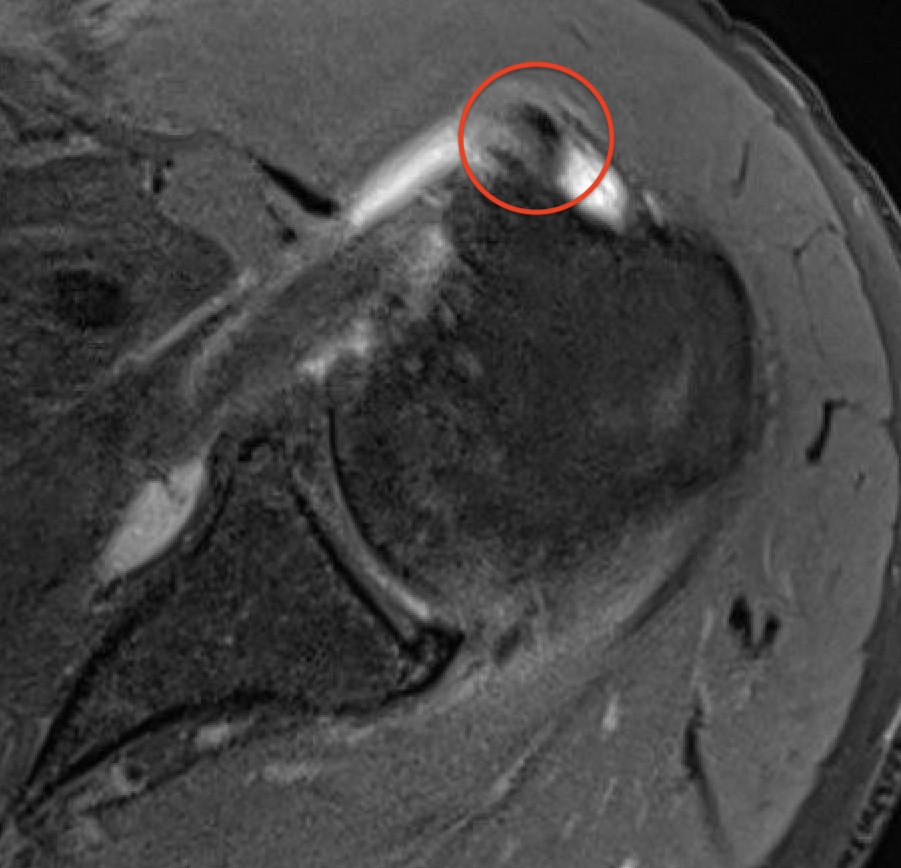
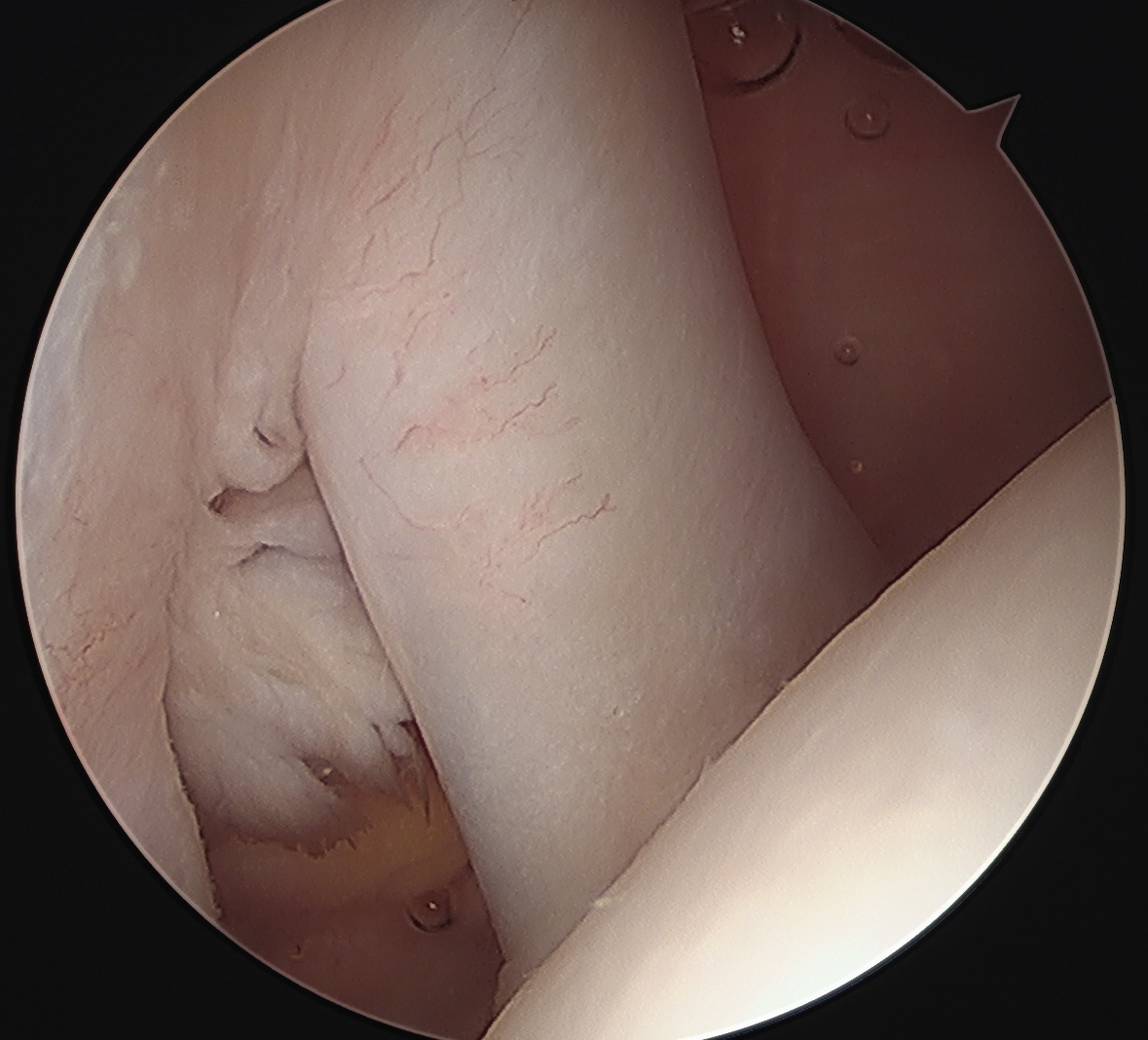
Medial subluxation of long head biceps
Definition
Medial subluxation of long head of biceps tendon out of groove and into rotator interval
Medial subluxation of long head of biceps tendon out of groove and into rotator interval



Early < 3 - 6 months
- most common


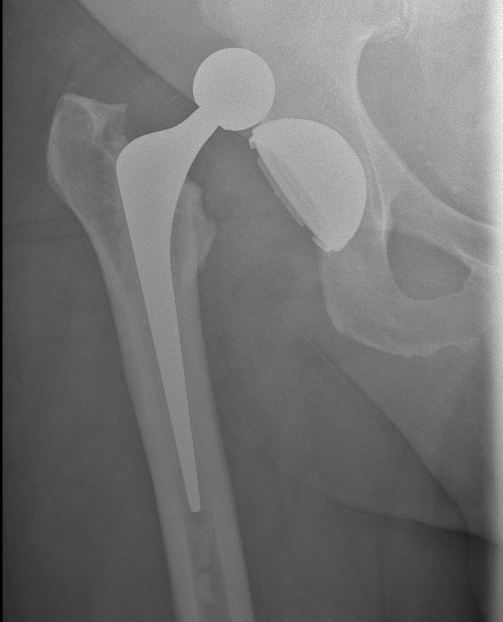
Stryker dual mobility
Prevent contractures
Prevent dislocations
Improve walking
Provide stable and painless sitting
Allow perineal care
Hip Dislocation
Adductor contractures
Flexion contractures
In-toeing
Windswept hips
Accepted that a dislocated hip in CP is painful
Deadly & rare
- usually post mortem
More common in children due to
- immature joints
- larger head to body ratio
- relative ligamentous laxity
High velocity trauma
- MVA
Mechanism
- hyperextension, distraction & rotation
Pure ligament injury usually
Facet joint dislocations secondary flexion distraction injury
10%
1. Unifacet subluxation - interspinous process widening
2. Unifacet dislocation - 25% anterolisthesis
3. Bifacet dislocation - 50% anterolisthesis
4. Complete vertebral translation - 100% anterolisthesis
Uncommon
- dancers
- athletes
Hyperdorsiflexion of the MTPJ
MT head dislocates plantar
- may buttonhole through capsule
- can prevent closed reduction
1. Sesamoids
2. Conjoint tendon
3. Intersesamoid Ligament
1. AP Instability
2. Varus Valgus Instability
3. Global Instability
4. Frank Dislocation