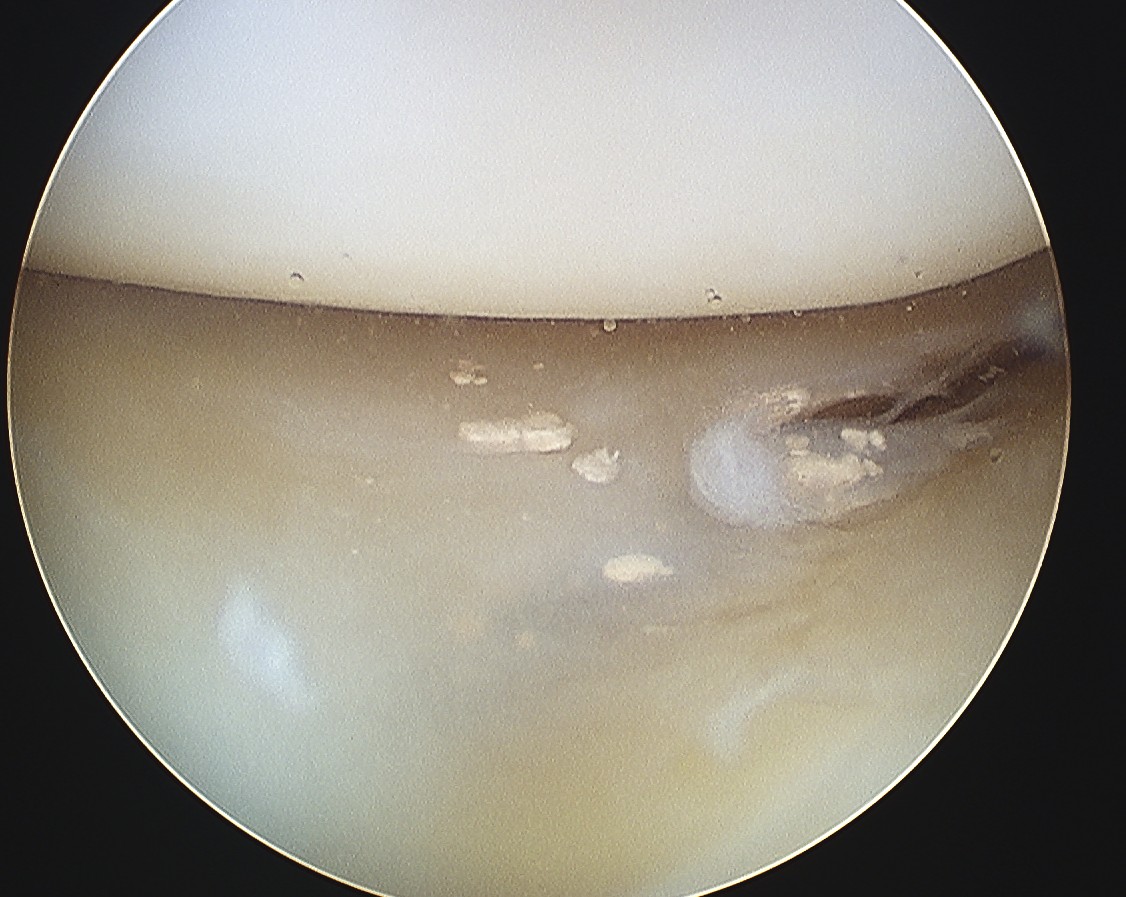
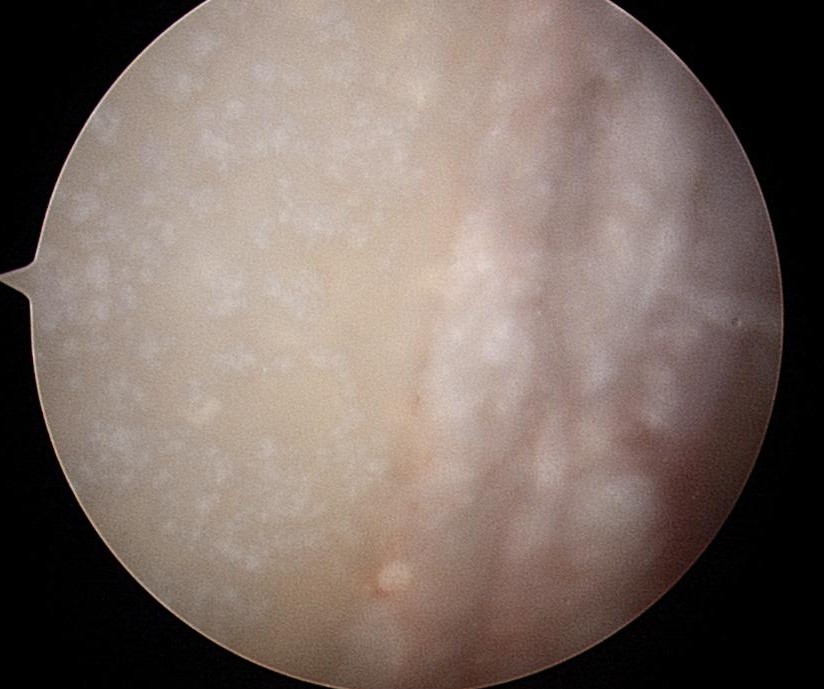
Avascular necrosis
Epidemiology
Much less common than hip OA
- usually presents late
Aetiology
Similar causes as hip (AS IT GRIPS 3C)
Alcohol / Steroid / Trauma / Idiopathic
Gauchers
RA / RTx
Sickle Cell

Much less common than hip OA
- usually presents late
Similar causes as hip (AS IT GRIPS 3C)
Alcohol / Steroid / Trauma / Idiopathic
Gauchers
RA / RTx
Sickle Cell
Deformity characterised by
- dorsiflexion of calcaneus
- plantarflexion of forefoot / plantaris / forefoot equinus
Both sides of foot have elevated arch
Weakness of triceps surae
- polio - most common worldwide
- spina bifida
1 year: Bow legs / 15° varus
2 year: Neutral
3 year: Knock knees / 10° valgus

6 year: Physiological valgus / 6° valgus
Joint inflammation secondary pyogenic organism
All age groups
Usually children
- 50% < age 3
M= F
Any joint
- Infants = Hip
- Children = Knee
- Adults = Large Joints
IVDU - SCJ & SIJ
Two Routes

Heterogeneous group of diseases characterised by
- hyperuricaemia
- recurrent attacks of acute arthritis
Diagnosis confirmed by
- crystals of Monosodium Urate in synovial fluid
- tophi ("Porous stone") urate in soft tissues
- renal urate stones
Adult men
Pseudogout
- Calcium Pyrophosphate Dihydrate (CPPD) crystals
- inflammatory arthritis of older individuals
Pain at attachment of thickened central part of plantar aponeurosis to Medial Calcaneal Tuberosity
Origin
- medial calcaneal tuberosity
Inserts
- 5 bands superfical & deep layers
Superficial
- insert transverse MT ligament & skin
Deep
- flexor sheath, volar plate & periosteum of P1
Acquired Adult Flatfoot Deformity (AAFD)
- collapse of medial longitudinal arch
- secondary to ligament / tendon / joint or bony pathology
Flexible / Physiological
Ligamentous Laxity (DIAL HOME)
Rigid
- Congenital Vertical Talus
- Tarsal Coalition
Pure Cavus Deformity characterised by
- dorsiflexion of Calcaneus
- plantarflexion of Forefoot
Weakness of Tendoachilles
Usually neuromuscular
- Polio (Most common worldwide)
- Spina bifida
- CP (can be due to overcorrection of T Ach)
- Spinocerebellar Degen (Friedreich's Ataxia)
Lateral compartment of leg
- run through retromalleolar groove
- pass superior and inferior to peroneal tubercle
- covered by inferior peroneal retinaculum
Peroneus longus
- origin lateral condyle of tibia and head fibula
- tendon PL superficial and inferior to brevis in retromalleolar groove
- runs in cuboid groove
- insert plantar surface base of 1st MT and lateral aspect medial cuneiform