Osteoarthritis
Epidemiology
Usually after 50-60 years of age
Aetiology
Primary 90% of cases
Secondary
- AVN
- trauma
- instability
Pathology

Usually after 50-60 years of age
Primary 90% of cases
Secondary
- AVN
- trauma
- instability
Epidemiology
- seen in women over 40
Xray
- sclerotic and overgrown
CT
OA of the scapho-trapezium-trapezoidal joints
50% patients with CMC OA have STT OA
F > M


Return to Sport
Shelbourne et al. Am J Sports Med 1999
- 133 patients with isolated PCL injuries followed for mean of 5 years
- 1/2 returned to sport at same level of play
- 1/3 returned to sport at lower level of play
https://pubmed.ncbi.nlm.nih.gov/10352760/
Agolley et al. Bone Joint J 2017
Resuscitation
EMST
Neurovascular assessment
Investigations - exclude Pipkin, NOF
Emergent reduction / skeletal stabilisation
Assess stability
Re-evaluate sciatic nerve
Indications
- displaced acetabular fracture
I. Lateral Spilt
- seen in young patient
- lateral meniscus can be incarcerated in fracture
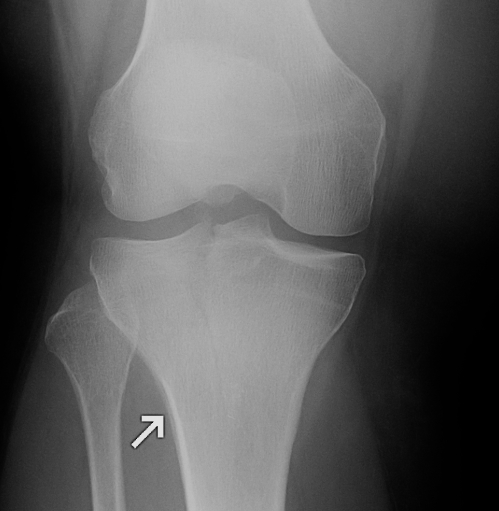
II. Lateral Split Depression
- often seen in young patients with high energy injuries
- vary in severity


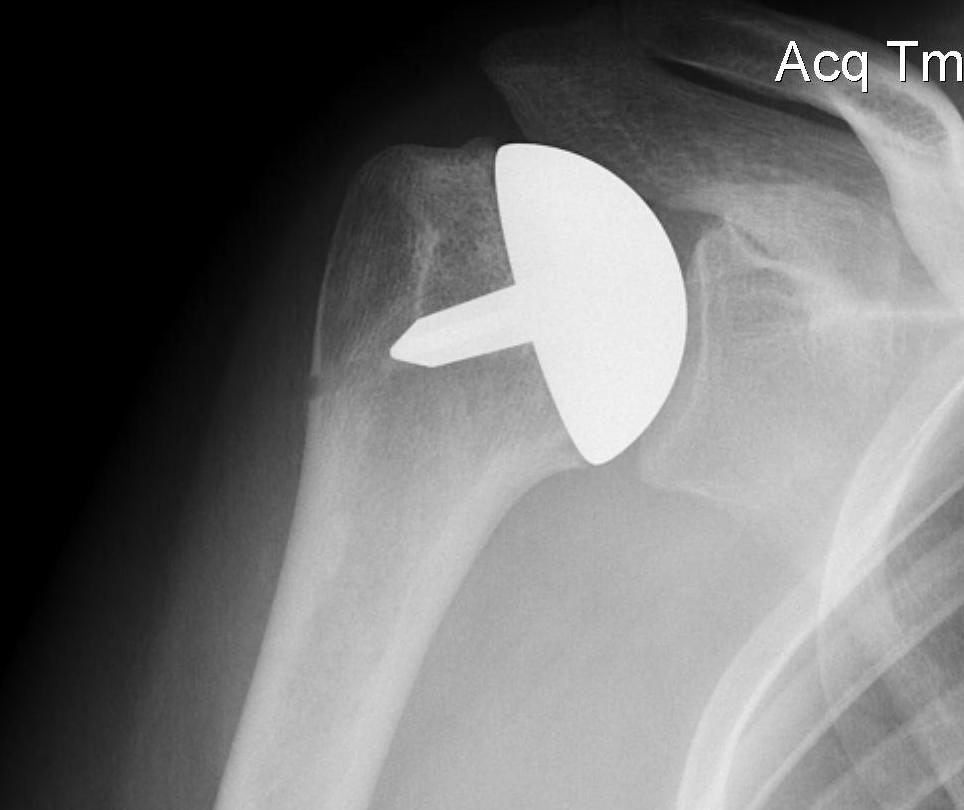
Fewer complications than TSR
Simpler procedure
OA
Psoriasis
CREST (scleroderma)
RA (rare form)
Other seronegative arthropathies
Hyperparathyroidism
Reactive arthropathy
Gout
Diagnosis
Pisotriquetral view
- forearm positioned 30° supinated off the neutral position
- loss of symmetry between the pisiform and triquetrum is required for the diagnosis
- carpal tunnel view may be helpful in further assessment of the joint
Clinical
More common problem


Darrach's
- distal ulna excision
- best for elderly RA patient
Bower's interpositional hemiarthoplasty
Technique