Definition
Partial or complete rupture of one or more of the lateral ligaments of ankle
Epidemiology
Lateral ankle sprains are the most common ligamentous injuries
ATFL most commonly torn ligament in humans
Roos et al Am J Sports Med 2017
- 5 years NCAA
- 2429 lateral ankle sprains
- 480 high ankle sprains
- 380 medial ankle sprains
- basketball most common sport
Risk factors
- meta-analysis of 181 papers
- incidence of ankle sprains
- females > males
- children > adolescents > adults
- most common in indoor / court sports
Natural history
- up to 33% patients still have pain 1 year after acute ankle sprain
- up to 34% risk of recurrent ankle sprain
Thompson et al BMC Musculoskeletal Disord 2017
- prognostic factors associated with poor recovery after acute ankle sprain
- female, increased severity, swelling, limited weight bearing
- pain at 3 months
- reinjury within 3 months
- increase number of ligament injuries + bone bruise on MRI
Etiology
Inversion injury
- jumping sports
- foot plantarflexed and inverted
Associations
Pes Cavus
Tarsal Coalition
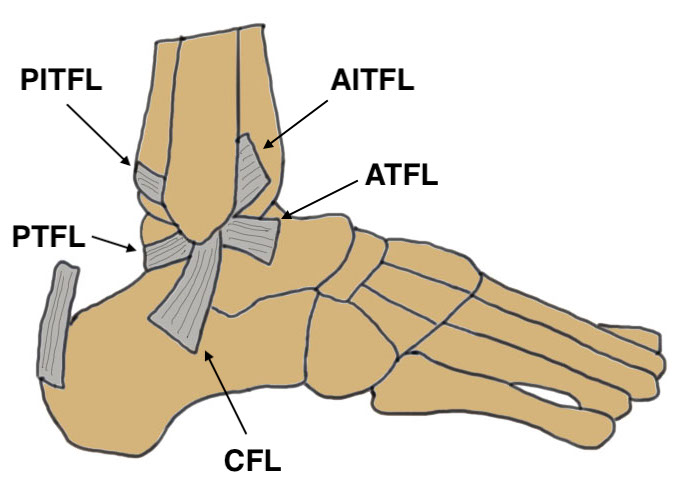
Anatomy
The ankle is a uniaxial joint that resembles a mortise and tenon
- very stable when loaded in the neutral position
- bony contact and stability decrease with plantar flexion
|
ATFL (Anterior talofibular ligament) |
CFL (Calcaneofibular ligament) |
PTFL (Posterior talofibular ligament) |
Deltoid | |
|---|---|---|---|---|
| Dimension |
15 to 20 mm long 6 to 10 mm wide 2 mm thick on average |
Cylindrical 20 to 30 mm long 3 to 5 mm thick 4 to 8 mm wide |
30 mm long 5 mm wide 5 to 8 mm thick |
20 - 30 mm long 10 mm wide 2 to 3 mm thick
|
| Origin |
Anterior margin lateral malleolus 1 cm above tip |
Tip of lateral malleolus | Medial surface lateral malleolus | Medial malleolus |
| Attachment | Lateral talar neck |
Deep to peroneal tendons Lateral aspect of calcaneum 13 mm below subtalar joint |
Posterior lip of talus |
Superficial - navicular / spring ligament / sustenaculum / calcaneum Deep - medial wall of talus |
| Action | Primary restraint to anterior displacement |
2.5 x stronger than ATFL Lateral ankle stability |
Strongest Least often injury |
Isolated injury rare |
Pathology
Most are mid-substance tears
- avulsion injuries occur in about 14%
Findings
- isolated ATFL tear is most common injury(60% to 70%)
- combined ATFL / CFL tear (20%)
- isolated CFL, PTFL, & subtalar ligament ruptures all very rare
Examination


Lateral ligament complex
- pain / tenderness
- lateral ankle swelling
- ligament testing - anterior drawer / talar tilt
| Anterior drawer | Talar tilt |
|---|---|
| Assess ATLF | CFL test / subtalar instability |
|
10° plantarflexion neutral rotation Draw talus anterior to tibia |
10-20° plantarflexion Ankle inversion |
| > 3mm difference to other ankle | > 20o difference to other ankle |
 |
 |
Deltoid ligament
- tenderness / bruising medially
Syndesmosis / high ankle sprain
- tender syndesmosis
- pain with external rotation foot
Grade
| Grade I | Grade II | Grade III |
|---|---|---|
|
Mild injury Minimal swelling Minimal tenderness |
Diffuse swelling Diffuse tenderness |
Marked swelling |
|
Negative anterior drawer / talar tilt Partial ATFL |
Positive anterior drawer Negative talar tilt ATFL tear +/- partial CFL |
Positive anterior drawer Positive talar tilt Rupture ATFL & CLF |
| Normal activities with pain |
Cannot perform normal activities Weight bear with pain |
Difficulty weight bearing |
X-rays
Ottawa rules for xray acute ankle sprain
- malleolar bony tenderness
- unable to weight bear
- bony tenderness
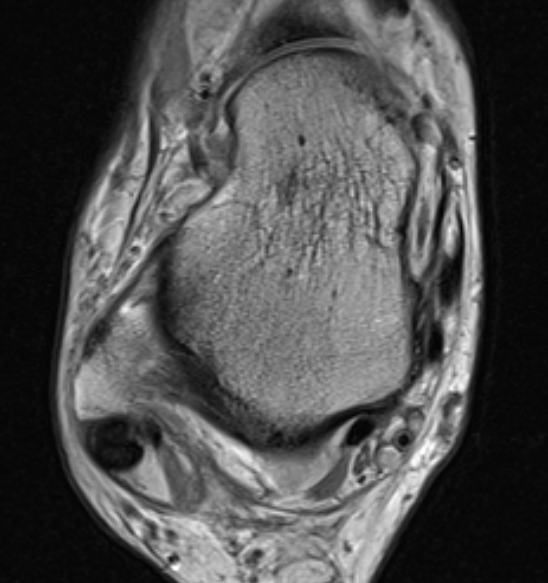
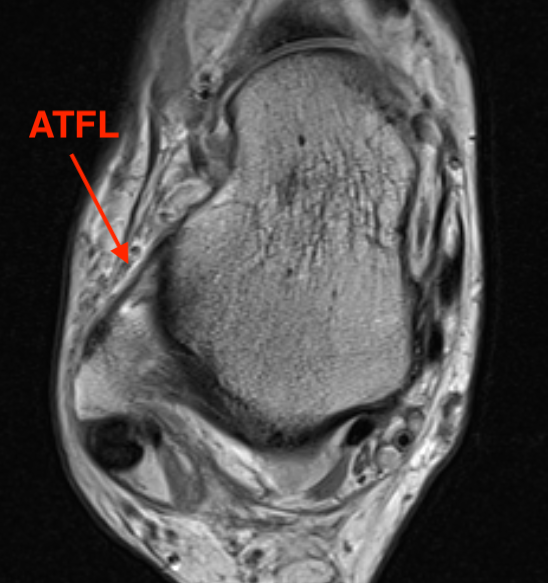
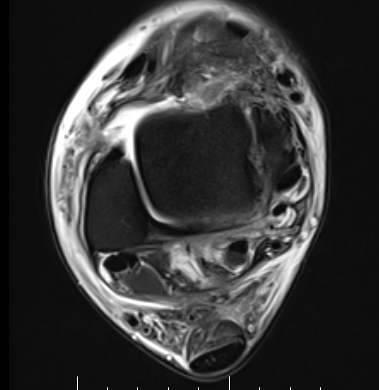
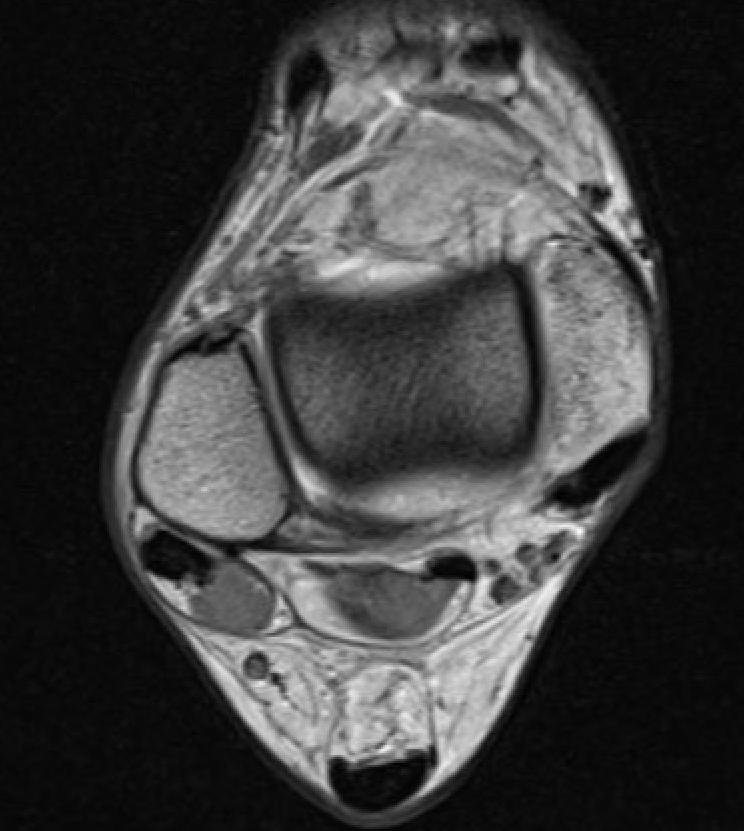
MRI
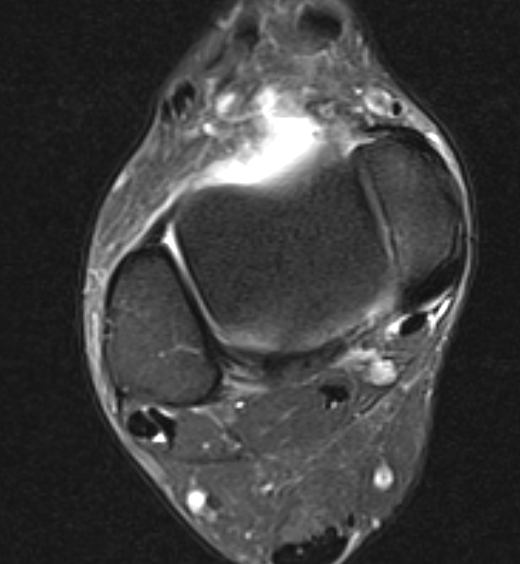
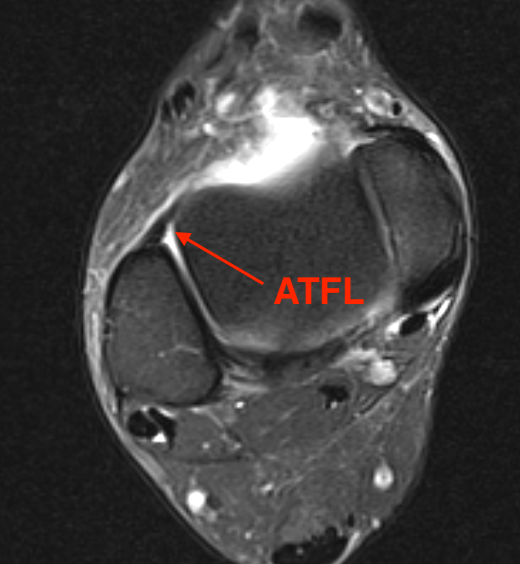


ATFL normal
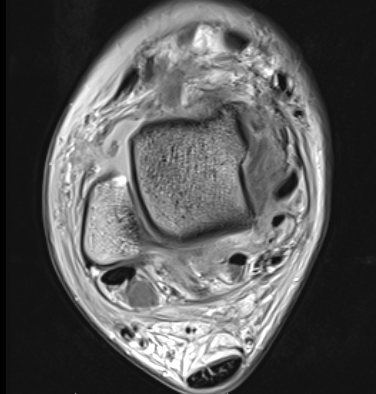
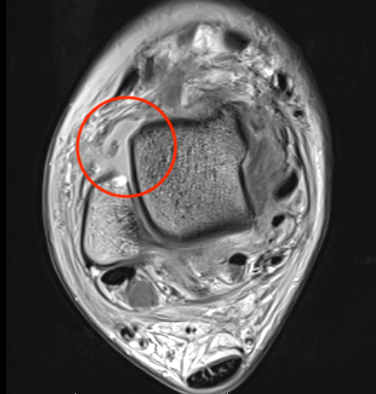
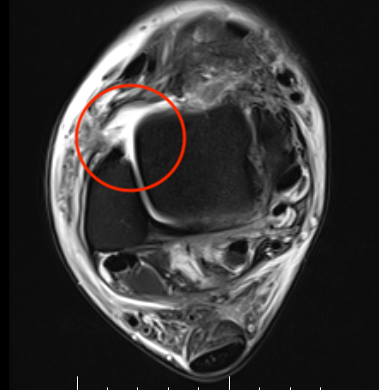
Torn ATFL

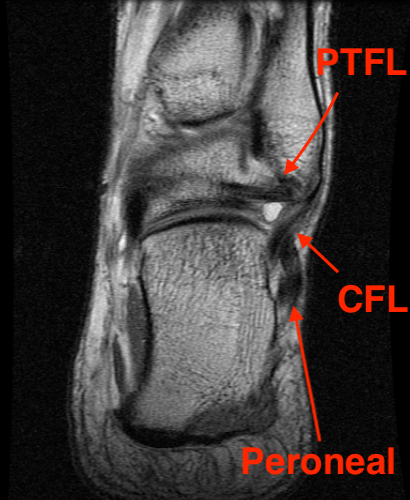


CFL


PTFL

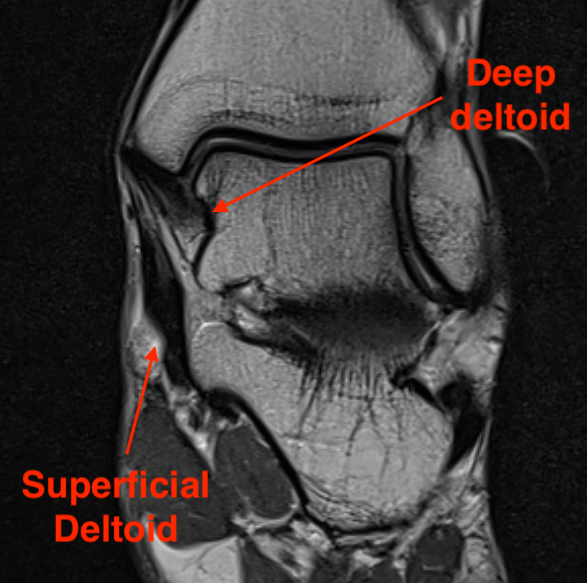
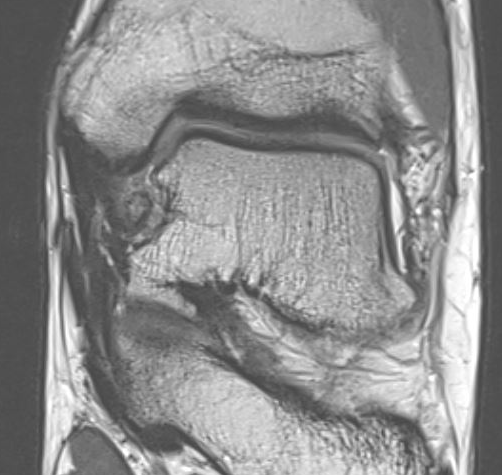
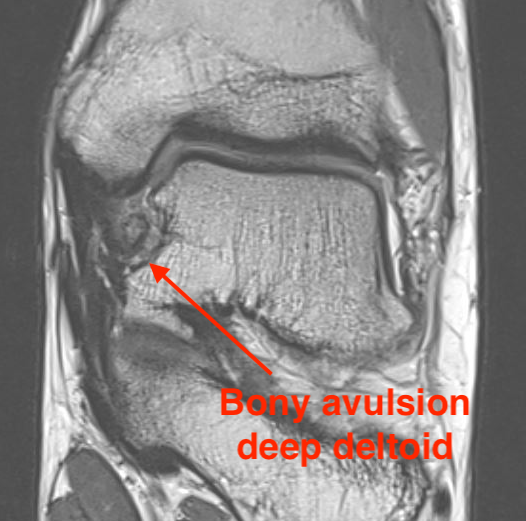
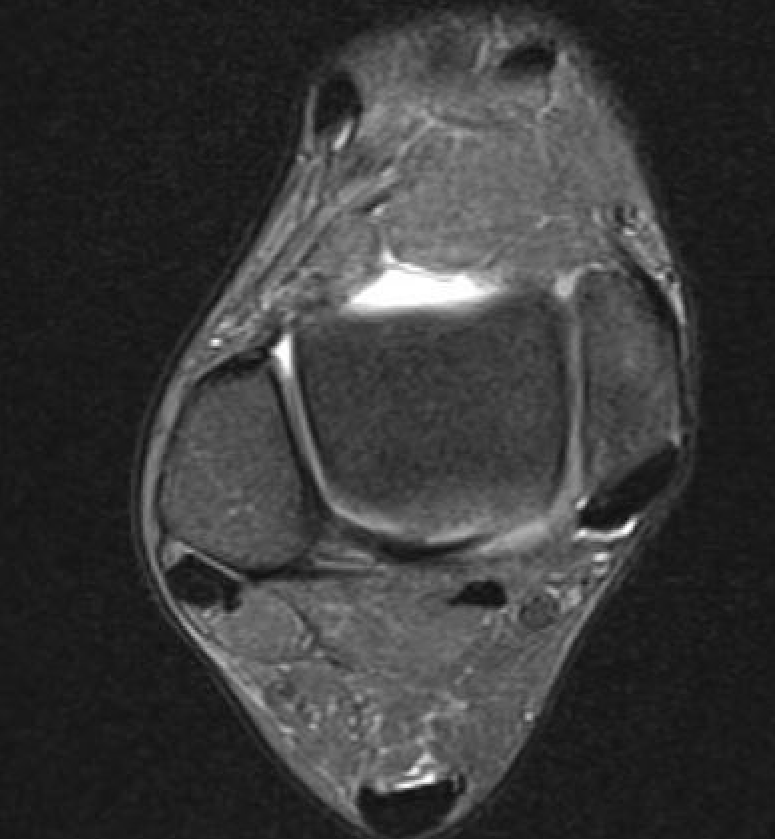
Deltoid ligament
Associated injuries
Osteochondral lesions
- MRI of 261 acute ankle sprains
- 40% complete ATFL tear
- 20% syndesmotic injury
- acute lateral talus osteochondral lesions 8%
- chronic lateral talus osteochondral lesions 1%
Management
Operative versus non operative management
Kerkhoffs et al Cochrance Database Systematic Review
- systematic review of operative v nonoperative management acute ankle sprain
- evidence early surgery improves stability
- evidence early surgery associated with longer recovery time / stiffness / complications
Non operative management
Goals
Return to function
Reduce recurrence / chronic ankle instability
Acute management


- systematic review of acute ankle sprains
- mild / moderate sprains - functional bracing / taping
- severe sprains - air cast for short period
Petersen et al Arch Orthop Trauma Surg 2013
- systematic review of 16 prospective RCT
- evidence for semi-rigid bracing for grade I / II
- evidence for 10 days immobilisation for grade III injuries
Prevention of recurrence
Brace / taping
Janssen et al Br J Sports Med 2014
- brace v proprioception exercises v both
- 384 athletes
- recurrence brace:15%
- recurrence proprioception program: 27%
- recurrence both: 19%
Rehabilitation exercises
Neuromuscular training / proprioception / postural balance / strengthening
Bleakley et al Arch Phys Med Rehab 2019
- systematic review of postural training / strengthening
- 7 RCTs and 1400 patients
- evidence that rehabilitation exercises reduce recurrence at 6 and 12 months
- RCT of 522 athletes with acute ankle sprain
- home proprioception program: recurrence 22%
- no home program: recurrence 33%