Instability
Types of Instability
1. AP Instability
2. Varus Valgus Instability
3. Global Instability
4. Frank Dislocation
1. AP Instability
2. Varus Valgus Instability
3. Global Instability
4. Frank Dislocation
Usually occurs in patients over 60
- due to decreased vascularity & collagen weakness
Younger patient on steroids / growth hormone
Occasionally occurs in young athlete with excessive contracture
Often preceded by quadriceps tendinosis
Direct blow
- most common
Indirect
- forced knee flexion with foot fixed / maximally contracted quadriceps
1. Vertical

2. Transverse

1. Loosening
2. Infection
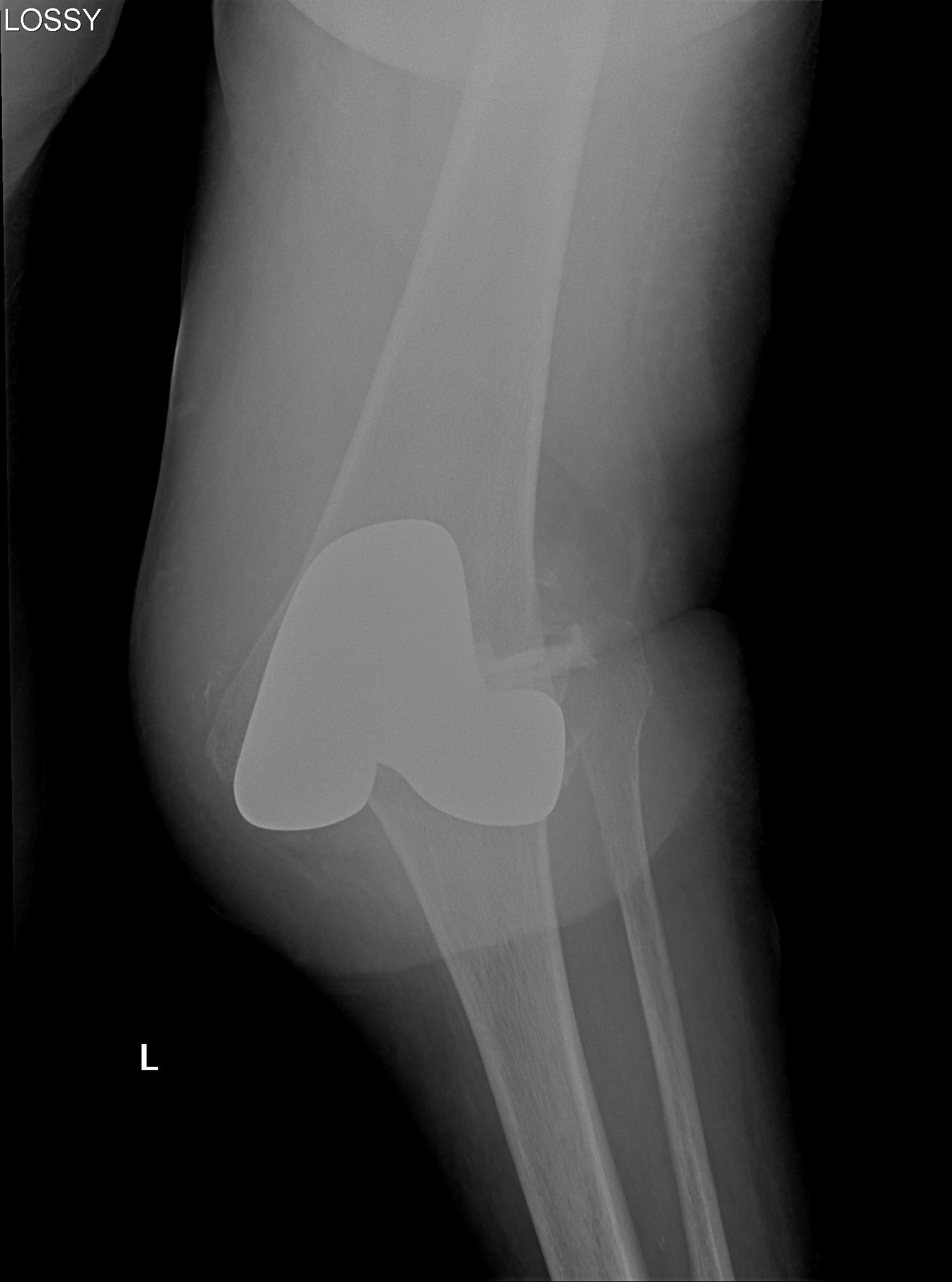
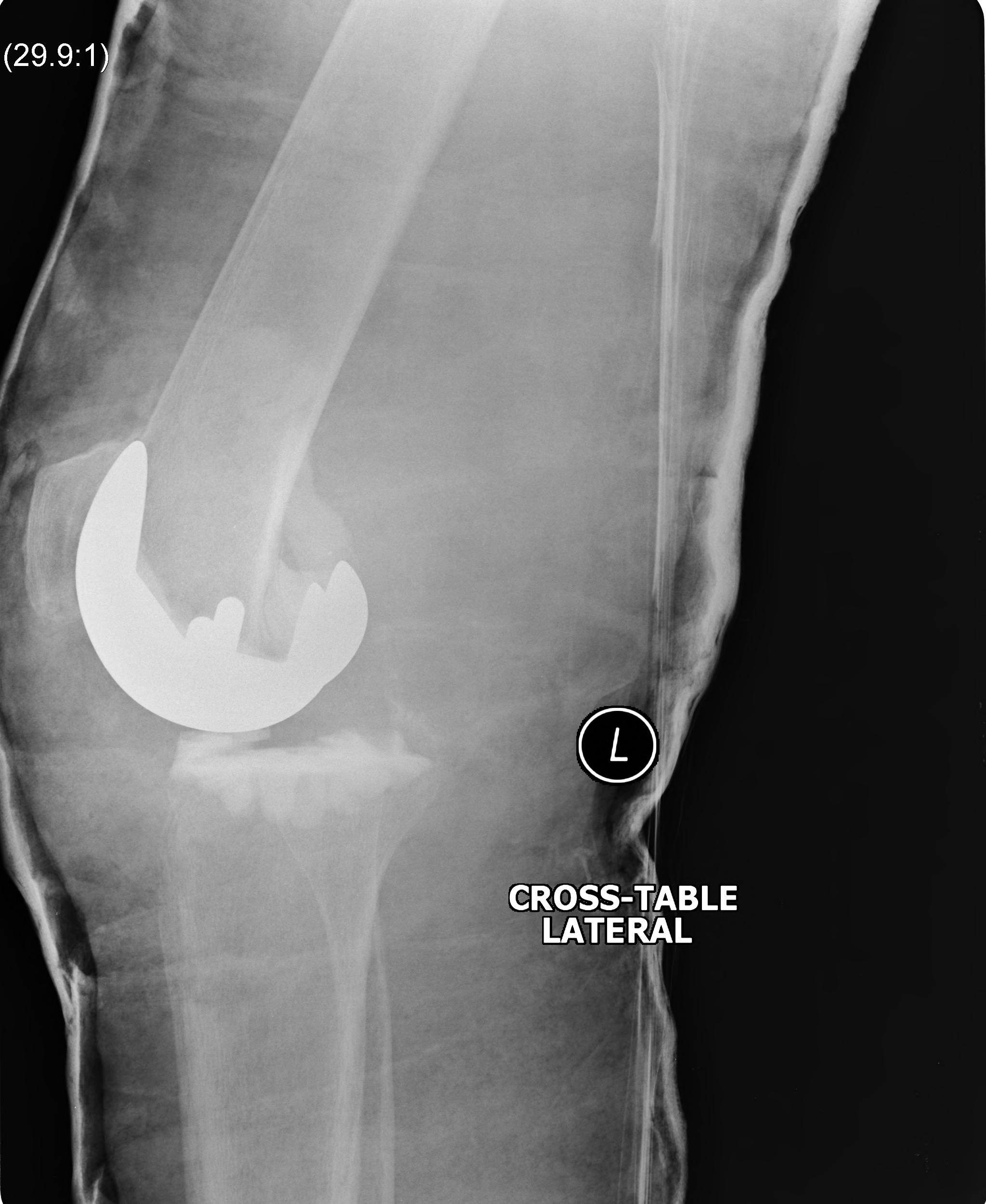
3. Instability
4. Periprosthetic fracture
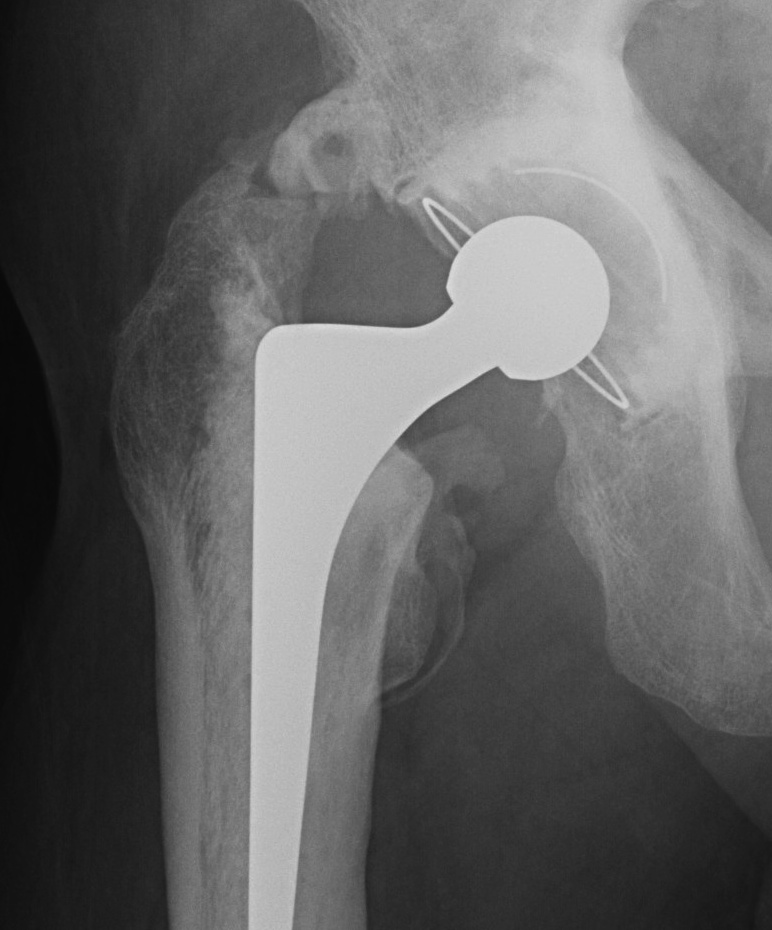
5-15% of posterior dislocations
Posterior hip dislocation
Type I - head fracture below fovea
Undisplaced
- non operative
Displaced
- excise fragment if small
- ORIF fragment if large (can contribute to instability)


Rheumatoid arthritis

Combined ankle and subtalar joint osteoarthritis
Calcification
- central pattern
- often increased opacity compared with bone
Ossification
- peripheral pattern
- similar density to bone

Pathological bone formation in soft tissues
In elbow
- 3% of trauma
- 89% if head injury + trauma
Completely different
1. Myosisitis Ossificans Circumscripta
- post traumatic
- more common
- recognised as a consequence of neurological injury
Multi-ligament knee injury (MLKI)
- 2 or more ligaments disrupted
Knee dislocation
- ACL + PCL + one of collaterals
High energy (MVA)
Low energy (sport)
- low energy has 5% arterial injury
Pigmented Villo-Nodular Synovitis
- benign inflammatory process that arises in synovial tissues
- contains significant amounts of hemosiderin
Age: 20 - 50
Sex: M > F
A. Diffuse
- throughout joint synovium
- more difficult to treat / excise fully