

Etiology
Primary osteoarthritis
Secondary
- trauma / distal radius fractures / distal ulna fractures
- inflammatory / Rheumatoid arthritis
- Madelung's deformity
Xray

DRUJ instability


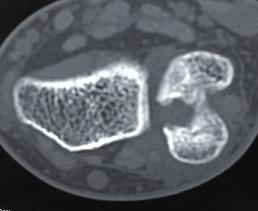
Post traumatic distal ulna osteoarthritis
Options
Distal ulna excision / Darrach's procedure
Interpositional arthroplasty
Distal radio-ulna arthrodesis with distal ulna pseuodoarthrosis / Suave-Kapanji
DRUJ Arthroplasty
- systematic review of distal ulna excision v arthrodesis
- Suave-Kapanji v Darrrach's
- similar satisfaction rates 70%
- distal ulna excision: instability 13%, reoperations 3%
- distal radio-ulna arthrodesis: instability 7%, reoperations 7%
Darrach's procedure / distal ulna excision
Indication
Elderly / low demand patients
Technique
Dorsal approach
- between ECU and EDM (extensor compartment 5 and 6)
- protect dorsal sensory branch of ulna nerve
- open extensor compartment
- open capsule
- resect distal 2cm of the ulna
- careful to close capsule under extensor tendons as tendon rupture is known complication
Youtube Darrach's distal ulna resection video
Results
Suave-Kapanji distal radio-ulna arthrodesis
Indication
Young, active patients
Technique
Distal radio-ulna arthrodesis with screws + proximal ulna pseudoarthrosis
Dorsal approach
- between ECU and EDM (extensor compartment 5 and 6)
- protect dorsal sensory branch of ulna nerve
- open extensor compartment
- proximal ulna osteotomy and resection 1 cm to allow rotation
- debrided lateral ulna and sigmoid notch of radius
- radioulna arthrodesis with screws
- interposition with pronator quadratus to create proximal ulna pseudoarthrosis
- +/- stabilized with slip ECU / FCU to prevent proximal ulna instability
Youtube open Suave-Kapanji procedure video
Vumedi arthroscopic Suave-Kapanji procedure video
Results
Reissner et al J Hand Surg Eur 2021
- 15 Suave Kapanji procedures followed for 13 years
- 6/15 required revision for proximal ulna stump instability
Interposition arthroplasty
Indication
Young, active patients
Technique
Dorsal approach
- between ECU and EDM (extensor compartment 5 and 6)
- open capsule over ulna head
- excise distal wafer of ulna head
- allograft secured to radius / sigmoid notch with suture anchors
- secured to ulna via drill holes
- can be wrapped around ulna in setting of instability
Vumedi interposition arthroplasty video
DRUJ Replacement
Options
Hemiarthroplasty
Total joint arthroplasty
DRUJ hemiarthroplasty
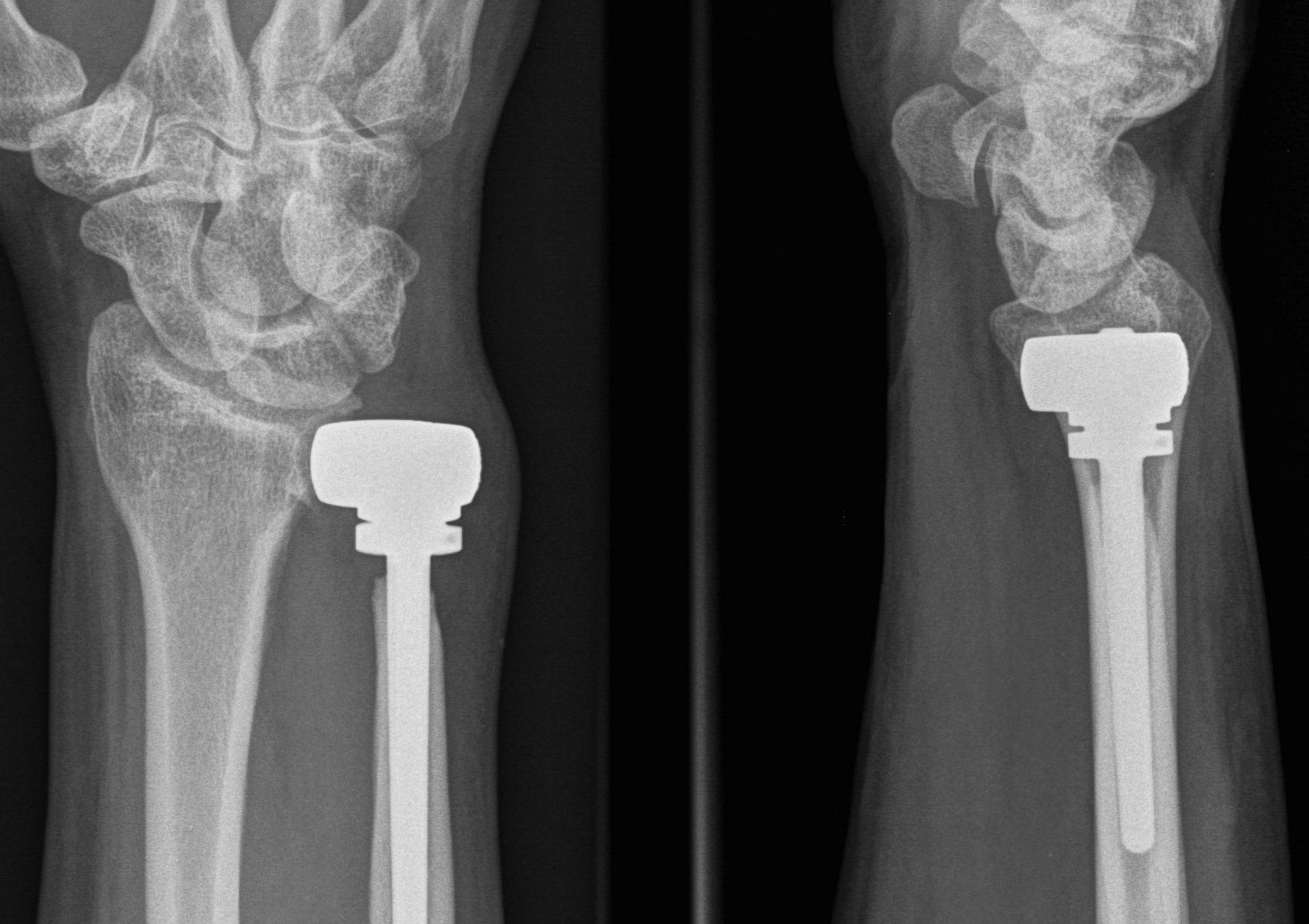
Technique total joint arthroplasty



Aptis DRUJ total joint arthroplasty
Dorsal approach
- between 5th and 6th extensor compartment
- open extensor retinaculum
- resect proximal ulna
- prepare radius and apply radial plate checking implant position with fluoroscopy
- intramedullary ream ulna
- press fit ulna prosthesis
Aptis DRUJ total joint replacement technique PDF
Vumedi Aptis DRUJ total joint arthroplasty video
Results
Stougie et al J Wrist Surg 2023
- 53 Aptis DRUJ total arthoplasty with 4 year follow up
- implant survival 92%
- revision surgery 41%
- complication rate 64%
- patient satisfaction 72%
- 32 DRUJ hemiarthroplasty followed for 3 years
- metallic implants: reoperation 10%, failure 30%
- pyrocarbon implants: reoperation 14%, failure 18%