


Etiology
Throwing athletes - repetitive microtrauma / valgus stress
Medial sided elbow pain
Baseball pitchers most common
- javelin throwers
- football quarterback
- tennis players
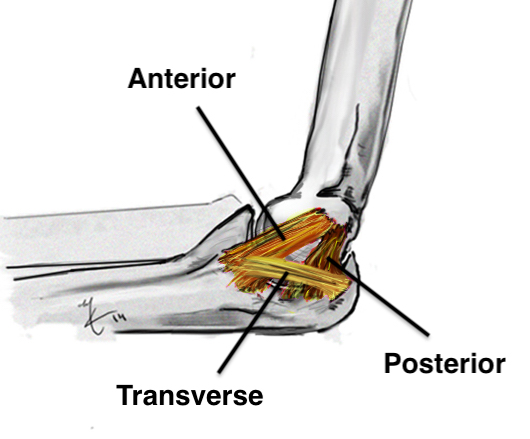
Anatomy of Ulna Collateral Ligament (UCL)
Provides valgus stability
Three components
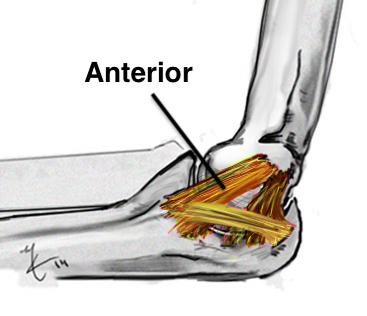
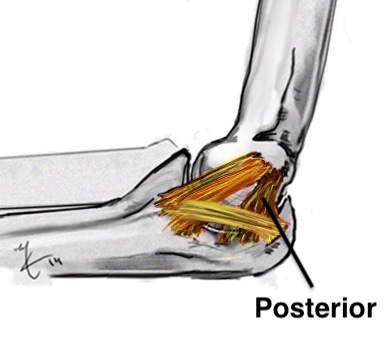
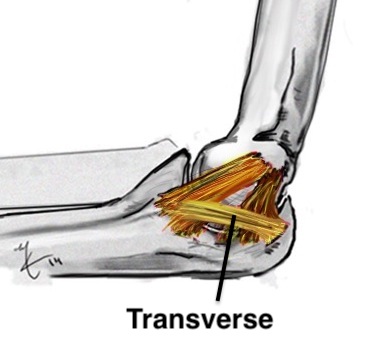
| Anterior band | Posterior band | Transverse band |
|---|---|---|
|
Most important Stabilizes from 30 - 90 degrees flexion |
Fan shaped Stabilizes from 90 - 120 degrees |
Does not cross elbow joint Does not contribute to vaglus stability |
| Medial epicondyle to sublime tubercle |
Medial epicondyle to medial semilunar notch of ulna |
Medial olecranon to medial coronoid |
|
Taut band Mean 6 mm thick |
||
 |
 |
 |
History
Medial sided elbow pain
Reduction in velocity & accuracy
40% ulna nerve symptoms
Examination
Pain on palpation of anterior bundle MCL
- flexor pronator muscle bulk covers insertion in full extension
- reveal UCL with flexion
| Valgus stress test | Milking maneuver |
|---|---|
|
Patient supine
Elbow flexed 25 degrees (removes bony stability) - valgus stress and palpate UCL |
Patient seated or standing
Shoulder extended and externally rotated - thumb pointing out / wrist supinated - elbow at 90 debrees - pull on thumb and extend arm which places a valgus strain |
| Modified Jobes - patient prone | |
  |
 |
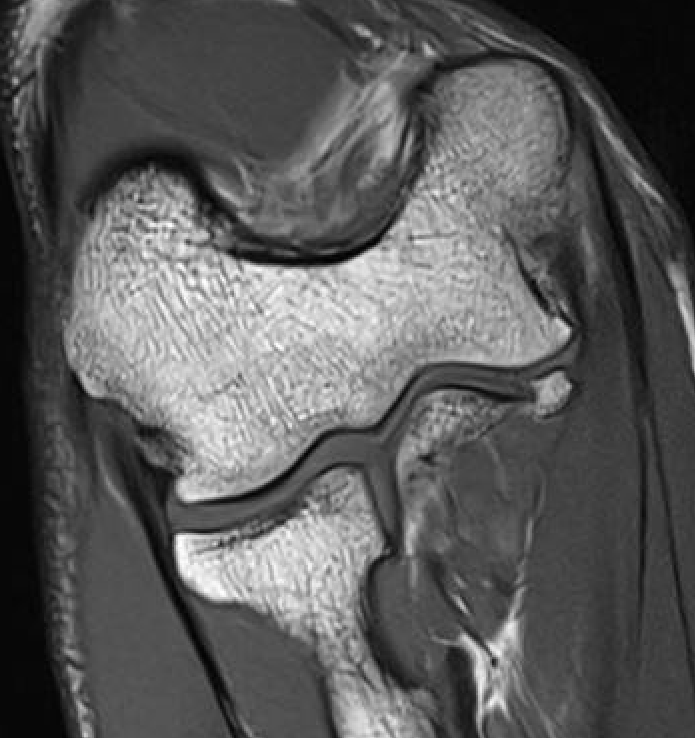
MRI
Intact

Grading of tears
Proximal / midsubstance / distal injury
Partial tears - low grade versus high grade
Complete tears


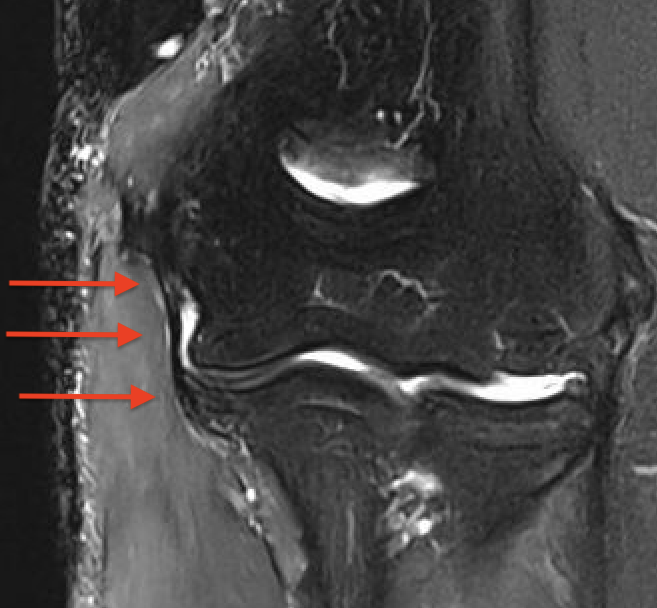
Acute full thickness UCL tear
High grade partial distal UCL tear
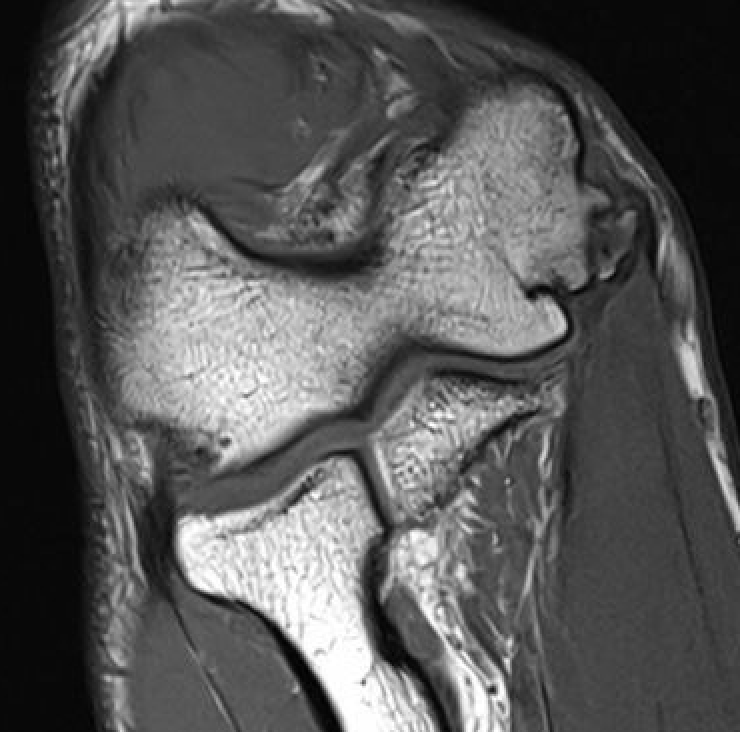
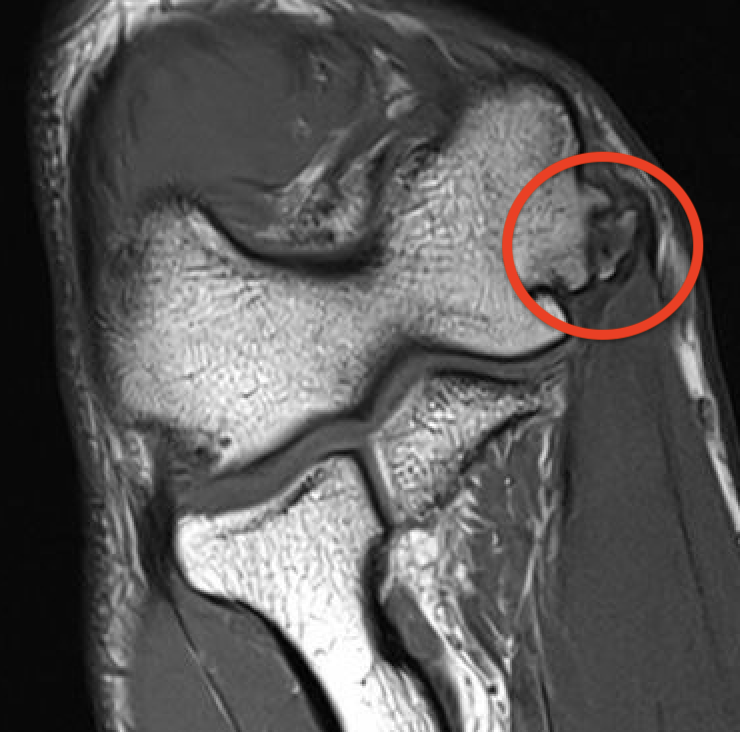
Bony avulsion UCL complex medial epicondyle
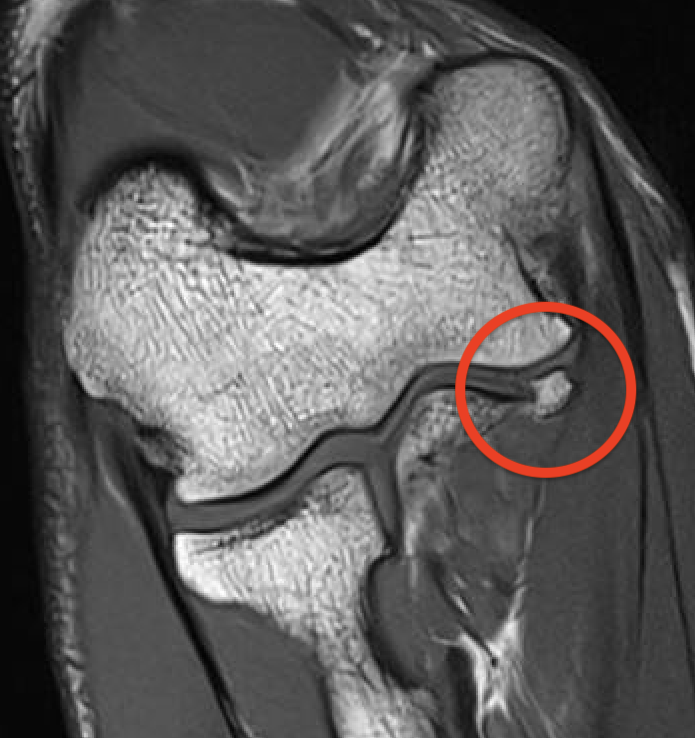
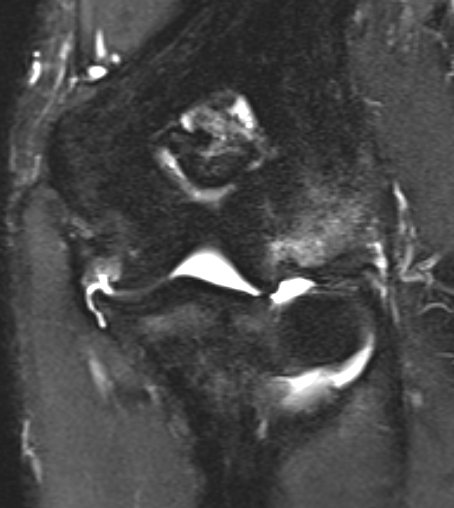
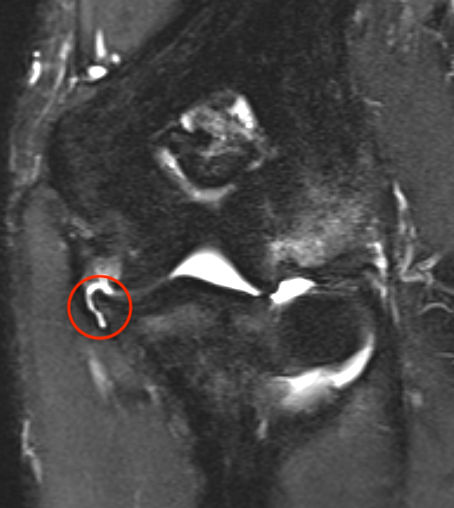
Bony avulsion UCL sublime tubercle
MRI findings in asymptomatic throwing elbows
- MRI of elbow in 426 baseball players
- 2/3 asymptomatic, 1/3 symptomatic
- 30% had evidence of high grade UCL injury
- no difference between groups
Nonoperative management
Options
Rest
Physiotherapy
PRP
Results
Outcome
- 544 MLB players treated nonoperatively for UCL injury
- 54% return to play
- no effect of PRP / distal v proximal tears / MRI grading
- systematic review of nonoperative care of UCL injuries
- return to previous level of sport 78%
- return to sport proximal tears: 90%
- return to sport distal tears: 41%
- lower return to sport with increasing UCL injury grading
- no effect of PRP
Incomplete tears
- 27 professional baseball players with incomplete UCL injuries
- treated non operatively
- return to play pitchers 82%
- return to play position players 90%
Operative management
Options
1. UCL reconstruction with autograft
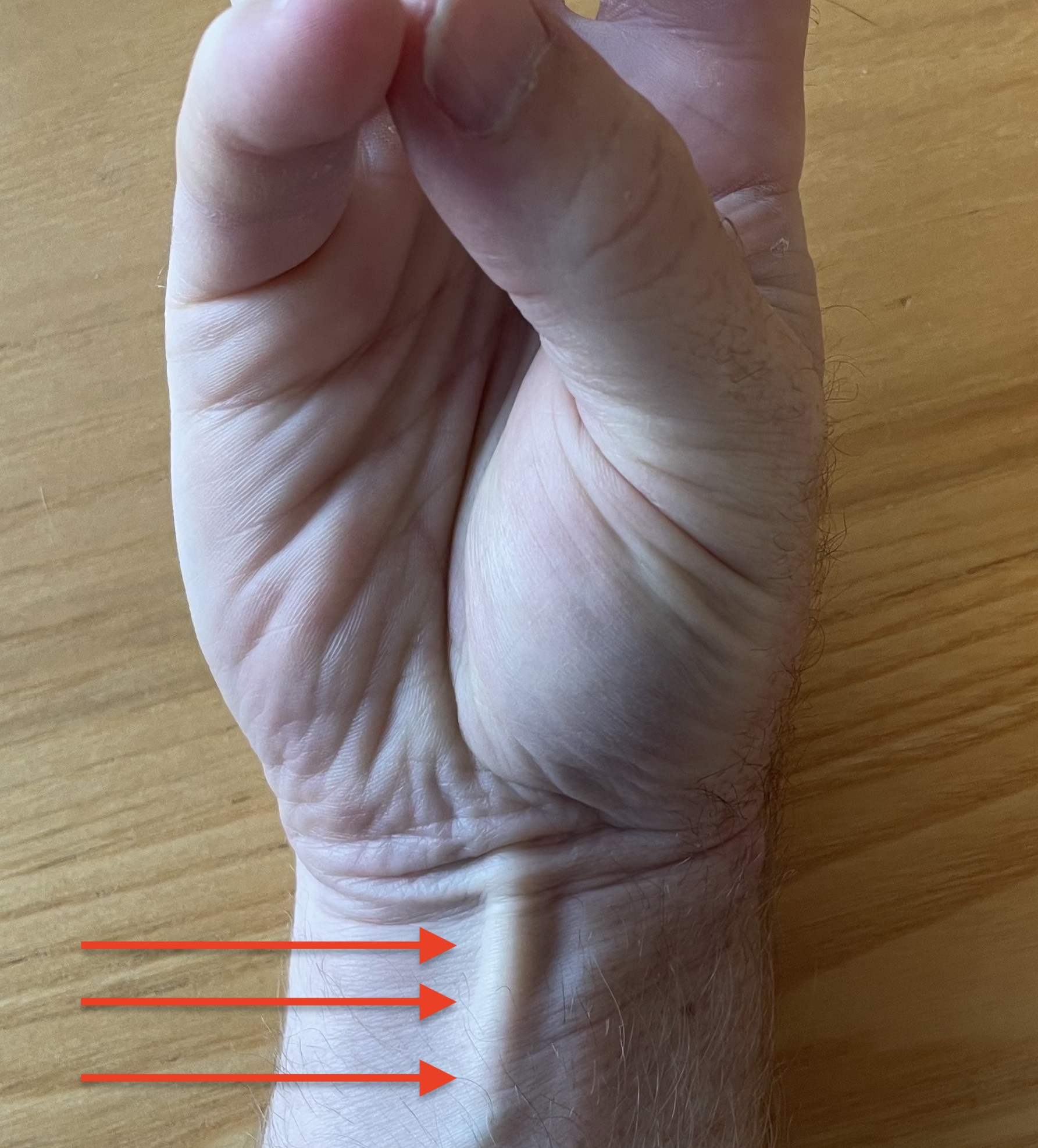
- palmaris longus if present
- gracilis / semitendinosis
- "Tommy John surgery" - name after famous MLB pitcher who was first to have surgery
1. UCL repair +/- internal brace -
- if avulsed from medial epicondyle or sublime tubercle
+ / - ulnar nerve transposition
Ulna collateral ligament reconstruction
Graft choices
Palmaris longus - present 85% / press thumb and finger together
Gracilis / semitendinosis
Vumedi 2 incision palmaris longus harvest technique video

Approach
Medial approach
- incision over medial epicondyle
- protect antebrachial cutaneous nerve
- protect and identify ulna nerve
- split FCU to expose ulna collateral ligament
- split UCL longitudinally
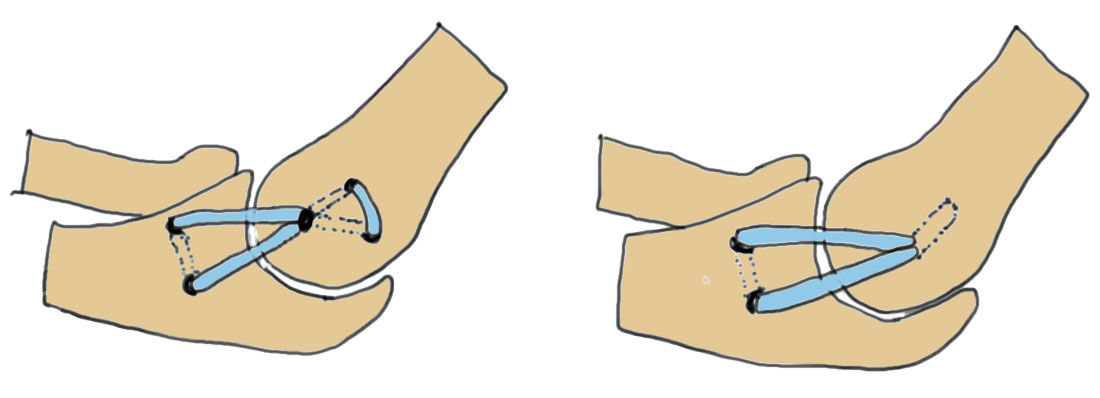
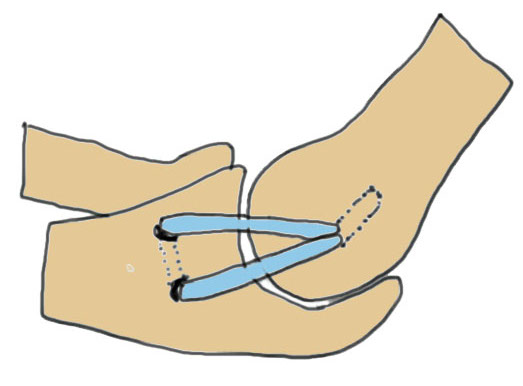
Modified Jobe / Figure 8 reconstruction
Technique
Vumedi UCL reconstruction with palmaris longus and figure 8 video
Proximal insertion - Y shaped tunnel in medial epicondyle
Distal insertion - transverse tunnel across ulna / sublime tubercle
Docking technique
Technique
Vumedi UCL reconstruction with palmaris longus and docking technique video
Arthroscopy techniques UCL reconstruction with palmaris longus and docking technique PDF
Distal insertion - transverse tunnel across ulna / sublime tubercle
Proximal insertion - blind tunnel in medial epicondyle
Results
Outcomes
Cain et al Am J Sports Med 2010
- modification Jobe technique + subcutaneous ulna nerve transfer
- 942 patients followed up for 2 years minimum
- 83% returned to previous level of sport at mean 12 months
- systematic review of 15 studies and 1100 patients
- mean age 20
- 86% return to sport at same level at mean 12 months
Graft type and technique
- 566 professional baseball players undergoing UCL reconstruction
- 64% palmaris longus: 83% return to play
- 24% gracilils: 81% return to play
- modified Jobe: 82% return to play & 6% revision UCL
- docking technique: 80% return to play and 6% revision UCL
Revision
- systematic review of 5 studies of revision UCL reconstruction
- MLB pitchers: return to sport at same level 69%
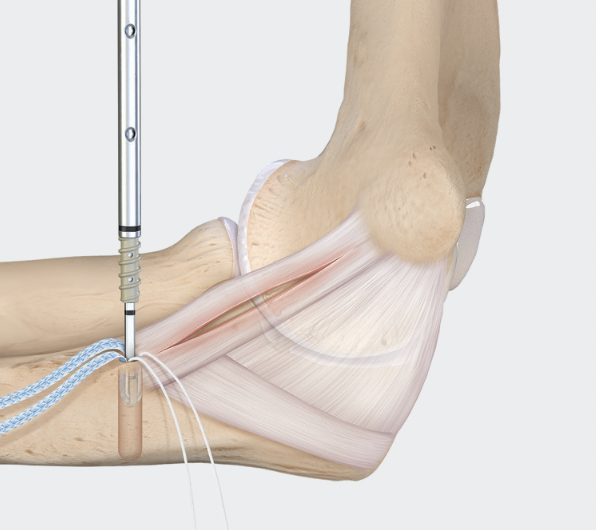
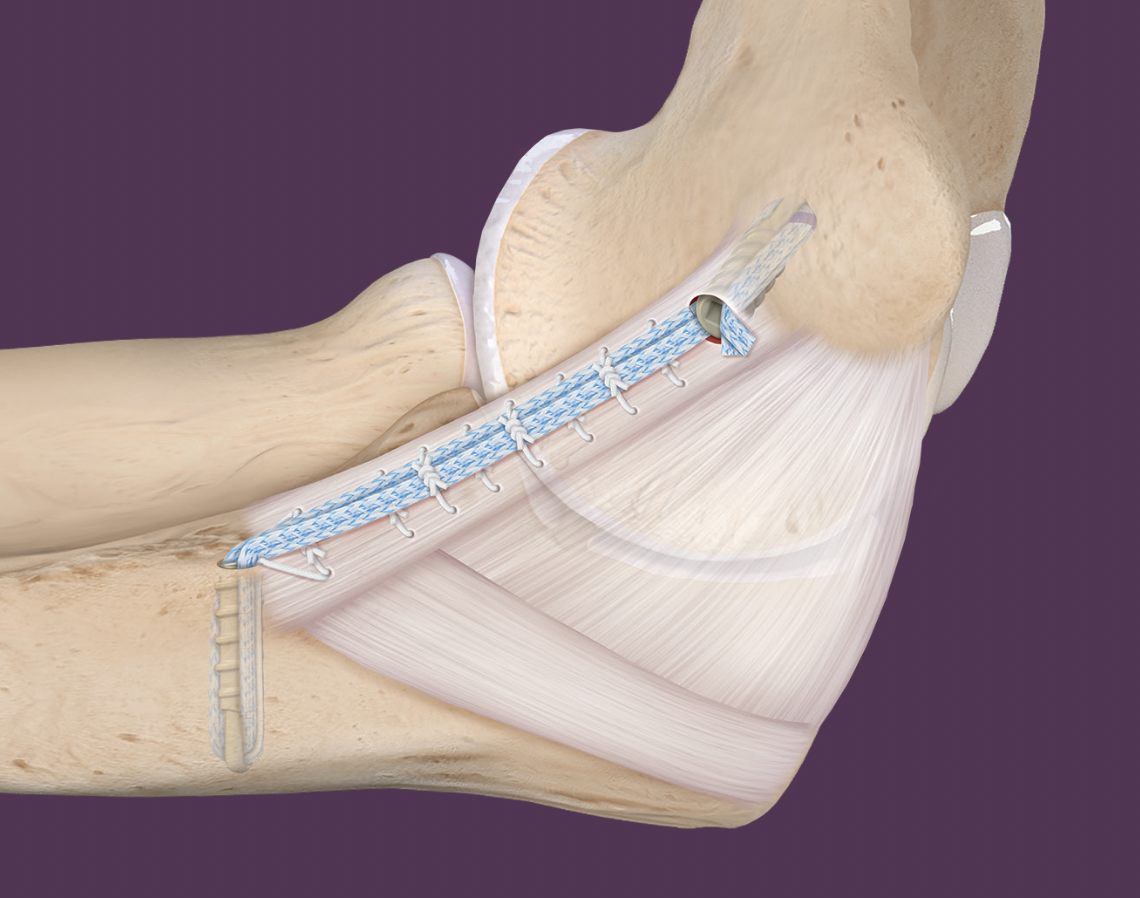
Primary UCL repair with internal brace augmentation
Technique
Arthrex internal brace UCL surgical technique PDF
Vumedi primary UCL repair with internal brace augmentation video
Arthroscopy techniques UCL repair with internal brace augmentation PDF
Arthrex UCL repair and internal brace video
Medial incision over medial epicondyle
- protect ulna nerve
- split FCU
- expose ulna collateral ligament
- repair avulsion from medial epicondyle / sublime tubercle as indicated with anchor
- ensure isometric
Results
Repair with internal brace versus reconstruction
- 461 athletes with repair + internal brace versus reconstruction
- repair if avulsed from medial epicondyle or sublime tubercle
- UCL repair: revision rate 9%, return to sport 99% at mean 9 months
- UCL reconstruction: revision rate 8%, return to sport 98% at mean 13 months
- no difference in outcomes but earlier return to sport with repair