Intraoperative Fractures
1. Shaft fracture from IM rod

2. Posterior condylar fracture
Management
- assess stability
- ORIF if needed


Periprosthetic Fractures
Definition
Within 15 cm of the joint line
Within 5cm of the implant
Incidence
Uncommon
- 0.6% primary TKR
- 1.6% revision TKR
Most common > 70 / female / revision TKR
Mechanism
Low velocity fall in elderly osteoporotic patient
Associated Factors
Patient
- RA
- steroids
- osteopenia
Surgical
- revisions
- notching
- arthrofibrosis / MUA
- wear / osteolysis
Notching
Cause
1. Posterior referencing and down sizing femur
2. Internal rotation femur / medial notching
Results
Stamiris et al Eur J Orthop Surg Traumatol 2022
- meta-analysis of 3264 TKRs
- supracondylar fracture risk OR 4.85 if notched > 3mm
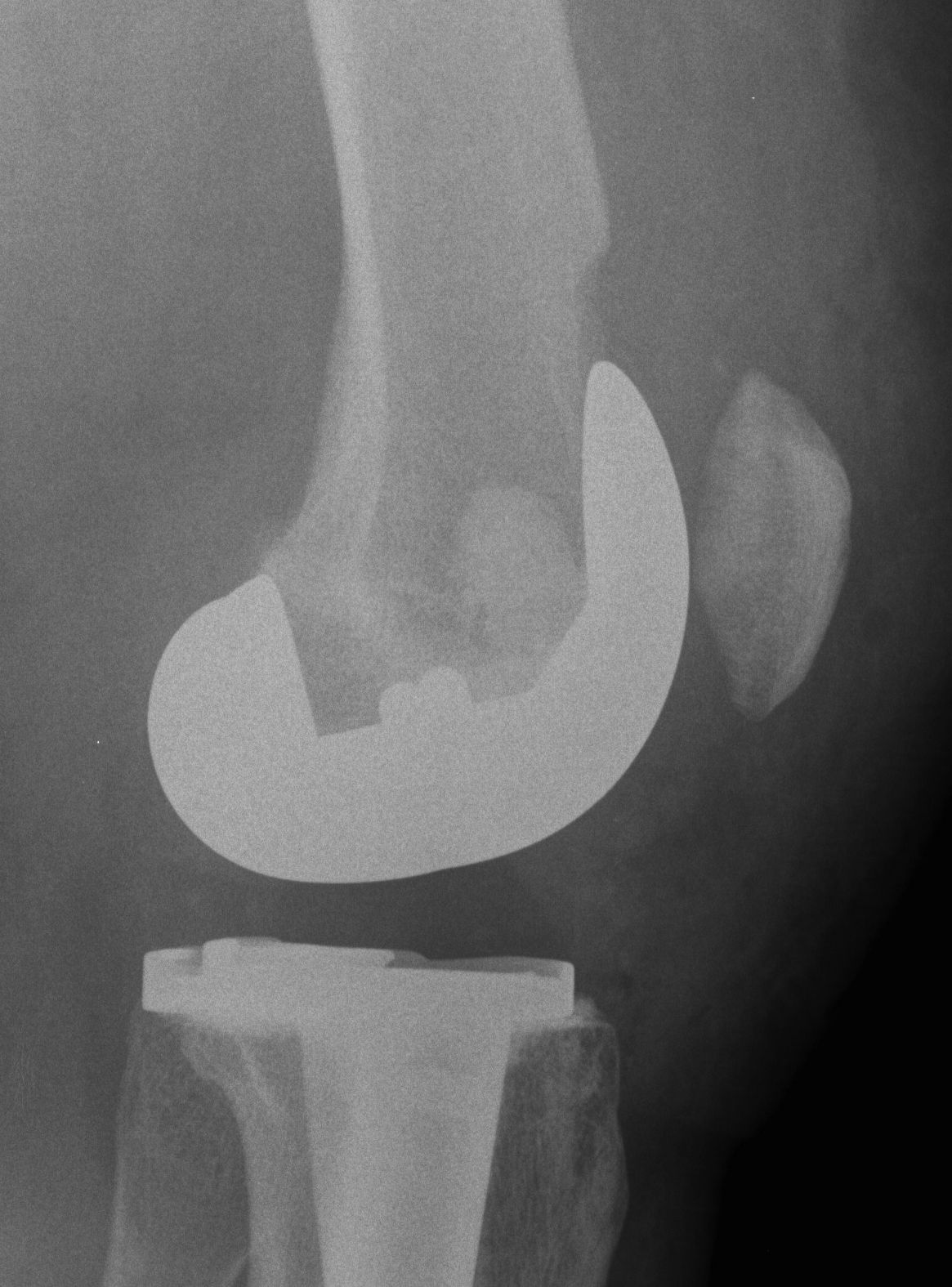
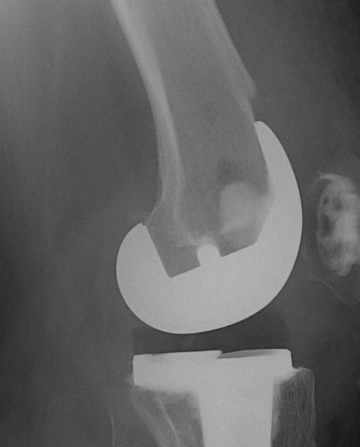
Xray Assessment
Fracture location
Femur
- proximal to femoral prosthesis
- distal to femoral prosthesis / reduced amount of distal bone for fixation
Tibia
Prosthesis stability
Bone stock
Suitability of femoral implant for IMN
Non-Operative Management
Indication
For minimally displaced fractures
Results
High rates of nonunion / malunion / stiffness
- Better outcomes with operation unless significant co-morbidities
Operative Management
Options
1. Lateral locking plate
2. Retrograde IM nail
3. Anterograde IM Nail
4. Revision TKR
1. Lateral locking plate

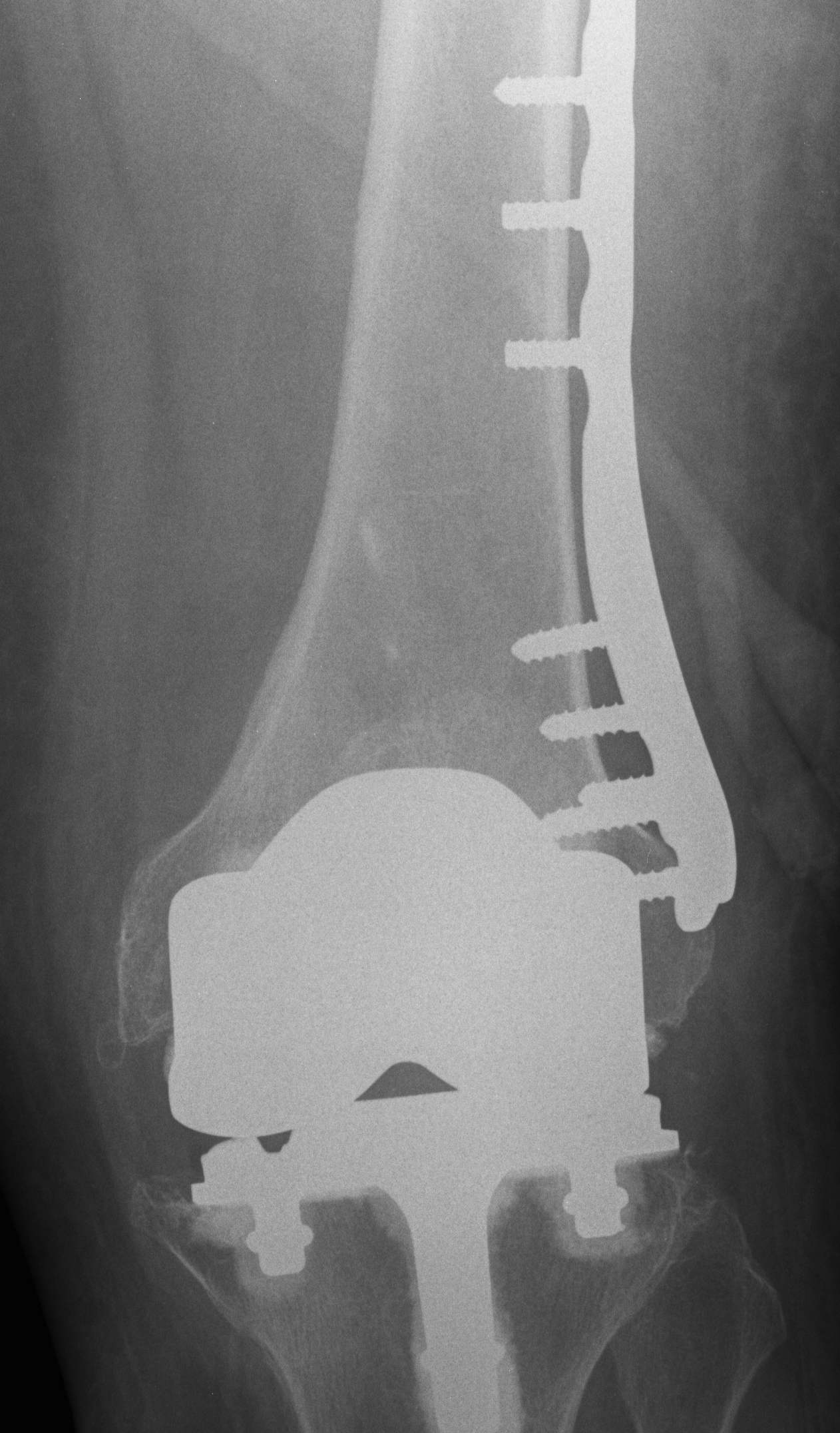

Technique
Minimally invasive technique
- may need unicortical screws distally
Results
Kolb et al J Trauma 2010
- 19 patients treated with LISS plate
- 2 delayed union
- otherwise good union rate with minimal complications and good ROM
Streubel JBJS Br 2010
- compared proximal fractures to distal (beyond the femoral prosthesis)
- showed similar healing rates in each group treated with locking plates
Complications
Non union






2. Retrograde IM Nail

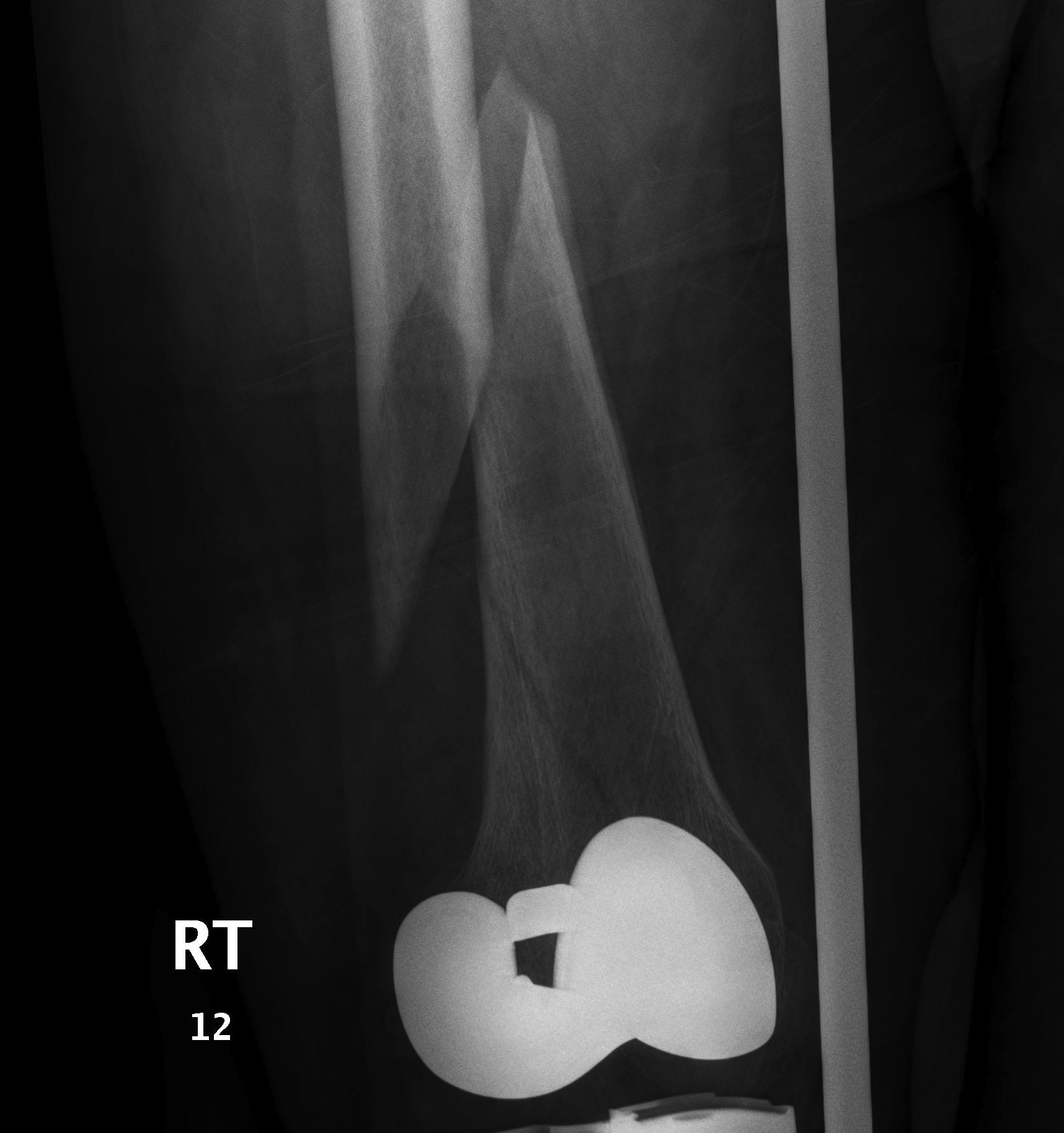


Issue
May be biomechanically superior
Have to open TKR to perform operation
- risk deep infection
Indications
Technically feasible
- CR knees contra-indicated
- must have sufficient sized hole in PS femoral component
- consult company as to suitablity
- small diameter nail
Technique
Minimum intercondylar distance of 12 mm
- AGC 18MM
- PFC = 20MM
- Genesis = 20MM
Usually remove polyethylene component
- replace after nail
- usually need new poly
3. Anterograde nail
Indications
- sufficient bone above implant for distal locking
Issues
- stress riser between femoral implant and nail
- must ensure correct alignment



4. Revision TKR
Indications
- very distal fracture
- insufficient bone stock
- loose prosthesis
Components
- stemmed, constrained implant
- tumour prosthesis
Case 1







Link to free article
https://reader.elsevier.com/reader/sd/pii/S1877056817300117?token=4EEB6…