Etiology
Elbow fractures treated with surgery
- distal humerus
- radial head / neck
- terrible triad
- proximal ulna fracture dislocations
Burns
Traumatic brain injury / spinal cord injury
Incidence
Hong et al Orthop Traumatol Surg 2015
- 124 surgically repaired elbow fractures
- HO 30%
- clinically relevant HO 20%
Symptoms
Restricted ROM
Ulna nerve symptoms - ulna nerve can be entrapped
Prevention
Indomethacin
- RCT of 164 patients with surgical management of elbow trauma
- postoperative indomethacin v placebo
- no difference in incidence of HO at one year between groups
- HO indomethacin: 49%
- HO placebo: 55%
Radiation therapy
- RCT of 7 Gray single dose 3 days post elbow trauma surgery v nothing
- early termination
- nonunion rate radiation: 38%
- nonunion rate control: 4%
Diffential diagnosis
Parosteal osteosarcoma - bone is contiguous with cortical bone
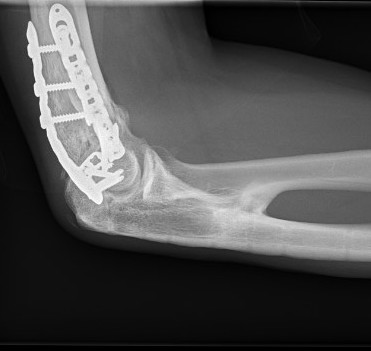
Xray



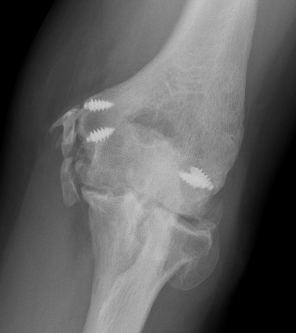

Radio-ulna synostosis

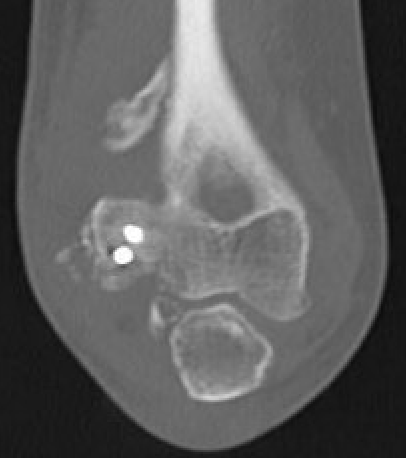
CT
Define anatomical location of the HO prior to surgical excision



- 56 elbows with post fracture HO
- 3D dimensional CT scans
- medial capsule 93%, lateral capsule 80%
- medial supracondylar 57%
- lateral supracondylar, radial head ulnar region 50%
Surgical management of heterotopic ossification
Timing
There is some evidence that delaying surgery > 12 months is unnecessary
Mature bone
- smooth well demarcated edges on xray
- cold on bone scan
- normal serum alkaline phosphatase
Results
He et al Acta Orthop Traumatol 2017
- 42 cases of surgical release of elbow HO
- < 12 months (mean 7 months) versus > 12 months (mean 33 months)
- better improvement in ROM with early group
- 77 cases of surgical release of elbow HO
- worse outcomes with delay > 19 months
- 164 cases of surgical release of elbow HO
- early excision (mean 6 months) versus late excision (mean 23 months)
- no difference in recurrence rates or outcomes
Post resection prophylaxis
Indomethacin - 25 mg tds for 4 weeks
Radiotherapy - 7 Gray single dose post operatively
Technique
Depends on site of ectopic bone
AO foundation surgical release of elbow HO
Universal posterior approach
Lateral approach
- Kaplan approach - interval between ECRB and EDC
- anterior capsulectomy
- elevate triceps and aconeus posteriorly
- posterior capsulectomy
Medial approach
- ulna nerve release
- over the top approach - elevate anterior half of flexor pronator mass
- posteriorly elevate triceps


+/- hinged external fixator

Results
Outcomes
Baldwin et al J Hand Surg Am 2011
- 64 cases of surgical release of elbow HO
- average ROM gain 49 degrees
- infection 6%
- 13% recurrence of HO
- revision surgery 11%
- recurrence rates higher in patients with neurological injury
Complete elbow ankylosis
Shivdasani et al JSES Int 2024
- 107 cases of elbow HO with complete elbow ankylosis undergoing HO resection
- 75% achieved ROM of 100 degrees
- patients maintained 95% of intra-operative ROM
- average extension loss of 20 degrees
Ulna nerve entrapment
- 32 elbows with HO and bony ulna nerve encasement undergoing HO resection
- post operative indomethacin
- ROM improved from 21 to 100 degrees
- 63% of patient's ulna nerve symptoms improved
Radio-ulna synostosis
Definition
Fusion between radial and ulna that limits rotation
Risk factors
High energy injury / comminution / open fractures
BBFF at same level / Monteggia
Traumatic brain injury
Delay in surgical treatment
Management
Excision
- wait for maturation between 1 and 2 years
- resection of synostosis
- +/- interposition bone wax / fat / fascia / vascularized graft
- +/- postoperative NSAIDS / radiation
Results
- excision of synostosis in 18 limbs
- no NSAIDS or irradiation postoperative
- recurrence in 1 patient with traumatic brain injury
- no evidence of efficacy of fat graft interposition
- possible better results with earlier surgery