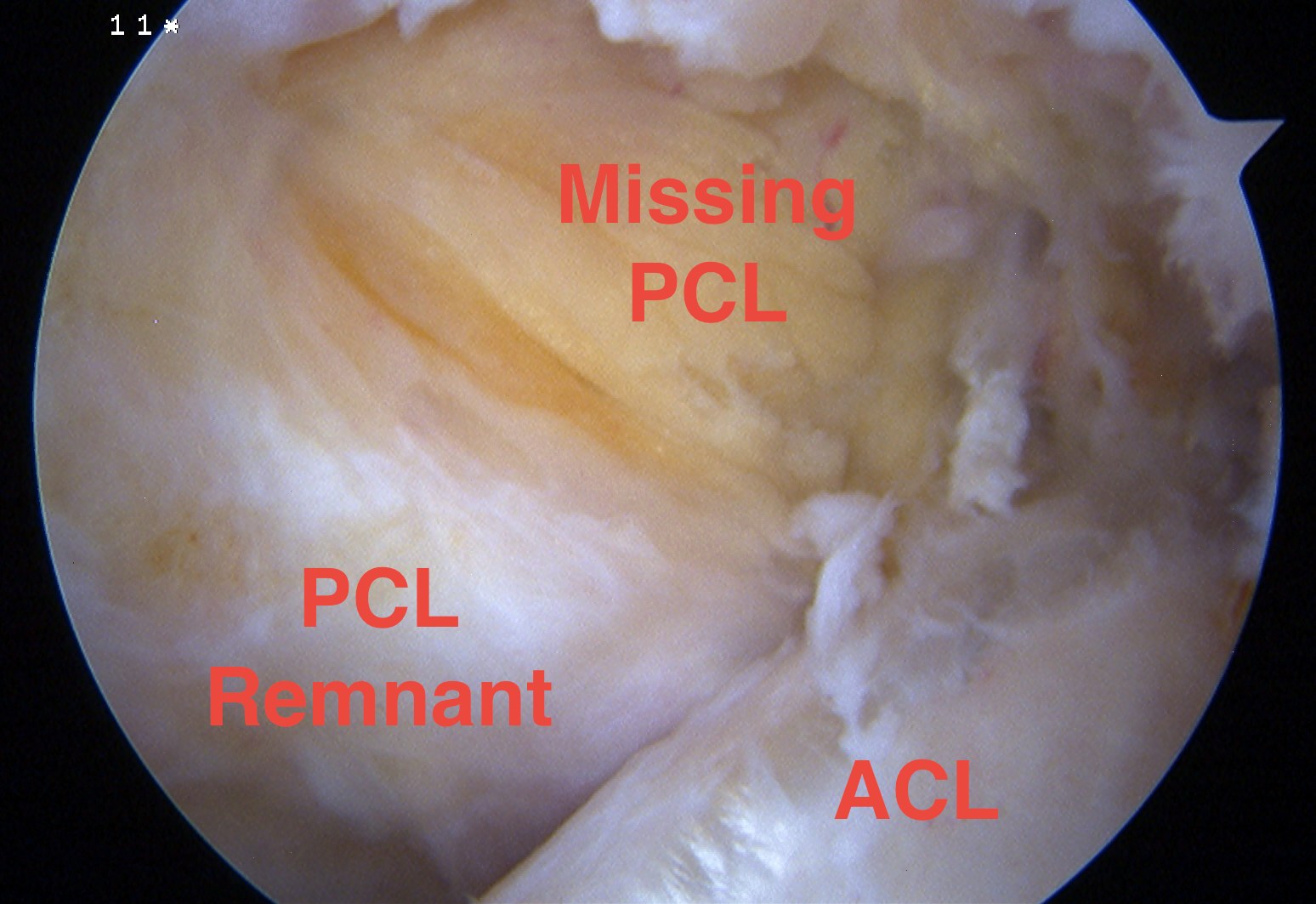
Chronic PCL tear from femur
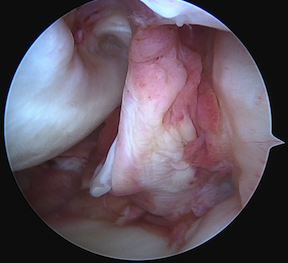
Acute PCL femoral avulsion
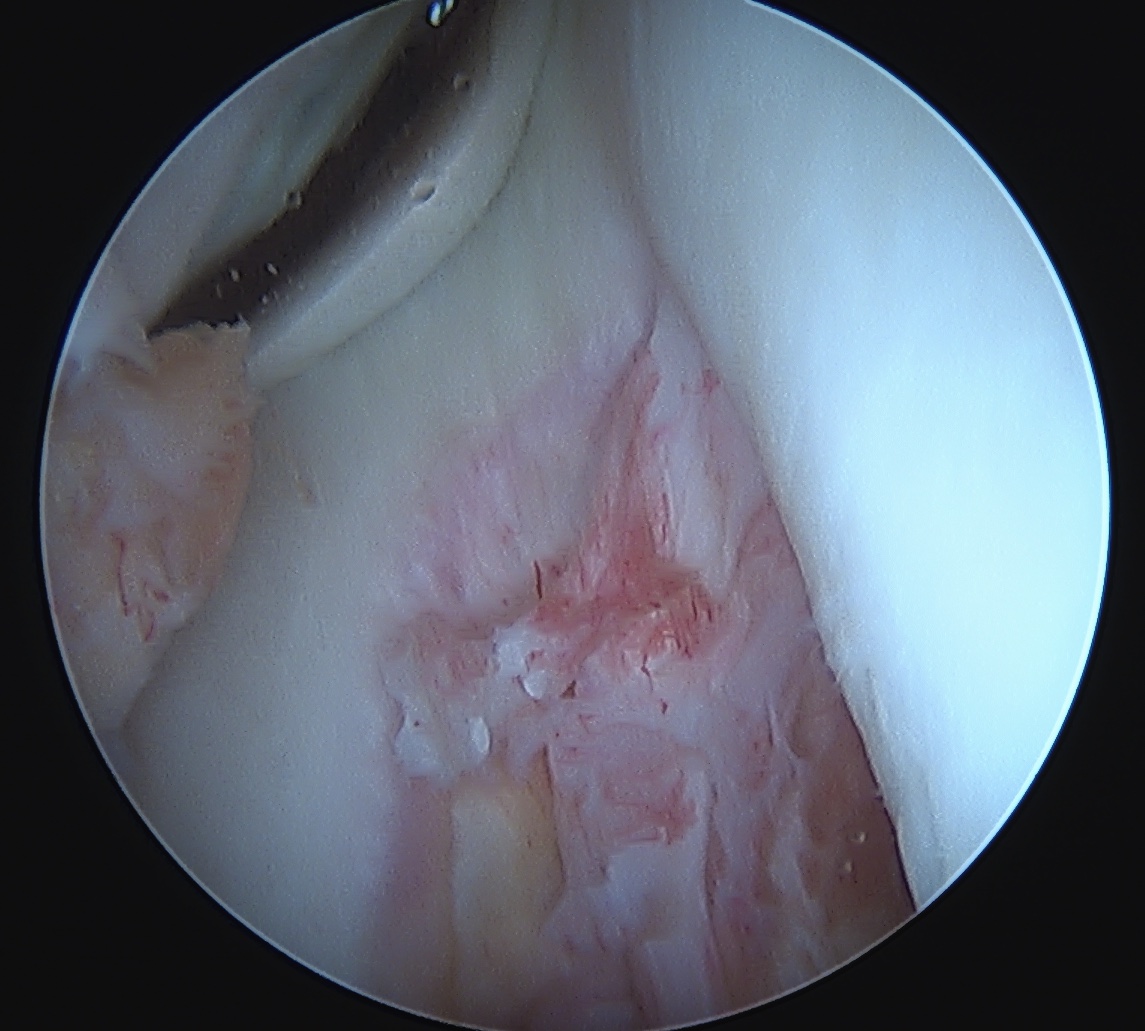
Apparent ACL laxity due to PCL tear and posterior tibial sag; ACL tension restored with anterior drawer