Epidemiology
Usually occurs in patients over 60
- due to decreased vascularity & collagen weakness
Younger patient on steroids / growth hormone
Occasionally occurs in young athlete with excessive contracture
Aetiology
Often preceded by quadriceps tendinosis

Location
1. Avulsion of quadriceps tendon from superior patella
2. Rupture of belly of rectus femoris
3. Rupture at musclulotendinous junction in athletes
Clinical


Palpable gap in tendon
Haemarthrosis
Extensor lag
- function usually good if tear incomplete

Diagnosis can be missed once acute features settle
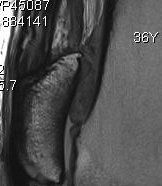
Xray
Patella Baja

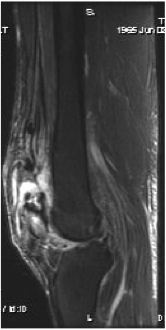
MRI

Management
Options
Incomplete
- immobilise for 4/52 in extension
- then rehabilitate


Complete
- surgical repair
Athlete
- surgical repair
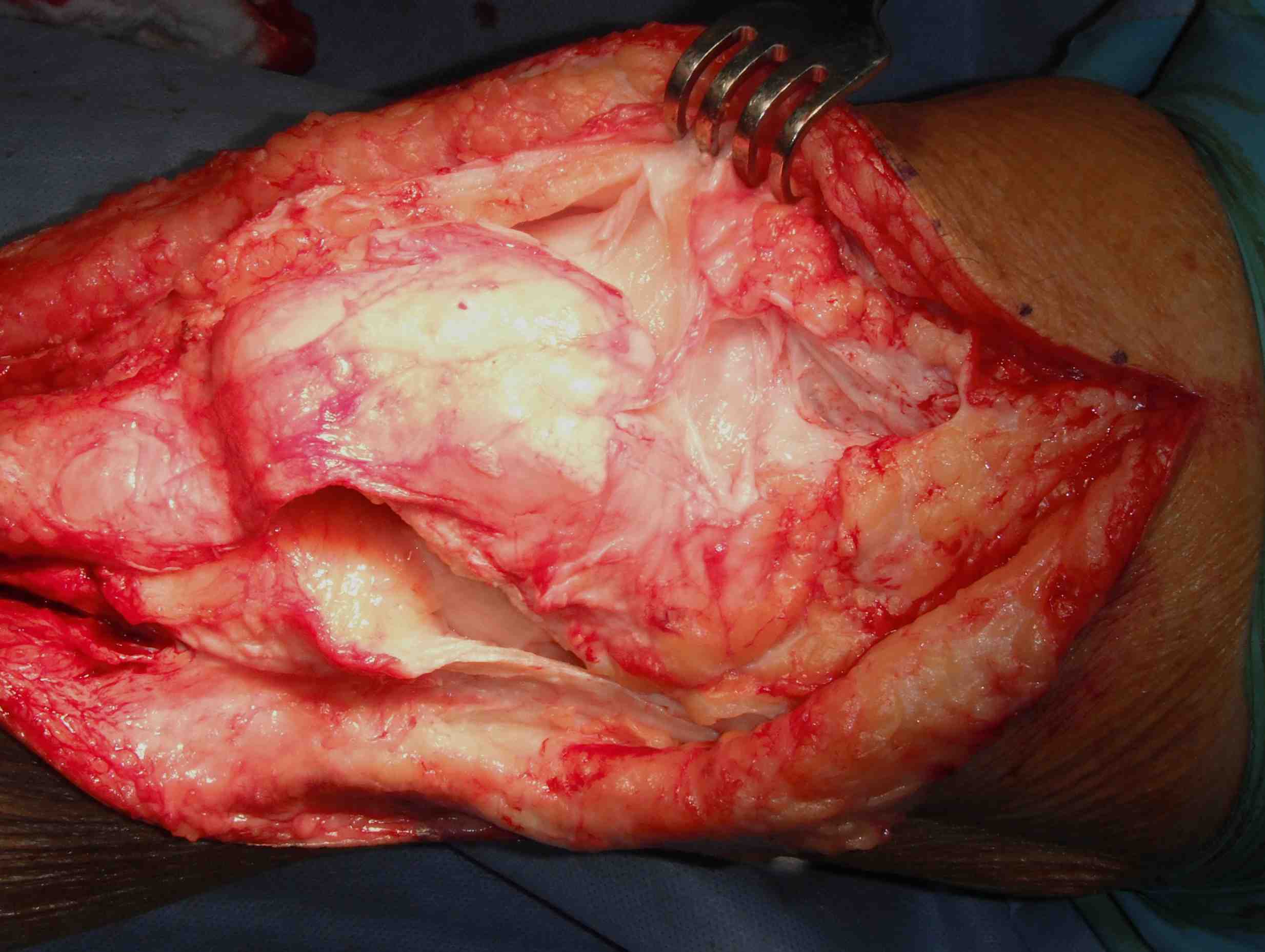
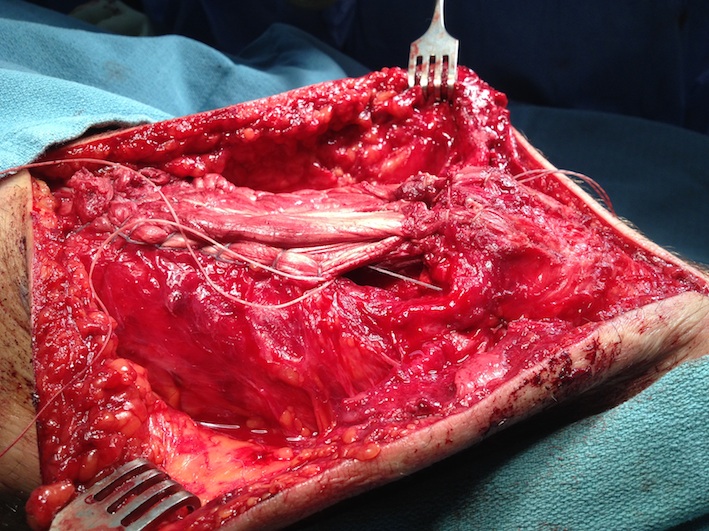
Surgical Technique
Position
- patient supine
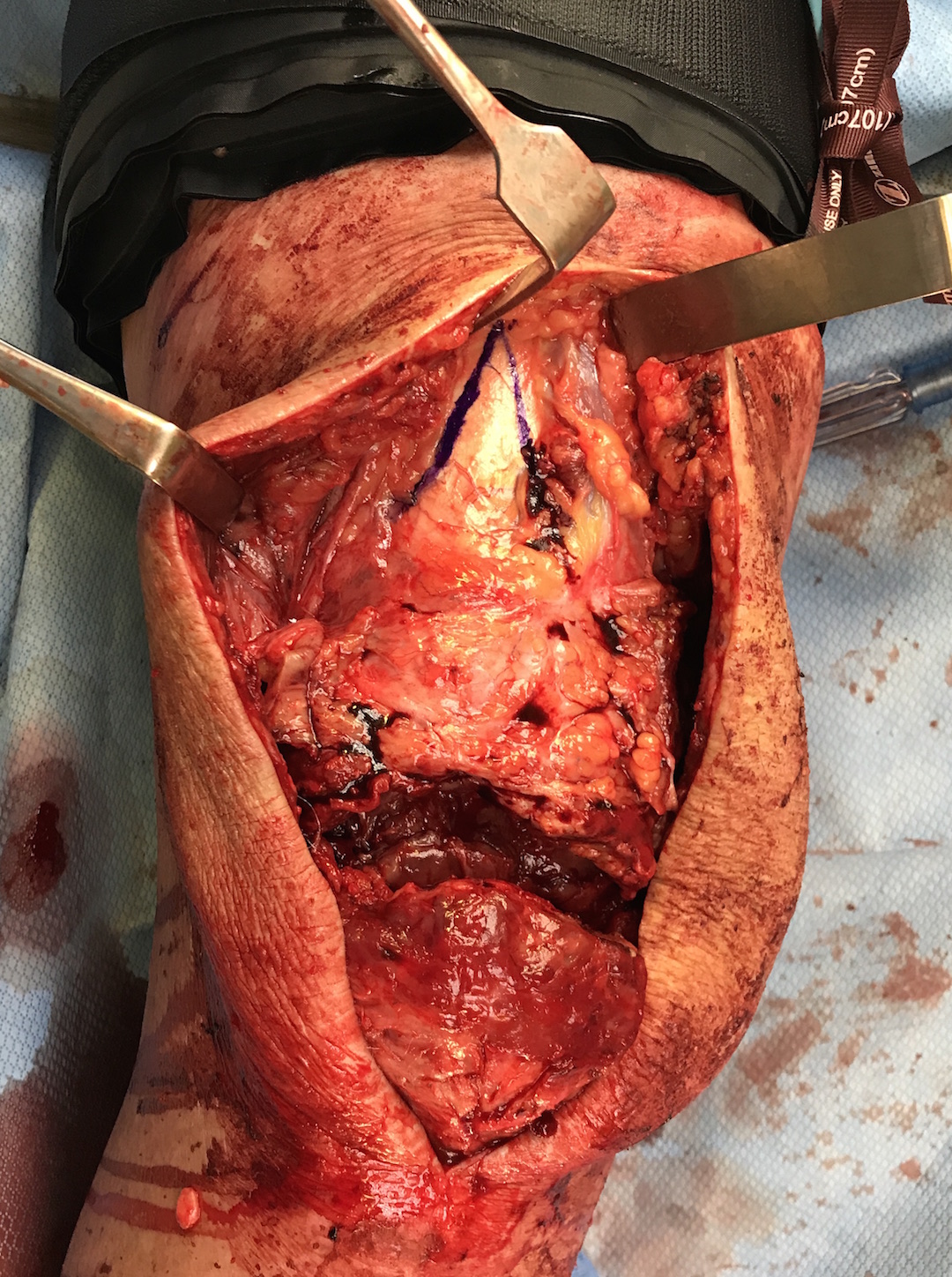
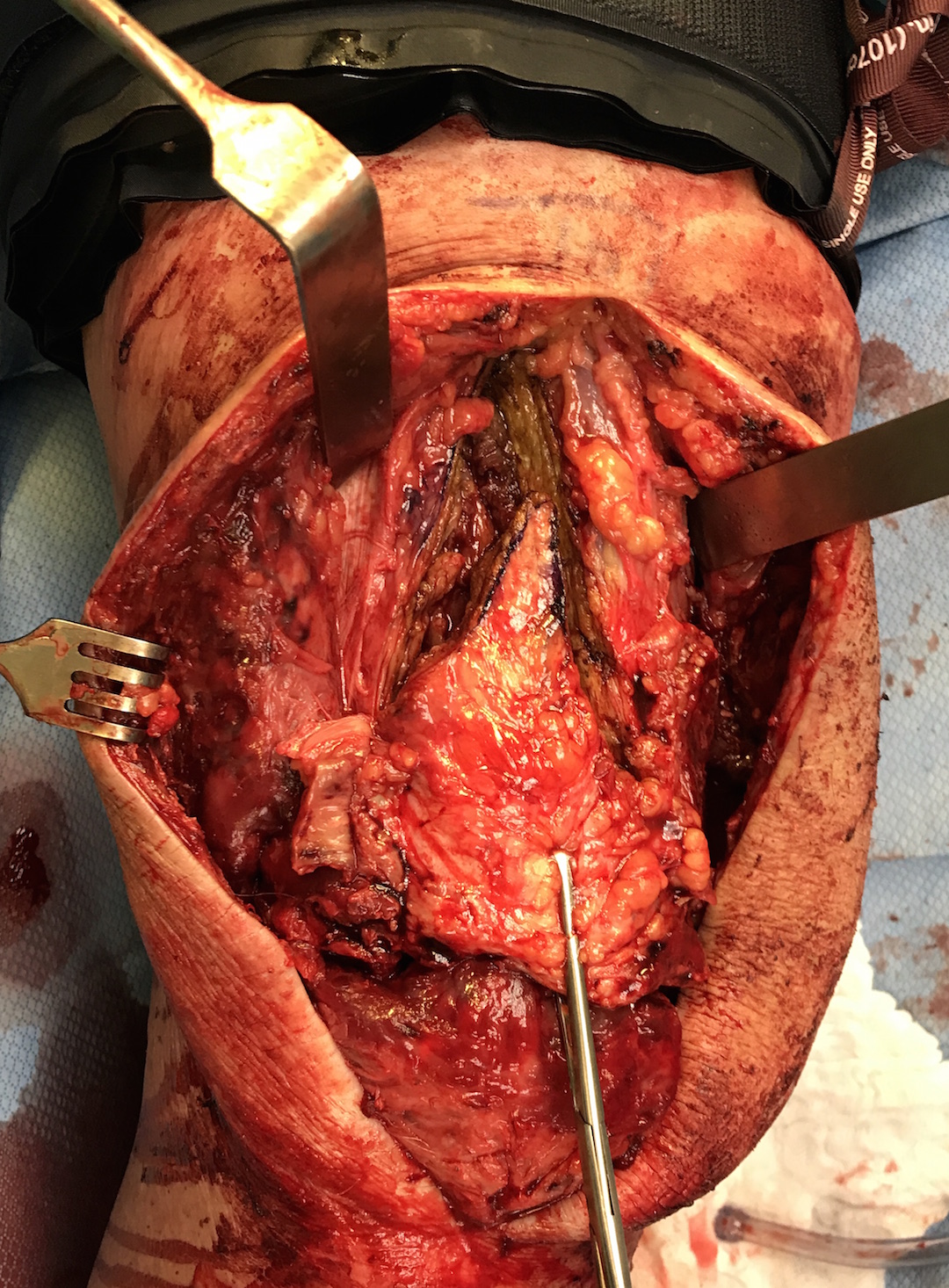
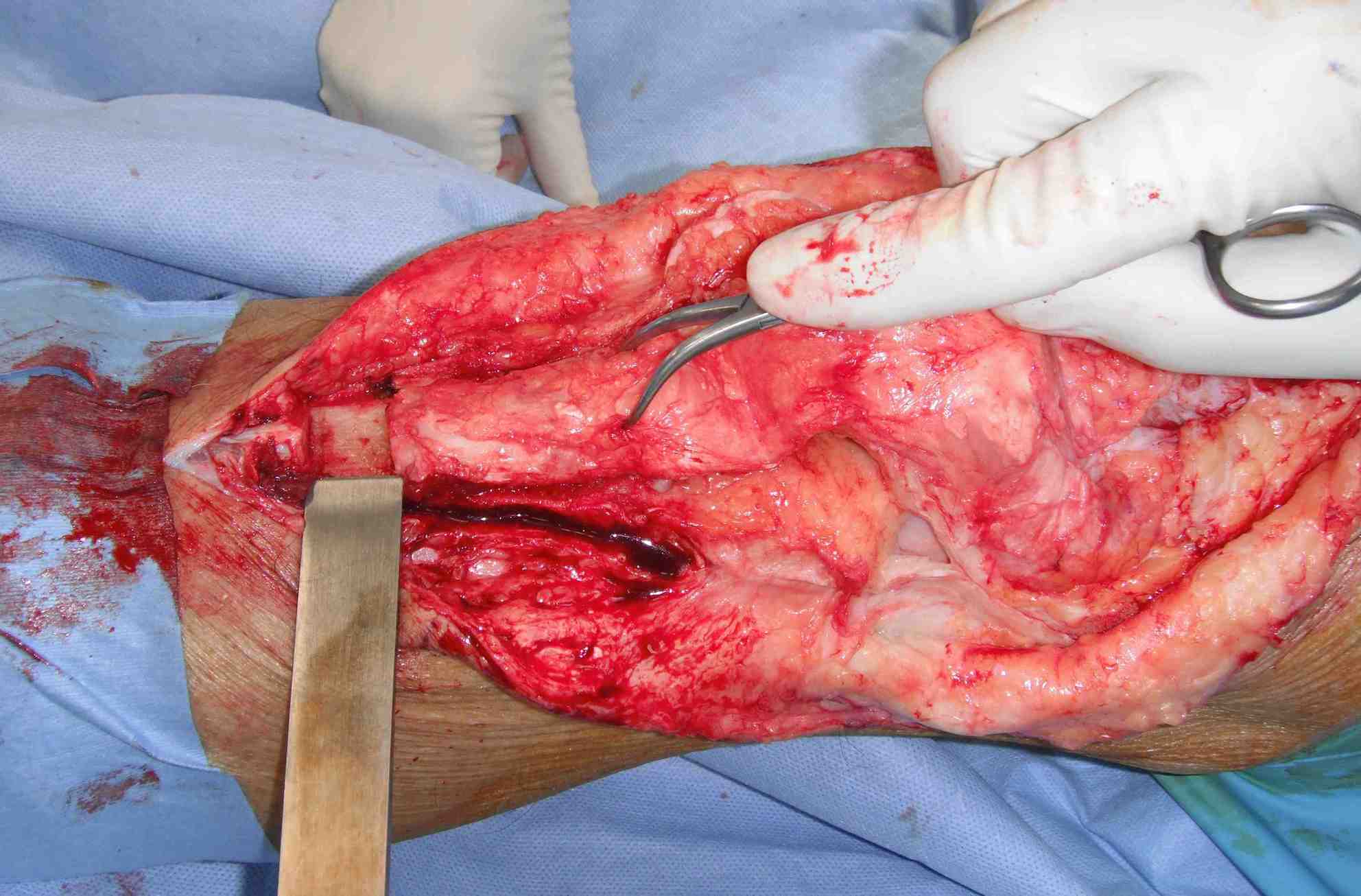
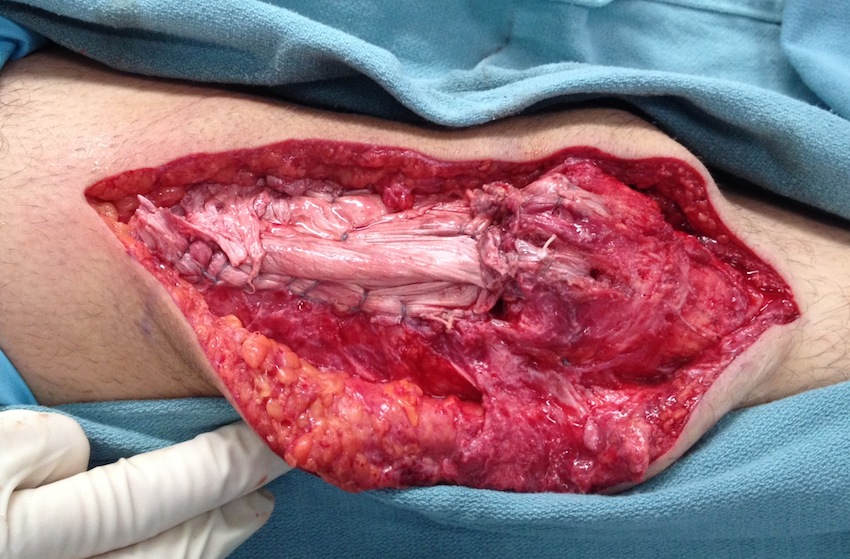
Midline incision
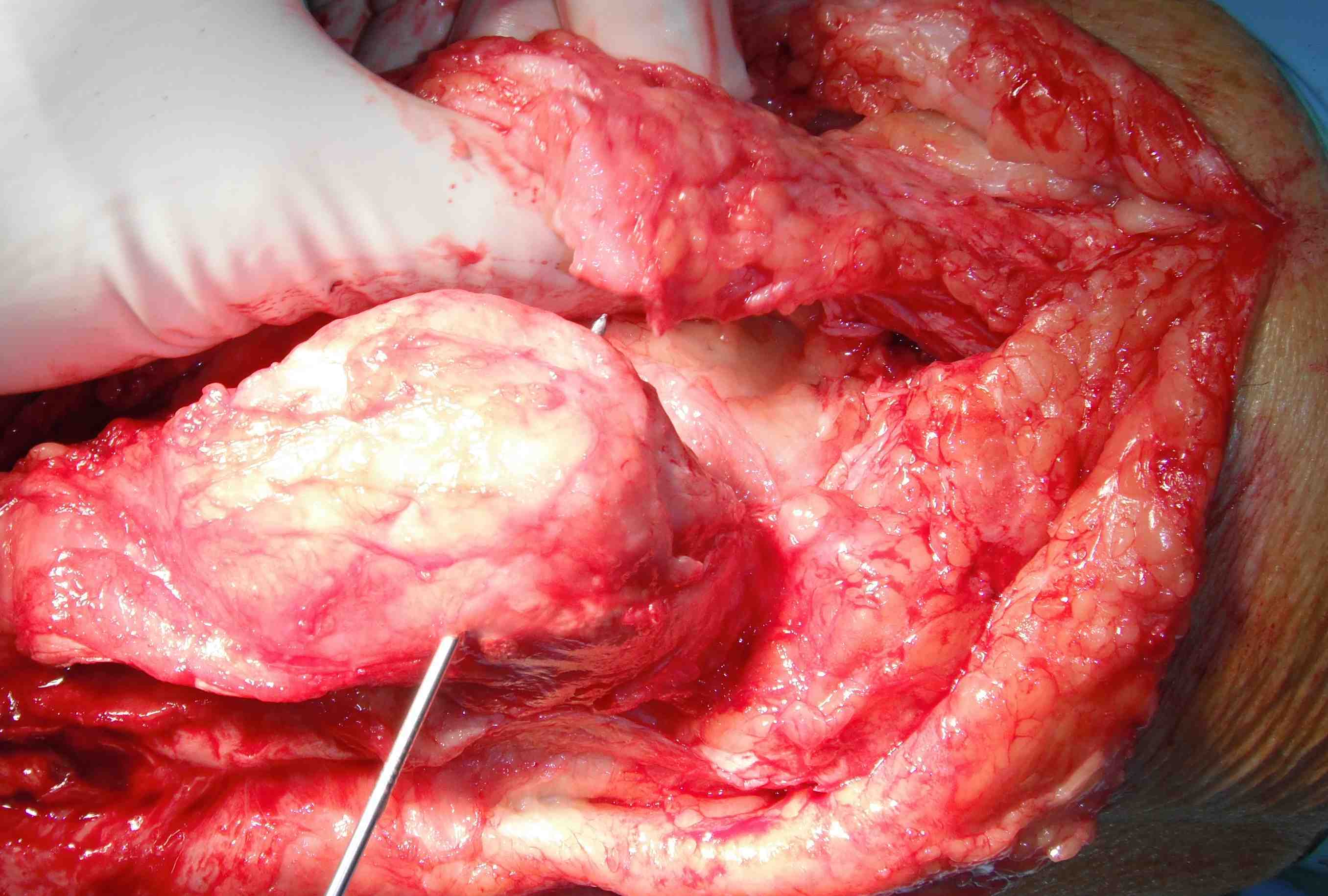
- expose quadriceps
- mobilise tendon / release from subcutaneous tissue
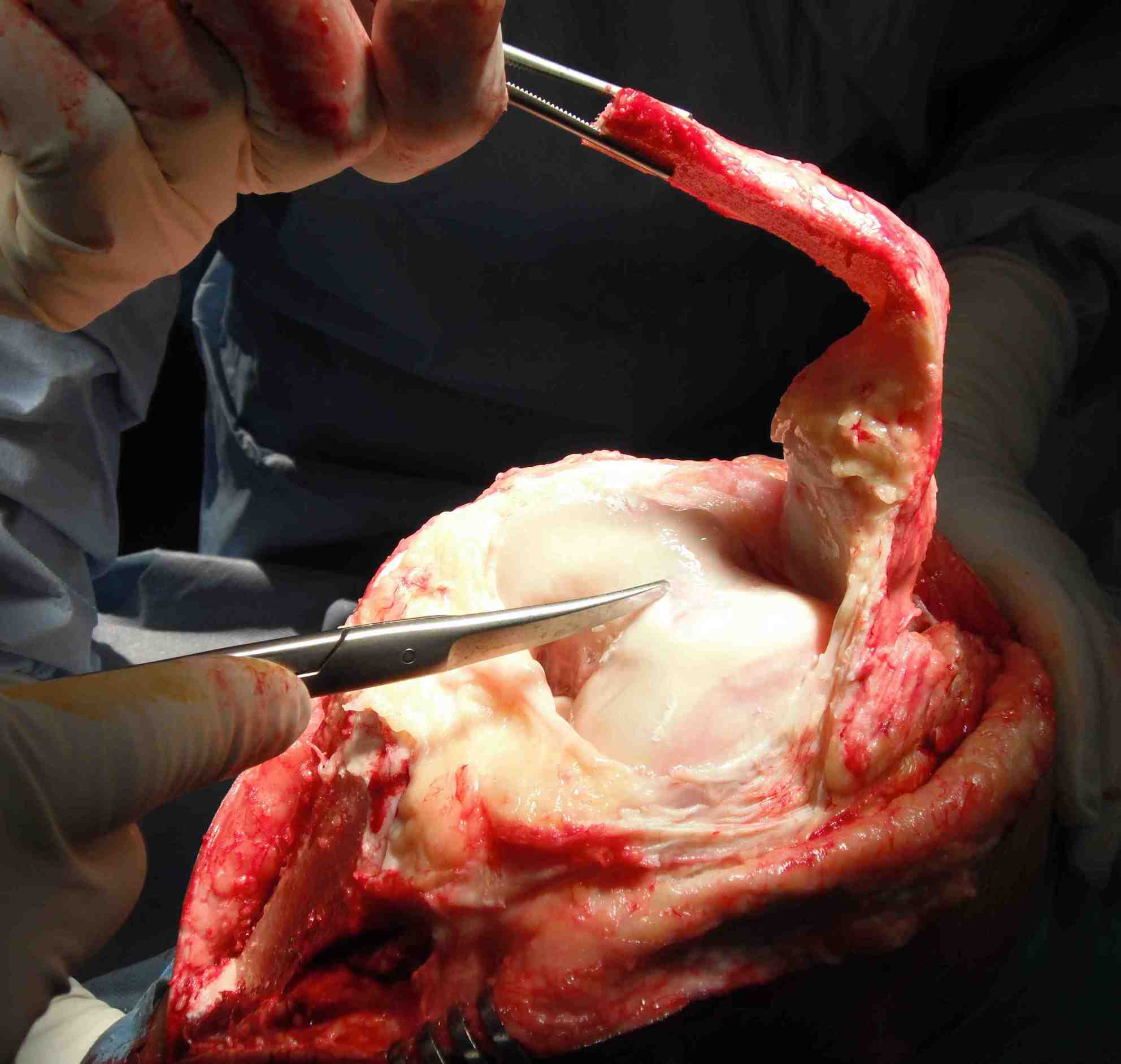
- debride insertion on patella
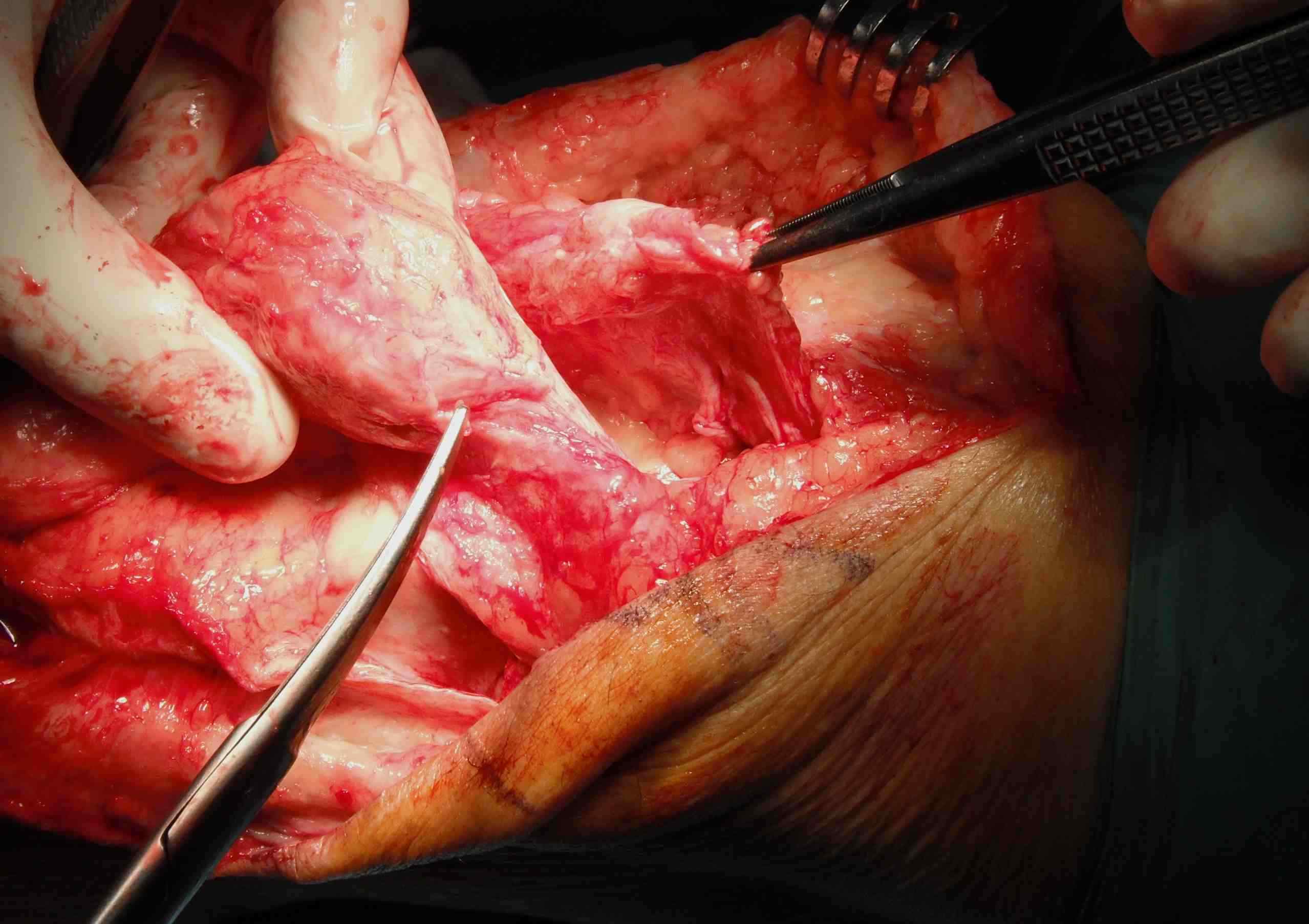
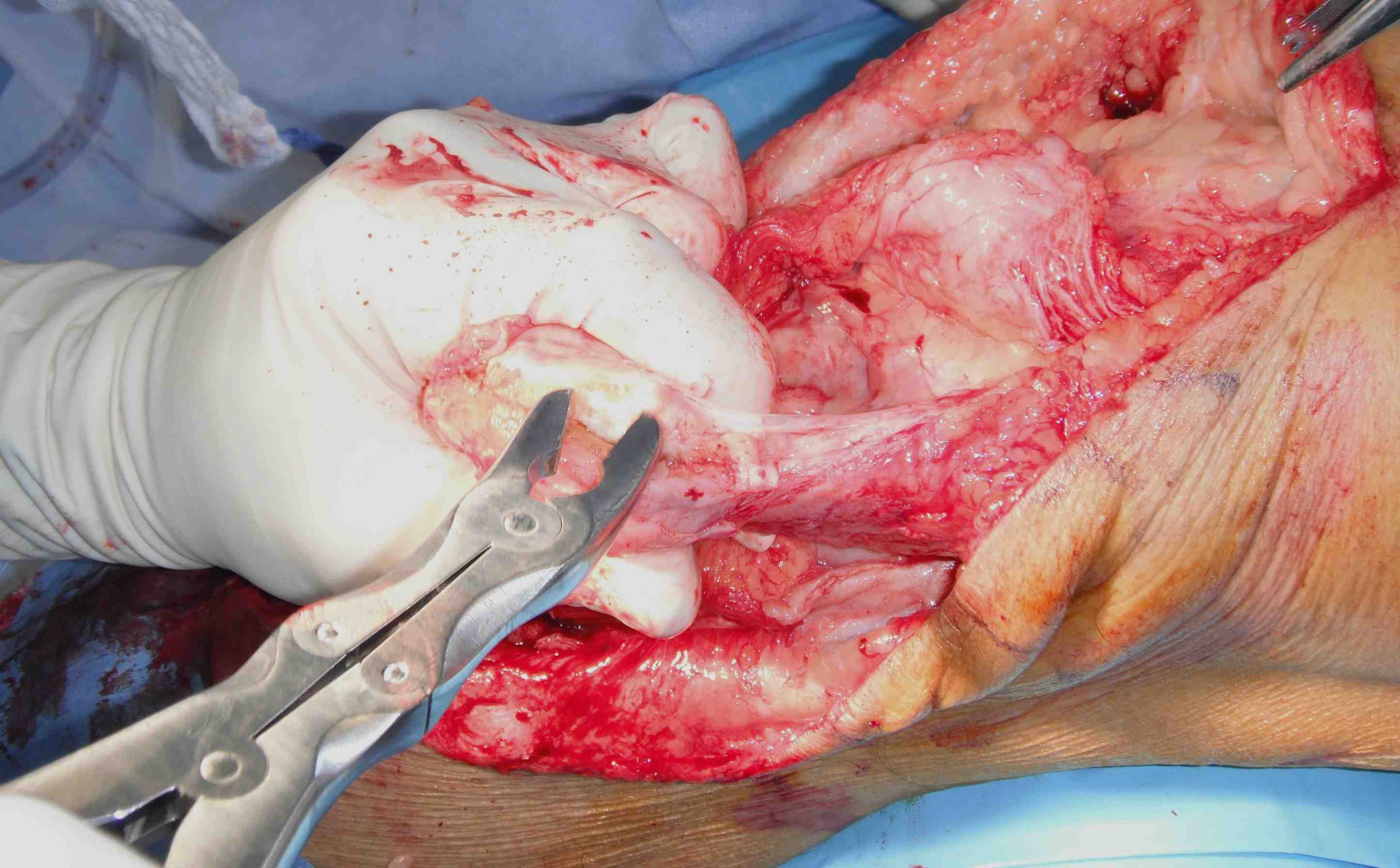
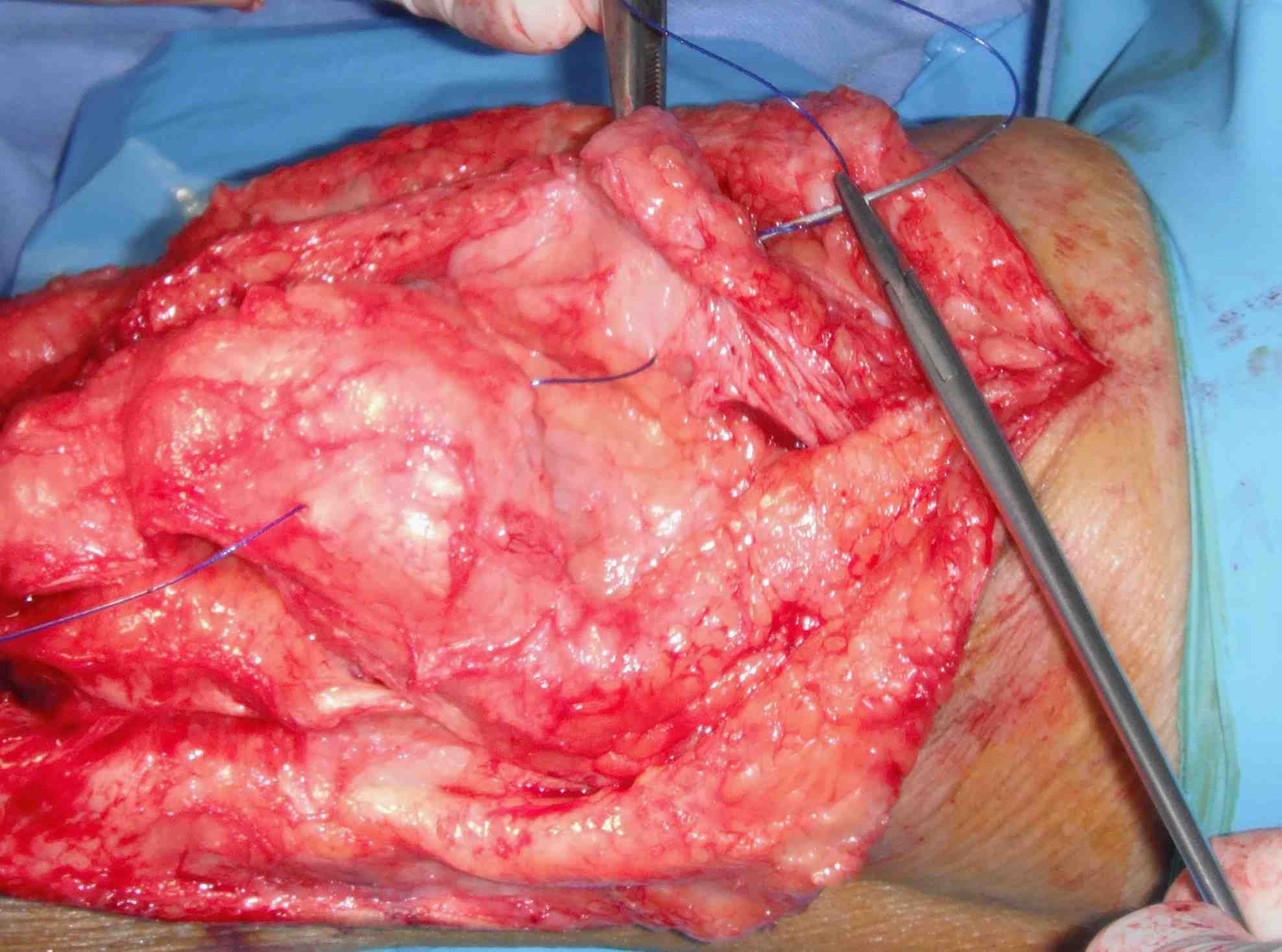
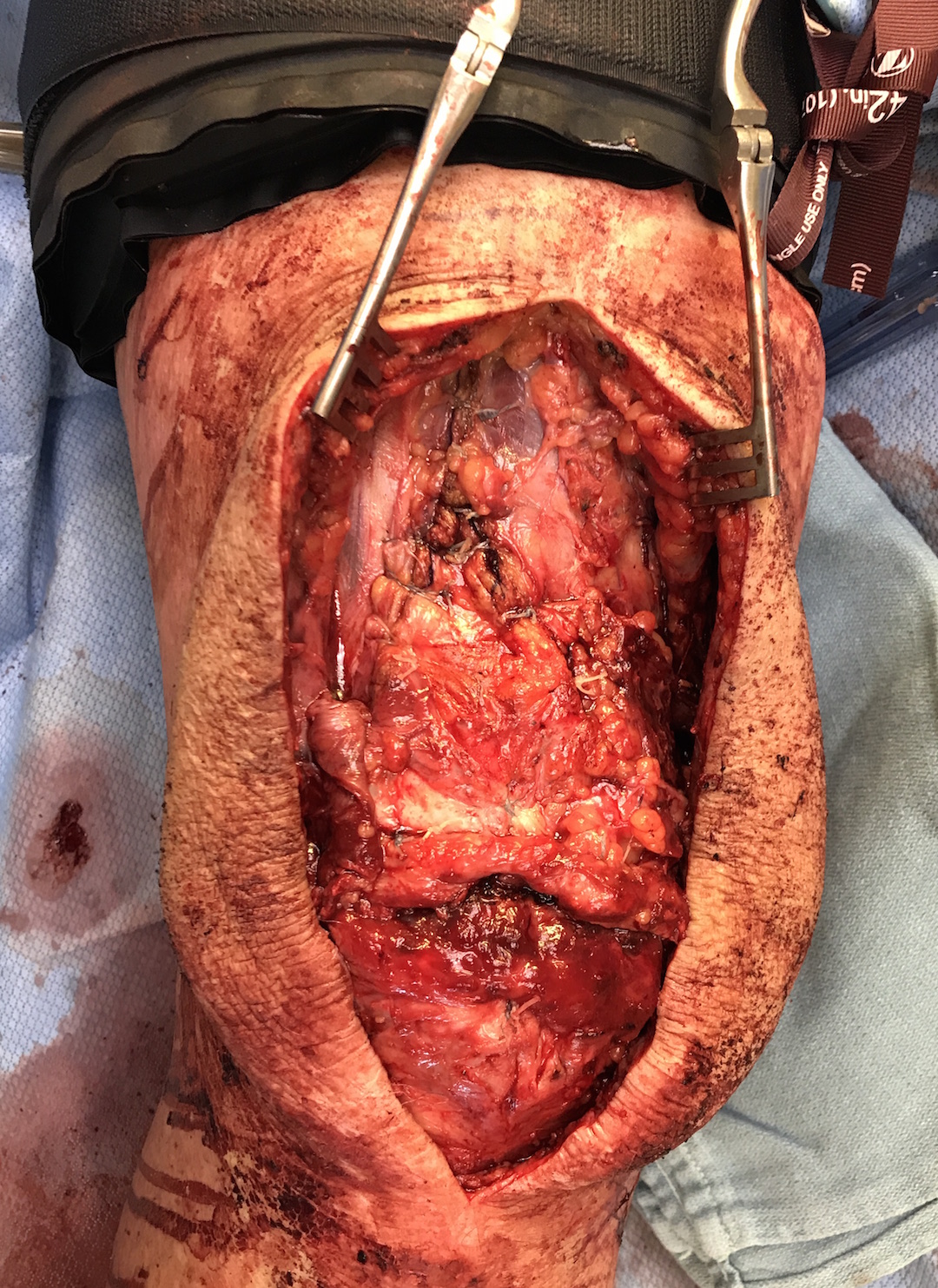
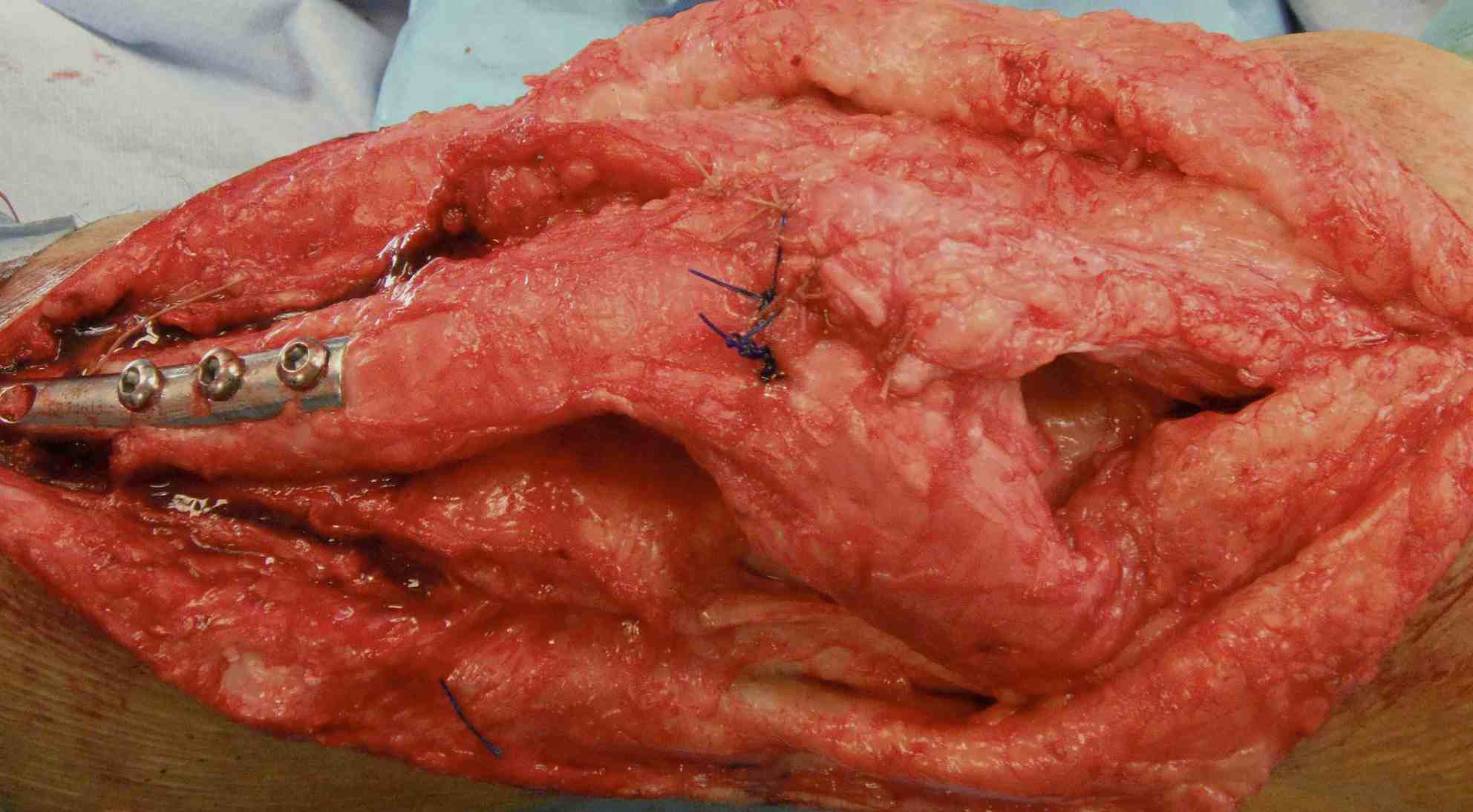
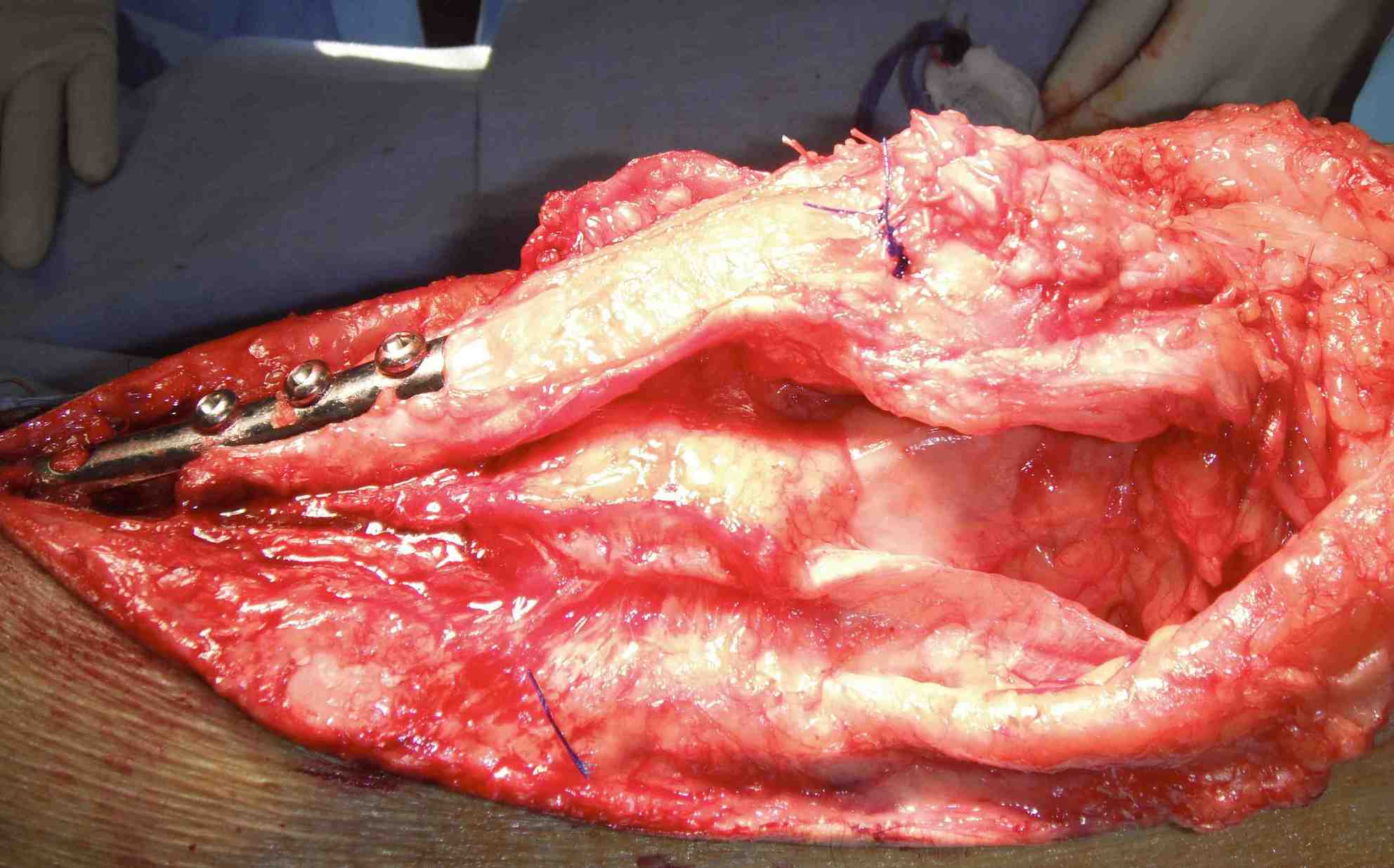
Drill holes in patella
- pass sutures with houston suture passer
- pass large non absorbable suture
- multiple times through tendon
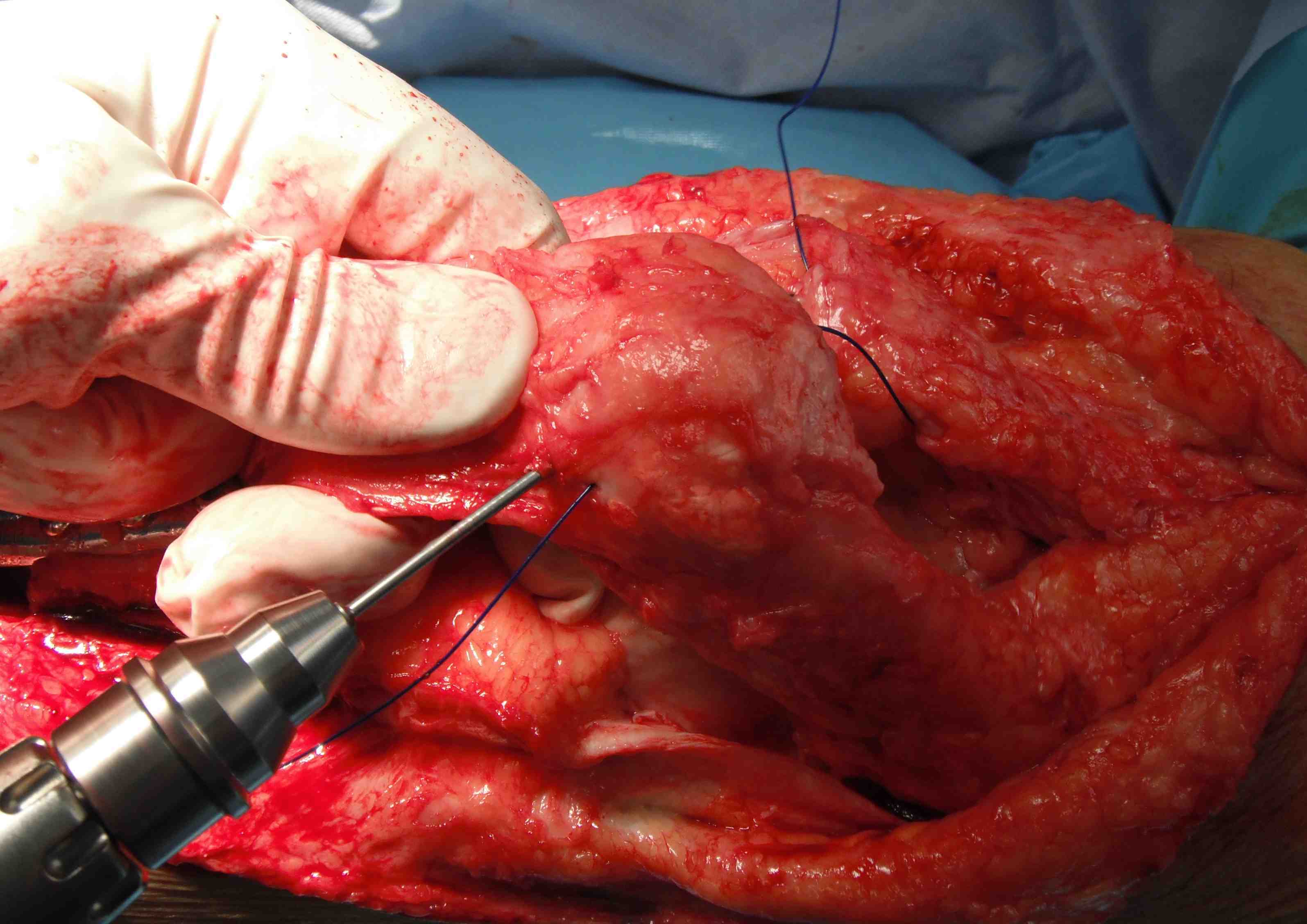
Other option
- suture anchors in distal patella
Post operative rehab
- keep in extension 6 - 8/52
Late presentations / Rerupture
Options
- quadriceps VY advancement
- allograft
- tibial tuberosity osteotomy and proximalization of the patella
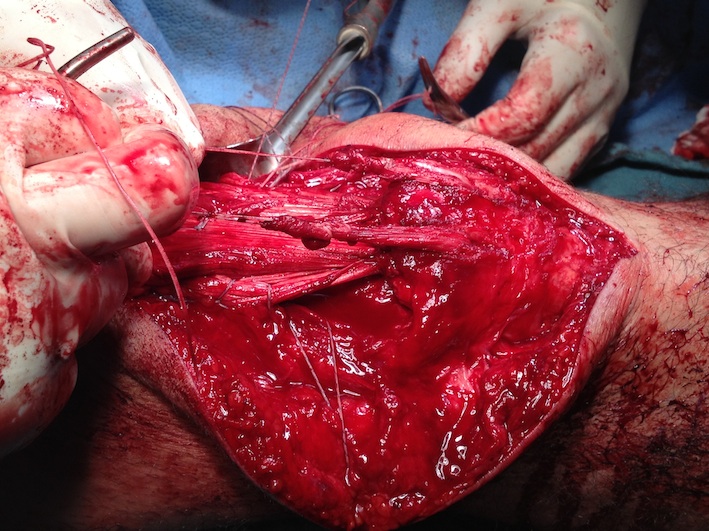
1. VY advancement
Will give an extra 2 cm
2. Tibial tuberosity osteotomy and proximalization of the patella
Note: Patella Baja with chronic rupture
- patient may develop patella baja
- with chronic injuries / failed injuries
- may need to perform tibial tuberosity osteotomy


3. Allograft Reconstruction




Tendo-achilles
- flat portion oversewn proximally
- two limbs passed through drill holes in patella
- sewn onto themselves