
Incidence
Tennis elbow
- middle aged population
- 1 - 3%
80% will resolve within 1 year
Etiology
Repetitive microtrauma
Pathology
Mainly affects ECRB
- tendon degeneration and partial tears
- minimal inflammation on histology
Angiofibrotic hyperplasia
- fibroblast proliferation
- vascular hyperplasia
Anatomy
ECRB
- arises from lateral epicondyle
- tendinous insertion
ECRL and Brachioradialis
- arise from lateral supracondylar ridge
- ECRL still muscular at lateral epicondyle
Clinical
Pain lateral elbow
- with gripping
- wrist extension with resistance
Tender ECRB - 5 mm distal and anterior to CEO
Pain with
- resisted wrist dorsiflexion
- resisted middle finder extension
DDx
Radial tunnel syndrome
- PIN compression in radial tunnel / supinator
- tenderness 3-4 cm distal to lateral epicondyle
- pain with resisted supination
www.boneschool.com/radial-tunnel-syndrome
Xray
May see dystrophic calcification

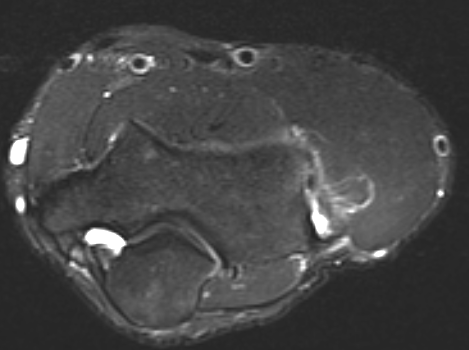
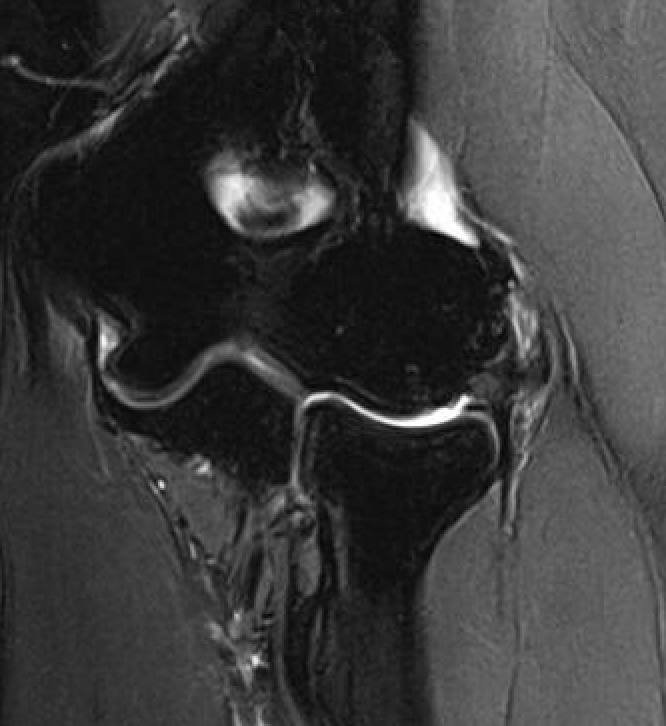
MRI
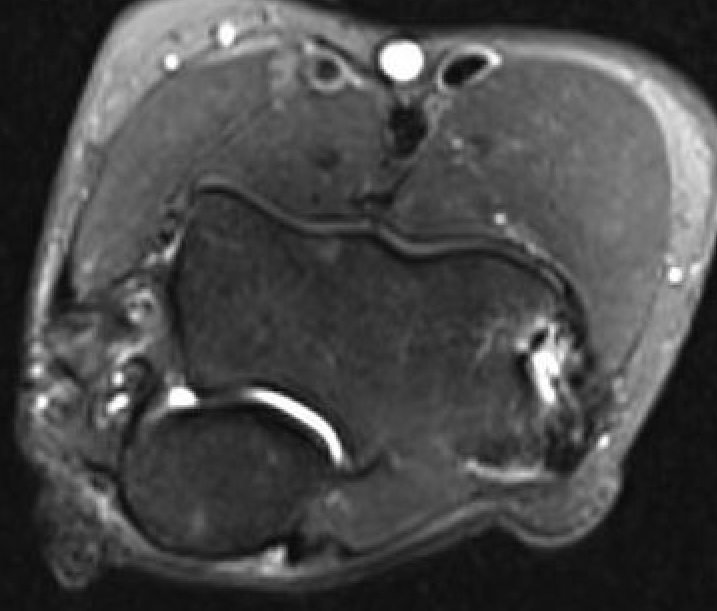
High grade partial tears of ECRB on lateral eipcondyle


Tendonopathy of the common extensor origin, with thickening and high grade tear partial tear
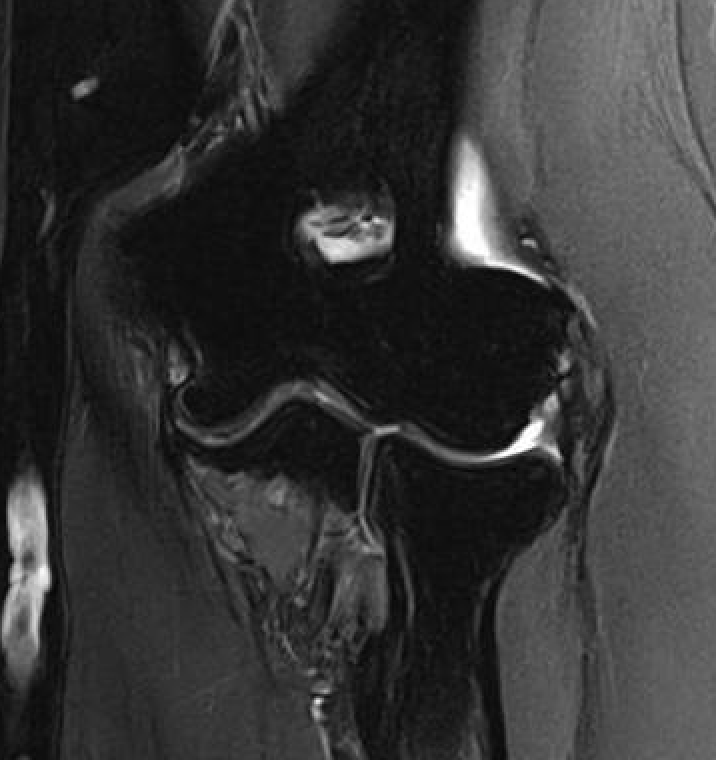
Tendonopathy of the common extensor origin, with thickening and high grade tear partial tear
Nonoperative management
Options
Counterforce braces
Physiotherapy - eccentric exercises
Shock wave
Transdermal nitroglycerin patches
Dry needling
Injections - cortisone / PRP / Botox

Physiotherapy
- systematic review of 6 RCTs and 430 patients
- evidence for improvement in pain
Transdermal nitroglycerin patches
- systematic review of nitroglycerin patches
- evidence for short and mid term pain and functional improvement
- complications include headache and dermatitis
Extra corporeal shock wave (ECSW)
- systematic review of 6 RCTs
- shock wave v cortisone
- cortisone better pain relief at 1 month
- ECSW better pain relief at 3 and 6 months
Dry needling
- RCT of dry needling v cortisone in 108 patients
- equal efficacy
- 8% of cortisone patients developed skin atropy and whitening
Injections
PRP v cortisone
- systematic review of 11 RCTs and 730 patients
- PRP v cortisone
- cortisone better pain relief at 2 months
- PRP better pain relief at 6 months
Botox v cortisone
- systematic review of 6 RCTs and 300 patients
- botox v placebo / cortisone
- botox superior pain relief to placebo for up to 4 months
- botox and cortisone equivalent
- cortisone better early pain relief and less weakness
Operative Management
Indication
Failure of good non-operative management
- > 6 - 12/12
Options
Open tennis elbow release
Arthroscopic tennis elbow release
Ultrasound guided percutaneous tenotomy
Results
- systematic review of open v percutaneous v arthroscopic approach to tennis elbow
- success rate arthroscopic 92%
- success rate percutaneous 91%
- success rate open 83%
- systematic review of open v arthroscopic tennis elbow release
- no difference in functional outcomes or complication rates
- longer operating times with arthroscopic
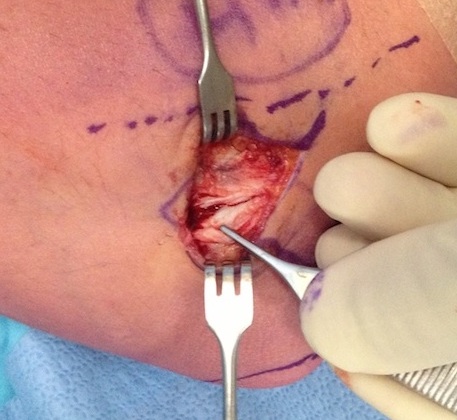
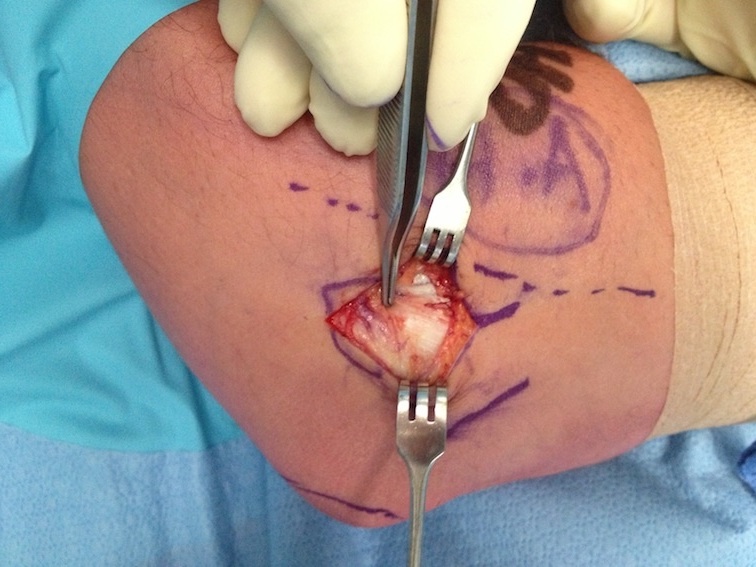
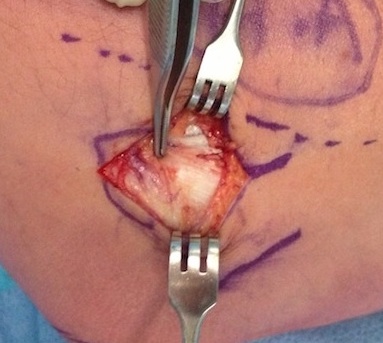
Open tennis elbow release
Technique
Vumedi open tennis elbow release video
Incision centered on common extensor origin
- slightly anterior to radiocapitellar joint
- elevate ECRL (ECRL muscular at this point)
- ECRB is deep and posterior to ECRL
- detach ECRB from lateral epicondyle
- debride degenerative tissue and decorticate underlying common extensor origin
- +/- reattach ECRB with suture anchors




Post tennis elbow repair with anchor
Results
- 171 open tennis elbow release with 10 year follow up
- 95% good results
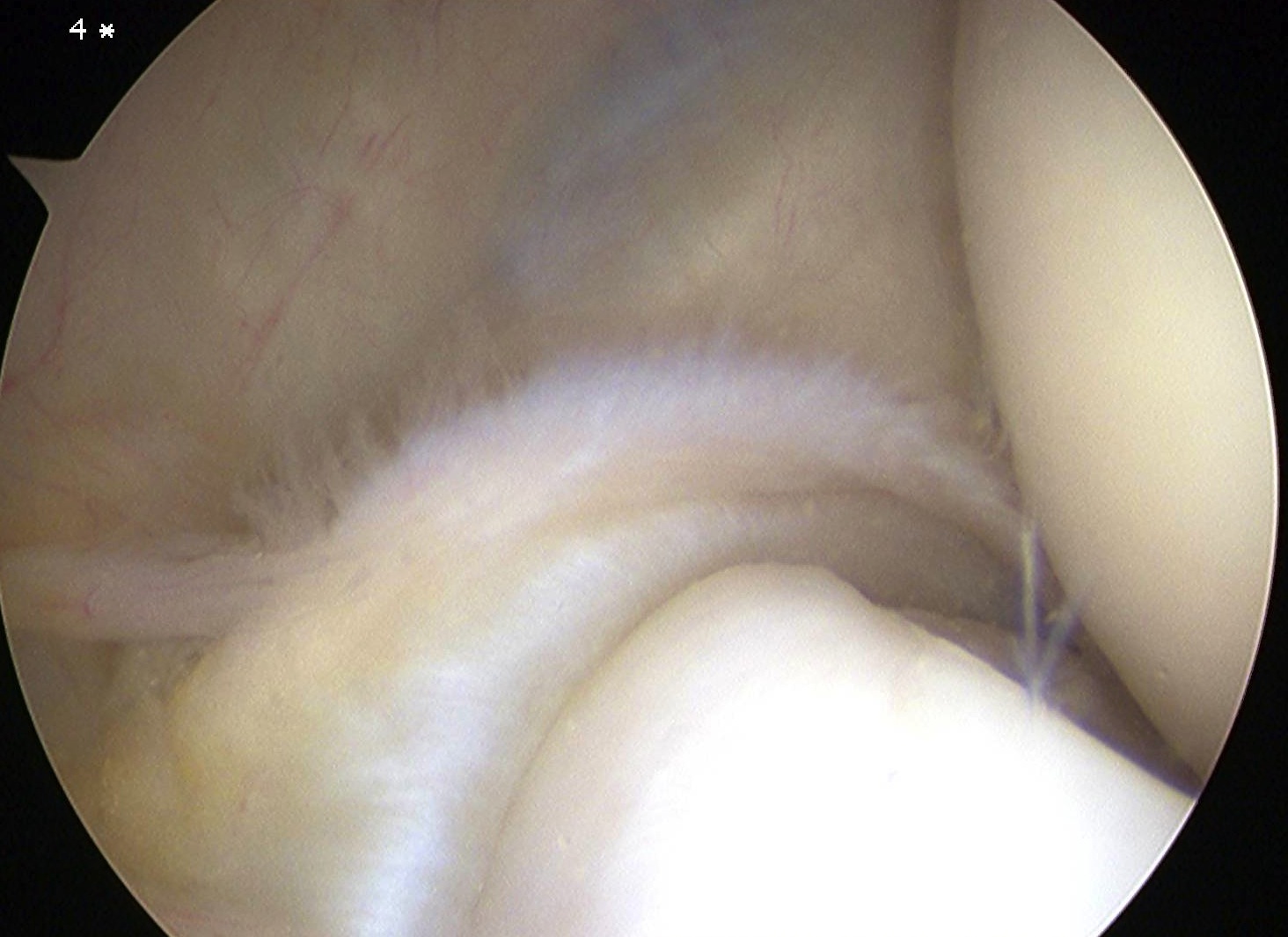
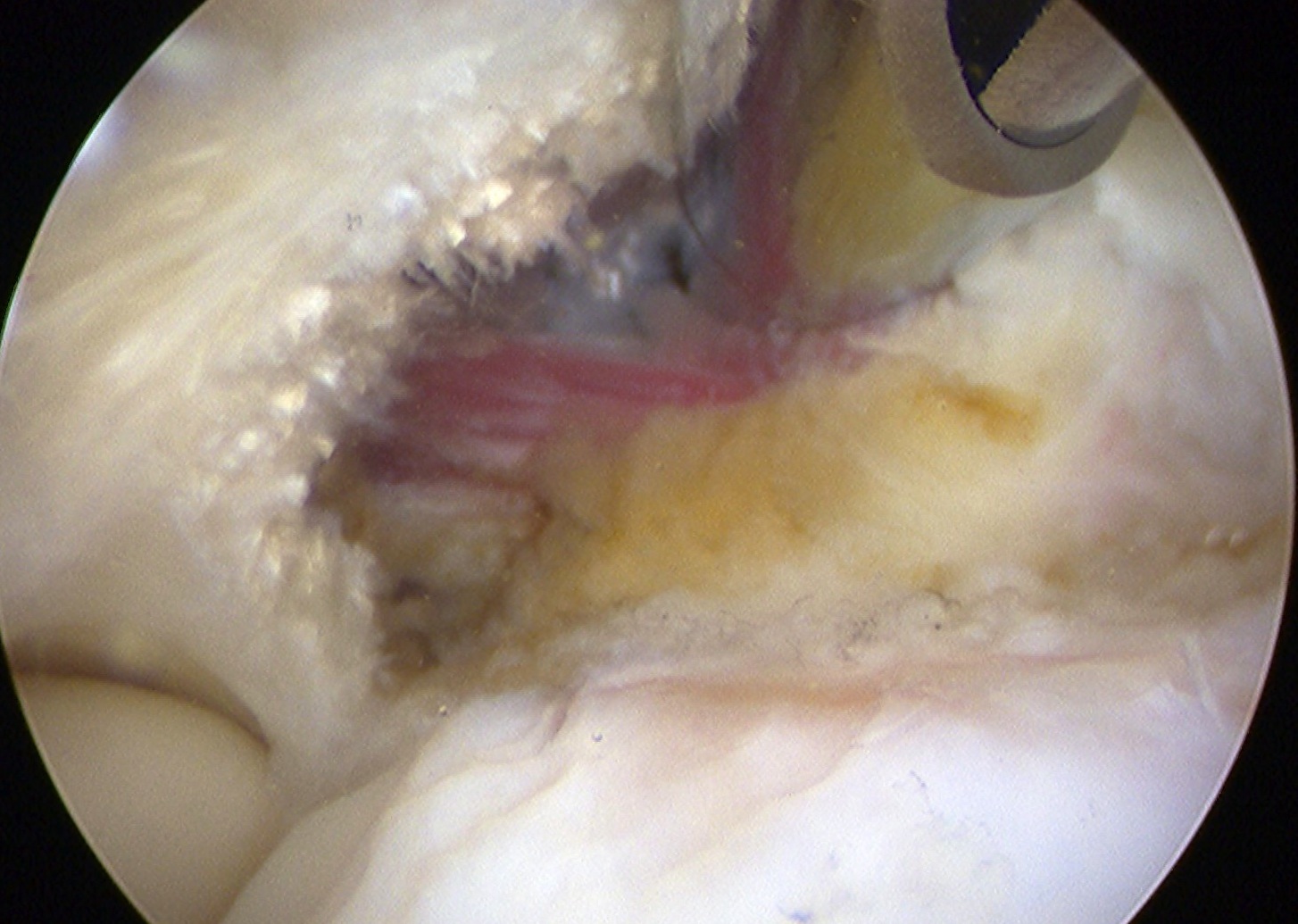
Arthroscopic tennis elbow release
Technique
Vumedi arthroscopic tennis elbow release video
Enter radiocapitellar joint
- release capsule
- release ECRB

Ultrasound guided percutanous tenotomy
Technique
Vumedi radiofrequency lateral epicondylitis ablation