
Definition
Degeneration at the attachment of the plantar fascia to medial tuberosity of the calcaneum
Anatomy
| Origin | Layers / insertions | Action |
|---|---|---|
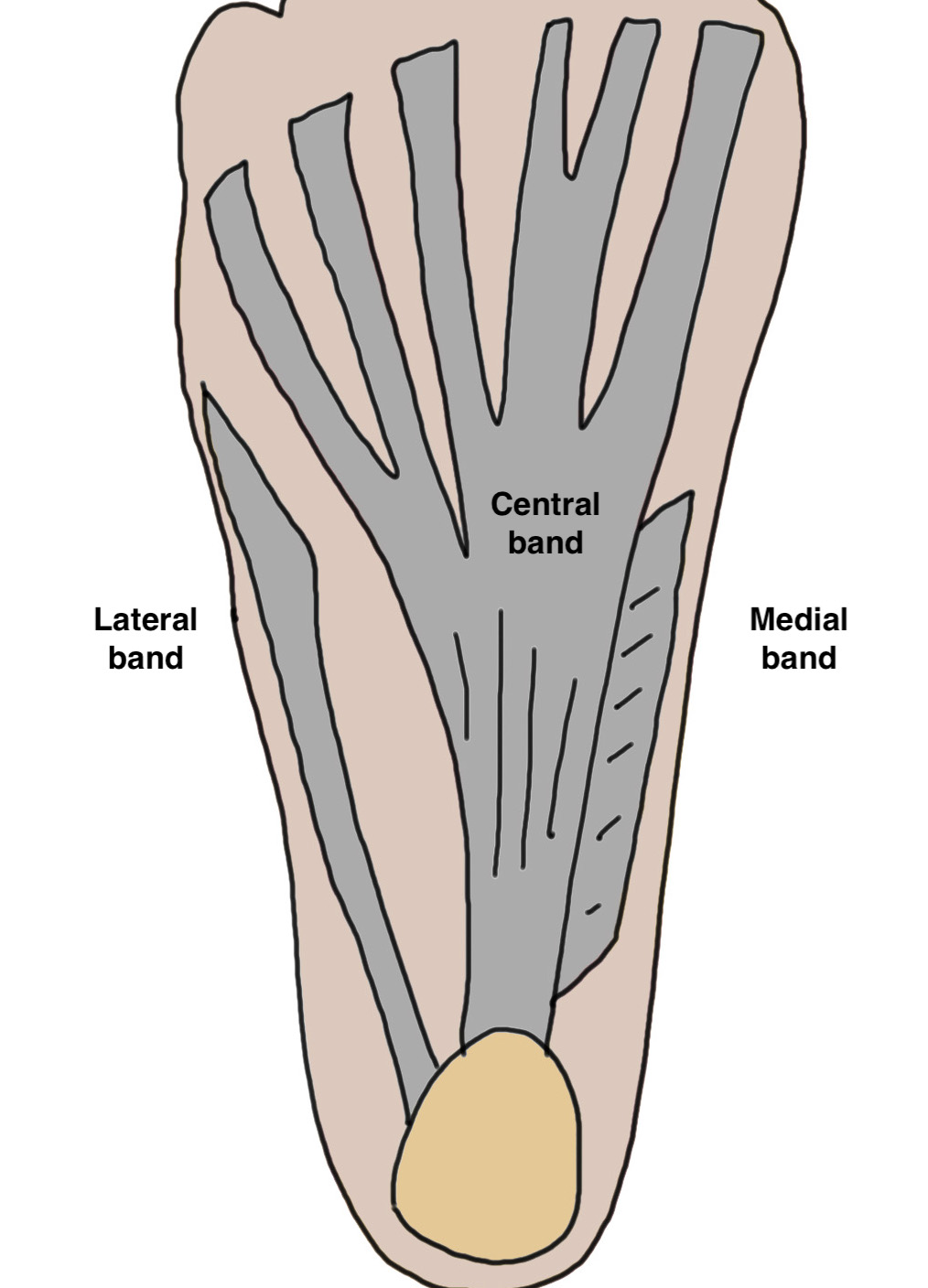
| Medial calcaneal tuberosity |
3 bands - Medial - overlies hallux - Lateral - over base of 5th - Central - 5 bands inserts volar plate / base P1
|
Stabilizes arch of foot - windlass mechanism - toes dorsiflex in toe off - elevates arch of foot |
Epidemiology
Patients aged 40 - 60
Women > men
30% bilateral
Risk factors
Chronic overload - walking occupations / athletes / runners / military
Obesity
Inflammatory conditions - Reiter's Disease, Ankylosing Spondylitis, Gout
Pronated feet / cavus feet / planus feet
Poor footwear
Tight tendoachilles
Pathogenesis
Degenerative process
- repetitive stress at attachment
- microtears & cystic degeneration
Natural history
Davis et al Foot Ankle Int 1994
- 105 patients with plantar fasciitis
- treated with orthotics and stretching
- 90% resolved by 11 months
History
Pain at inferomedial aspect of heel
- worse when first rising from bed
- worse with prolonged standing or exercise
Examination
Local tenderness at inferomedial aspect of calcaneal tuberosity
Windlass / Jack test - pain aggravated by passive dorsiflexion of toes
Pec cavus / planus
Tight Tendoachilles / Silverskiold
- > 10 degree difference in ankle dorsiflexion with knee flexed and extended
X-ray

Calcaneal spurs
Moroney et al Foot Ankle Spec 2014
- 1100 foot xrays
- calcaneal spurs in 12%
- more common women / older / diabetes / OA
- associated with foot pain
Zhou et al J Foot Ankle Surg 2015
- 2 types calcaneal spur
- Type A: superior to plantar fascia
- Type B: located within plantar fascia
Calcaneal spur above plantar fascia which is thickened with tears
Ultrasound
Thickened plantar fascia > 4.5 mm
Hypoechoic areas consistent with tears
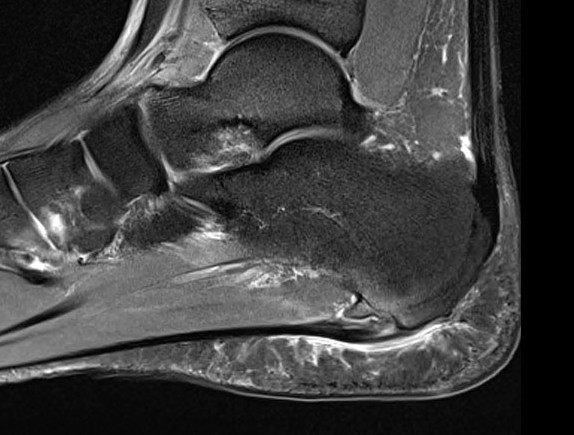
MRI
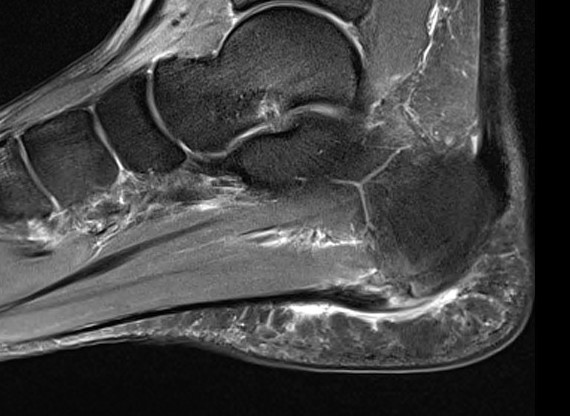

Thickened plantar fascia with tears
Exclude - retrocalcaneal bursitis / calcaneal stress fracture / Baxter's neuroma / tarsal tunnel syndrome
DDx
Calcaneal stress fracture
Fat pad syndrome
Tarsal tunnel syndrome - burning + numbness plantar aspect foot, EMG
Baxter's neuroma
- first branch lateral plantar nerve / Baxter's nerve
- mixed motor and sensory
- burning across heel pad
- motor to abductor digiti minimi
- EMG
- MRI shows atrophy of abductor digiti minimi
Posterior heel - Achilles tendonitis / retrocalcaneal bursitis / subtalar joint OA
Seronegative arthropathies - bilateral heel pain, young patients
Management
Non-operative
Options
Stretches - tendoachilles / plantar fascia
Orthotics / Night splints
ECSW - shock wave
Injections - corticosteroid / PRP / Botox
Stretches
- RCT of 101 patients
- plantar fascia v tendoachilles stretching
- superior outcomes with plantar fascia stretching
Orthotics / Night splints
Schuitema et al J Sport Rehabil 2019
- systematic review of 43 articles and 2800 patients
- full length insoles superior to heel cups
- RCT of 116 patients
- no effect of night splint over 3 month period
ECSW
Cortes-Perez et al Clin Rehabil 2024
- systematic review of 16 RCTs and 1100 patients
- ECSW compared to cortisone injections
- ECSW superior at reducing pain and improving function at 3 and 6 months
Injections
Cortisone
Short term relief / risk of plantar fascia rupture
- systematic review
- placebo RCT demonstrate significant effect cortisone
- short acting 4 - 12 weeks
Kim et al Foot Ankle Spec 2010
- retrospective review of 120 patients treated with cortisone injections
- 2.4% incidence of plantar fascia rupture
- average BMI 38 and average number injections 2.7 with rupture
PRP
Herber et al Foot Ankle Surg 2024
- meta-analysis of 21 RCTs and 1300 patients
- PRP superior to placebo / ECSW / cortisone
Botox - Botulinum Toxin A
Injection into gastrocnemius / plantar fascia
Roca et al Disabil Rehabil 2016
- 72 patient RCT of Botox v ECSW
- superior pain relief with ECSW
Ahmed et al Foot Ankle Int 2017
- RCT of saline v Botox in 50 patients
- significant improvement in Botox group
Operative management
Options
Partial plantar fasciotomy - open / endoscopic / ultrasound guided
Medial gastrocnemius recession
Percutaneous radiofrequency microtenotomy
+/- Calcaneal spur removal
+/- Decompression of the first branch of the lateral plantar nerve (Baxter's nerve)
Partial plantar fasciotomy
Results
Open partial plantar fasciotomy
Woelffer et al J Foot Ankle Surg 2000
- 33 feet with 5 year follow up
- 91% satisfaction rate
- 82% had 90% pain relief or better
Endoscopic partial plantar fasciotomy
- 30 patient RCT
- endoscopic fasciotomy v non operative treatment
- better VAS scores with operative at 2 years
- surgery better return to running and jumping
Open v endoscopic partial plantar fasciotomy
Feng et al Foot Ankle Int 2021
- retrospective study of 62 patients
- open v endoscopic
- better results with endoscopic at 6 months
- no difference at 1 or 2 years
Open technique
Vumedi medial approach open plantar fasciotomy
Vumedi plantar approach open plantar fasciotomy
Incision
- medial longitudinal incision - risk medial calcaneal nerve
- plantar incision
Technique
- identify central band plantar fascia origin from tuberosity
- medial incision in plantar fascia 1 cm from insertion
- release medial 50% of plantar fascia
- resect 5 mm medial rectangle of plantar fascia / fasciectomy to prevent recurrence
+/- resect calcaneal spur - exposed by releasing plantar fascia
+/- neurolysis
Endoscopic technique
Technique
Arthroscopy techniques endoscopic plantar fasciotomy PDF
Arthrex endoscopic plantar fasciotomy animation video
Arthrex endoscopic plantar fasciotomy video
Medial gastrocnemius recession
Technique
Arthrex endoscopic gastrocnemius release video
Arthrex endoscopic gastrocneumius animation video
Results
Pickin et al J Foot Ankle Surg 2022
- systematic review of medial gastrocnemius recession for plantar fasciitis
- mean 76% reduction in pain at 1 year
Gamba et al Foot Ankle Int 2020
- RCT of gastrocneumius release v plantar fascia release
- 86% satisfaction in gastrocnemius release
- 90% satisfaction in plantar fascia release
Percutaneous Radiofrequency Microtenotomy
Technique
Simulates healing / blood flow
Results
Yuan et al J Orthop Surg Res 2020
- comparison on open release versus RF in 39 feet
- equal outcomes and shorter recovery with RF