
Epidemiology
Uncommon - <1% of all physeal injuries
Adolescent boys 13 - 16
- sporting activities
Risk factors
- sporting activities
- Osgood-Schlatter disease
- obesity
Haber et al J Pediatr Orthop B 2021
- 236 tubercle fractures
- 87% male
- Osgood-Schlatter seen in 31%
Ossification
Proximal tibia - primary ossification center
Tibial tuberosity
- secondary ossification center appears aged 9 - 11
- tibial apophysis most vunerable to avulsion during adolescence
- eventually fuses with tibial physis in girls aged 15 and boys aged 17
Mechanism
Forceful eccentric contracture of the quadriceps
- initiating a jump or landing
- knee flexed
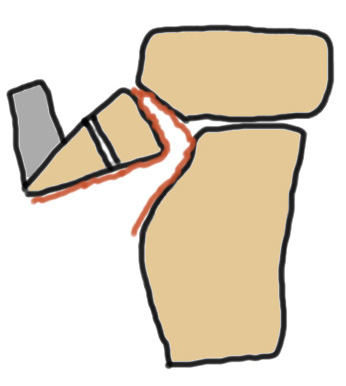
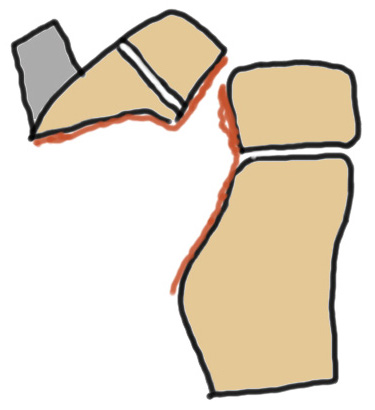
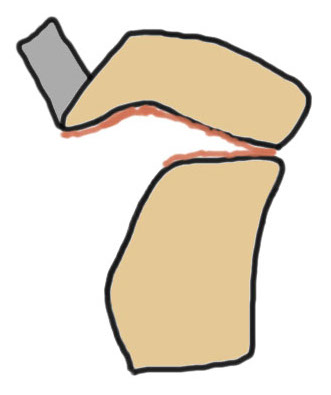
Ogden Classification
A: Undisplaced
B: Displaced
| Type I | Type II | Type III | Type IV |
|---|---|---|---|
| Avulsion distal tibial tubercle | Extension into tibial physis but not into knee joint | Extension across tibial physis and into knee joint | Extends posteriorly across tibial physis |
| Disrupts extensor mechanism | Disrupts extensor mechanism |
Disrupts extensor mechanism Disrupts articular surface Disrupts growth plate |
Disrupts extensor mechanism Disrupts articular surface Disrupts growth plate |
|
Associated Osgood-Schlatter Second most common |
Most common Risk of compartment syndrome |
Risk of compartment syndrome |
|
 |
 |
 |
 |
 |
 |
 |
Haber et al J Pediatr Orthop B 2021
- 236 tubercle fractures
- Type III most common 41%
- Type I second most common 29%
Associated injuries
Compartment syndrome
Injury to the anterior recurrent tibial artery
- runs lateral border of tibial tubercle
- compartment syndrome seen after injury, not after surgery
Pretell-Mazzini et al J Pediatr Orthop 2016
- systematic review of 300 cases
- compartment syndrome 4%
Haber et al J Pediatr Orthop B 2021
- 236 tubercle fractures
- compartment syndrome most common Type IV
Frey et al J Child Orthop 2008
- 4 cases of preoperative compartment syndrome
- Type IIA, Type IIB and Type IV
Patella tendon injuries
- systematic review of 950 cases
- associated injuries 10%
- most common patella tendon avulsion
Meniscal tears
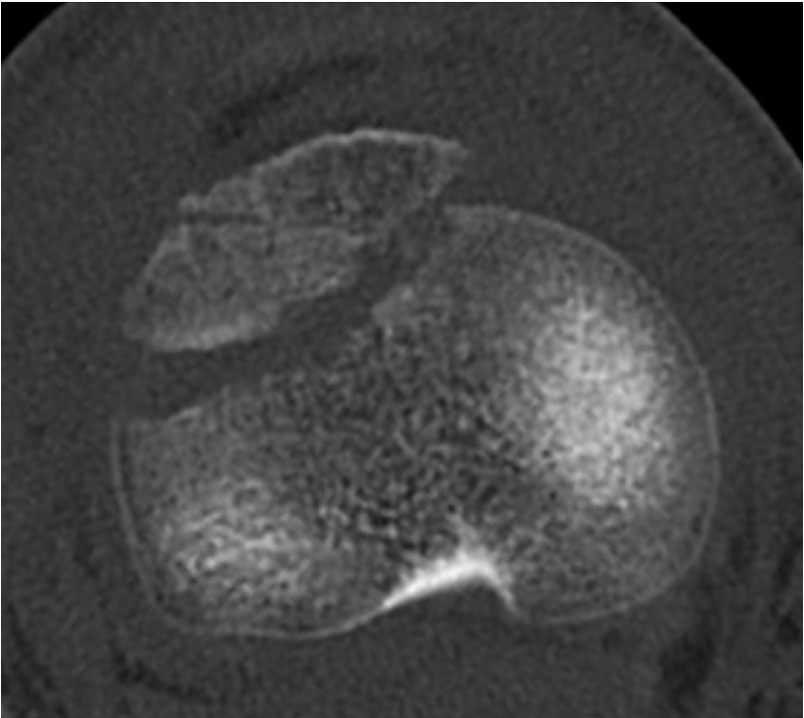
CT / MRI scan
CT scan - ensure fracture doesn't involve the physis / disrupt articular surface
MRI scan - patella tendon injury / periosteal sleeve avulsion


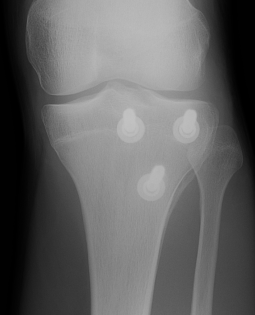
Type IB


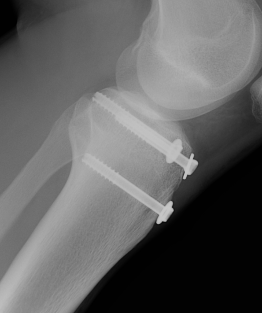
Type IIB


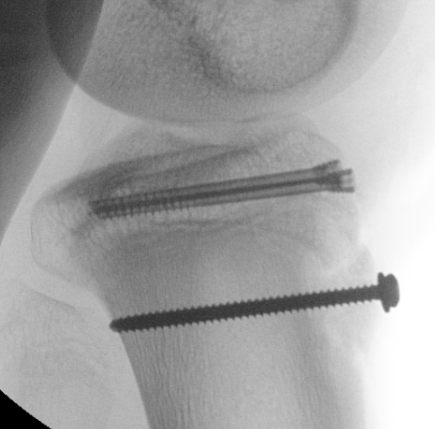
Type III

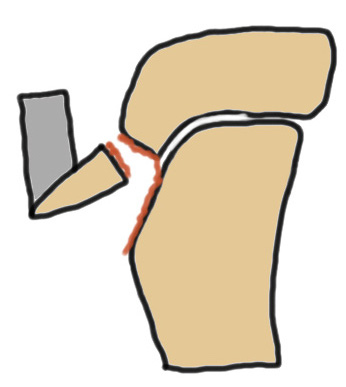
Comminuted Type III
Nonoperative management
Indications
Minimally displaced Type I / Type II < 2 mm



Technique
Cast in extension for 4 - 6 weeks
Results
Pretell-Mazzini et al J Pediatr Orthop 2016
- systematic review of 300 cases
- refracture in 6% treated non operatively
Operative management
Indications
| Displaced Type I &Type II | Type III | Type IV |
|---|---|---|
| Restore extensor mechanism | Restore articular surface | Restore alignment |
|
 |
Type I /Type II
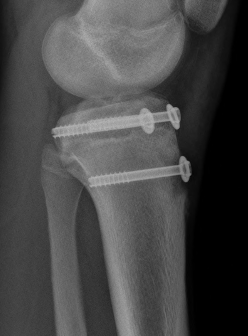
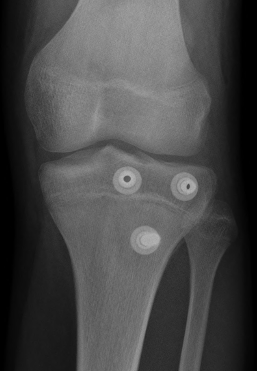
Technique
Vumedi tibial tubercle fixation video
AO surgery reference tibial tubercle fixation
Screw +/- anchor fixation +/- tension band fixation of tibial tubercle and patella tendon
- screw +/- washer in fragment if large
- can supplement with Krackow sutures in patella tendon and fixed distally with suture anchors
Type III
Technique
POSNA Type III tibial tubercle fixation video
Restore articular surface
- may need to visualize joint line with arthrotomy / arthroscopy
- pass guide wires for screws into epiphysis and tibial tubercle
- image intensifer to ensure reduction / growth plate protection / no penetration to posterior neurovascular structures
- secure with AP screws in tibial epiphysis through vertical split in patella tendon
- unicortical fixation to protect popliteal artery
- restore tibial tuberosity with screws +/- washer
Results
Union
- systematic review of 956 cases
- 88% managed with surgery
- union in 954/956 (99.8%) of fractures
Fixation
Arkader et al J Pediatr Orthop 2019
- 90 fractures treated with screw fixation
- 100% union
- no difference in unicortical versus bicortical fixation
Return to sport
- systematic review of 956 cases
- return to sport 99%
Type IV
Pace et al J Pediatr Orthop 2013
- 23 Type IV treated with surgery
- ORIF with screws
- 4 patients required supplemental plate fixation
- 1 compartment syndrome, 1 DVT
- 100% union
- no growth disturbances
Complications
Infection
Hardware prominence
Numbness
Compartment syndrome
Bergen et al J Pediatr Orthop 2024
- 46 cases of tibial tubercle fixation at average 3.5 days post injury
- no cases of postoperative compartment syndrome
- suitable for day surgery
Zukotynski et al J Child Orthop 2023
- 71 cases of tibial tubercle fixation
- half day surgery
- no cases of postoperative compartment syndrome
Popliteal artery injury
Haber et al J Pediatr Orthop B 2021
- 236 tubercle fractures
- one case due to AP drilling
Stiffness
Brnjos et al JBJS Open Access 2025
- 369 patients with tibial tuberosity fractures
- stiffness (>20 degrees loss of flexion) 3%
- immobilization > 4 weeks: stiffness 6%
- immobilization < 4 weeks: stiffness 1%
Huang et al J Pediatr Orthop 2022
- 134 patients with tibial tuberosity fractures
- all treated with screw fixation
- early ROM (< 4 weeks) versus late ROM (> 4 weeks)
- no difference in outcome
Growth plate arrest / genu recurvatum
Relatively uncommon
- injury usually occurs near time of physeal closure
- more likely to cause issues in patients under 13
Pretell-Mazzini et al J Pediatr Orthop 2016
- systematic review of 300 cases
- 4 cases of physeal closure and genu recurvatum