

Definition
Elbow dislocation with concomitant fractures
Inherently unstable
Injury patterns
Elbow dislocation + radial head fracture
Elbow dislocation + coronoid process fracture
Terrible triad - elbow dislocation + MCL injury / coronoid process fracture / radial head fracture
Elbow dislocation + proximal ulna fracture - Monteggia / Monteggia variant
Elbow dislocation with radial head fracture
Management
Critical to elbow stability
Based upon Mason classfication
www.boneschool.com/radial-head-fractures
Mason Classification
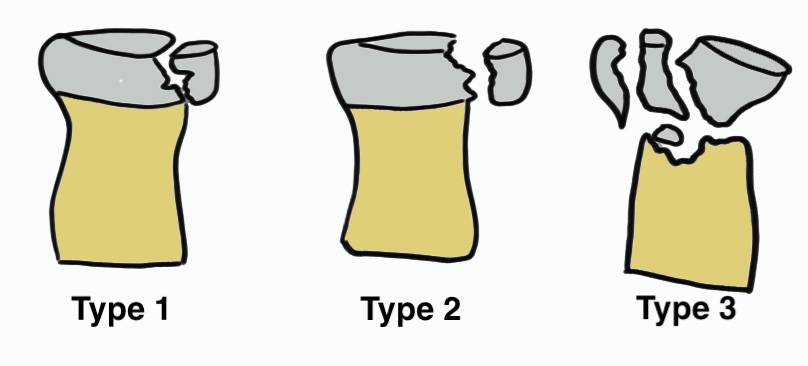
| Type 1 | Type II | Type III |
|---|---|---|
|
Minimally displaced fracture < 2 mm No block to rotation |
Displaced fracture radial head > 2 mm Reconstructable |
Comminuted fracture radial head Unreconstructable |
| Non operative |
ORIF + LCL repair / reconstruction +/- MCL repair / reconstruction if unstable |
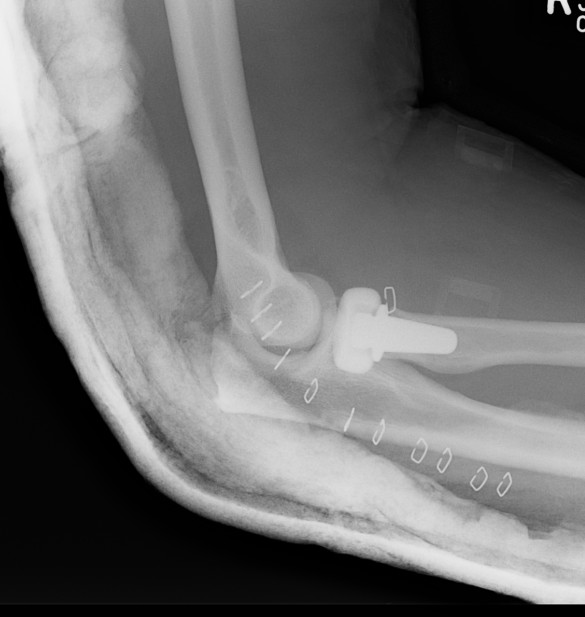
Radial head replacement + LCL repair / reconstruction +/- MCL repair / reconstruction if unstable
|
 |
 |
 |
 |
 |
Results
- 450 cases of radial head arthroplasty
- revision rate 18% for terrible triad versus 10% isolated cases
- increasing radial head diameter associated with increasing revision rate
- systematic review of radial head ORIF v replacement in terrible triad
- better functional outcomes and lower complications with radial head arthroplasty
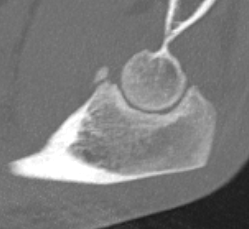
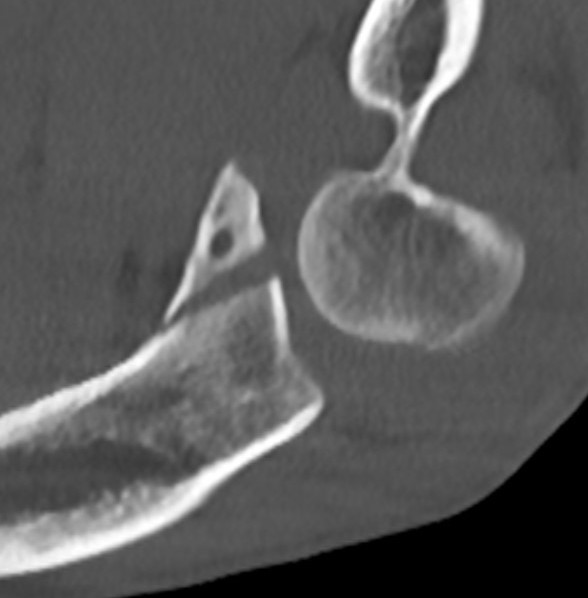
Elbow dislocation with coronoid process fracture

Coronoid process
www.boneschool.com/coronoid-process-fractures
Coronoid is the most important portion of ulno-humeral articulation
- provides anterior buttress
- attachment of capsule and brachialis
- anterior band of the MCL attaches to it
Regan and Morrey classification of transverse coronoid fractures
Elbow stability related to size of coronoid fragment
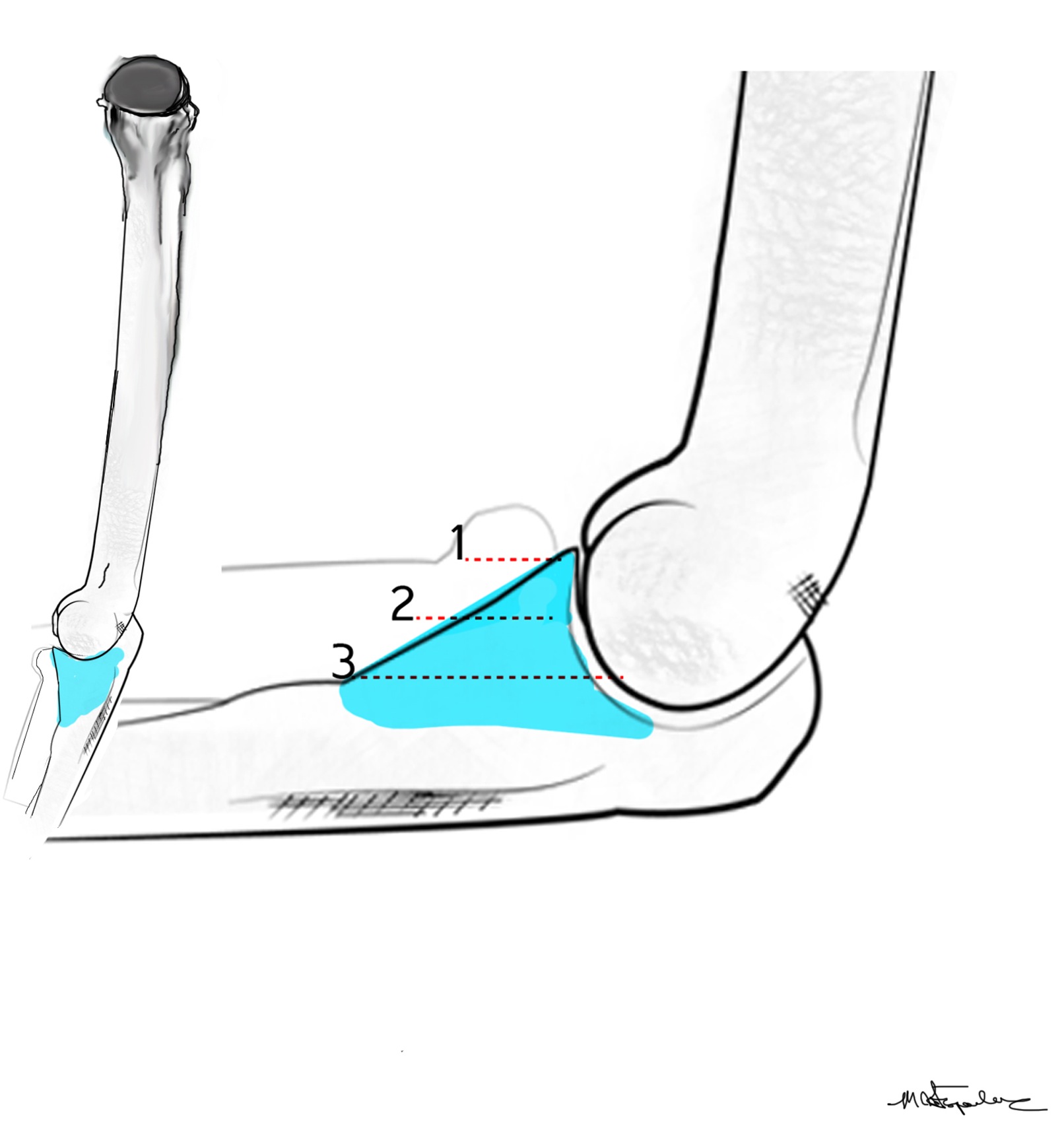
| Type I | Type II | Type III |
|---|---|---|
| Small coronoid process fracture | 50% of coronoid process | > 50% coronoid process |
| Usually stable |
Capsular attachment Elbw may be unstable |
Capsule + MCL attachment Elbow unstable
|
 |
 |
 |
 |
 |
 |
O'Driscoll classification anteromedial coronoid facet fractures
| Type I | Type II | Type III |
|---|---|---|
| Transverse fractures | Anteromedial facet fractures | Basilar fractures |
| Lasso suture fixation |
Lasso suture fixation - small Medial buttress plate / screws - large |
Dorsal +/- medial plate |
 |
 |
 |
Anteromedial coronoid facet fragment
- associated with varus posteromedial rotational force
- associated with tear of lateral ulna collateral ligament (LUCL)
Approach
Approach options for coronoid fixation
- radial head arthroplasty - lateral approach through radial head
- olecranon fracture - through fracture bed
- medial approach - coronoid fixation without radial head fracture
Medial approaches
| Hotchkiss over the top | FCU split | Taylor and Scham |
|---|---|---|
|
Split flexor pronator mass - interval between FCU and palmaris longus - elevate pronator teres / FCR / palmaris longus - +/- detach from medial epicondyle - open capsule - detach brachialis from anterior coronoid process
|
Dissect out ulna nerve - follow into FCU - open two heads of FCU - elevate flexor pronator mass off capsule - open capsule - detach brachialis from anterior coronoid process
|
Elevate entire flexor - pronator mass - subperiosteal elevation from ulna - posterior to anterior
|
|
Access to tip of coronoid
|
Access to anteromedial facet | Access to base of coronoid |
AO surgery reference medial approach to coronoid
Vumedi Hotchkiss over the top coronoid fixation video
Vumedi FCU split coronoid fixation video
Vumedi Hotchkiss over the top coronoid fixation video
Vumedi medial approach to coronoid + lasso fixation + plate video
Fixation
Lasso suture - suture fragment, use ACL guide to direct drill holes through olecranon to base of coracoid
Screws - PA screws into fragment
Buttress plate


Coronoid buttress plates
Terrible Triad


Definition
Elbow dislocation with radial head fracture + coronoid fracture + MCL tear
Technique
www.boneschool.com/radial-head-fractures
www.boneschool.com/coronoid-process-fractures
www.boneschool.com/elbow-external-fixation
Vumedi terrible triad repair radial neck ORIF + coronoid lasso + LCL internal brace repair video
Skin incisions
1. Lateral
- Kocher / Kaplan / EDC split
- for radial head / coronoid / LUCL
2. Medial
- FCU split / split flexor pronator mass / detach entire flexor pronator mass
- for medial approach to coronoid +/- MCL if needed
3. Universal Posterior Approach - make medial and lateral skin flaps for medial and lateral approach
Surgical Algorithm
Principles
1. Restore coronoid stability - ORIF type II / III, suture repair type I
2. Restore radial head stability - radial head ORIF or arthroplasty
3. Restore lateral stability - LCL repair and common extensor origin +/- reconstruct +/- internal brace
4. +/- Restore medial stability - repair MCL if residual stability
5. +/- External fixation / internal joint fixation
| Type II / Reconstructable radial head | Type III / Radial head arthroplasty |
|---|---|
|
Lateral / Kocher approach - ORIF radial head with screws/ plate - LCL +/- common extensor origin repair - reassess stability |
Lateral / Kocher / Kaplan / EDC split approach - excise radial head - can suture small coronoid process fracture through gap - radial head replacement - LCL +/- common extensor origin repair - reassess stability
|
|
Unstable - medial approach - FCU split / over the top approach to coronoid process - ORIF coronoid process with sutures / buttress plate / screws - MCL repair +/- common flexor origin repair - reassess stability |
Unstable - medial approach - FCU split / over the top approach to coronoid process - ORIF coronoid process with sutures / buttress plate / screws - MCL repair +/- common flexor origin repair - reassess stability |
| Unstable - external fixation | Unstable - external fixation |


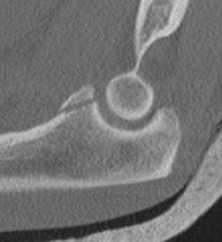
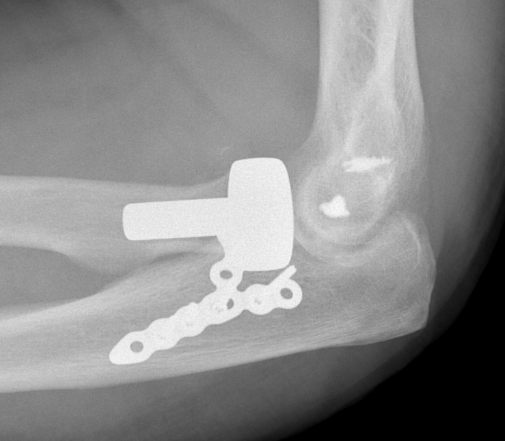
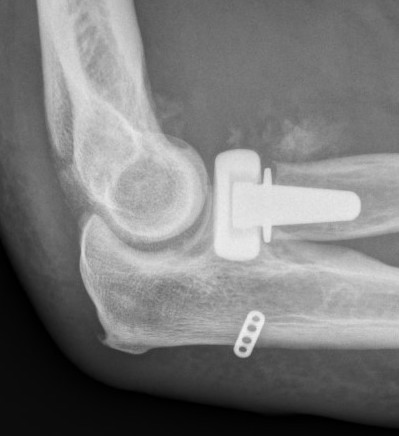
Radial head replacement with lag screw fixation of Type II coronoid


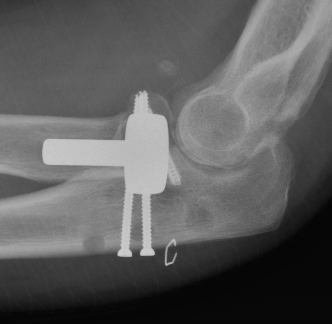
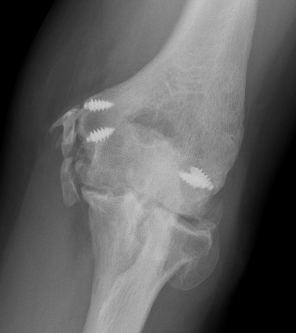
Radial head replacement with lasso fixation of small coronoid fragment
Results
Outcomes
- systematic review of terrible triad injuries
- mean flexion arc 110 degrees
- 30% complication
- 8% revision
- 11% HO
- 3% ulnar nerve

Coronoid process - only fix type III?
Antoni et al Orthop Traumatol Surg 2019
- 30 patients with terrible triad and Type I coronoid process
- some coronoid tip suture, some not
- no difference between two groups
- recommend no need to fix Type I coronoid process fractures
- 14 terrible triad with 2 type I and 12 type II coronoid process fractures
- no surgery to coronoid process
- LCL + radial head surgery, no MCL or external fixator
- no recurrent instability
- recommend surgery for type III coronoid process fractures only
- 24 terrible triad with radial head surgery / LCL repair +/- MCL repair
- only type III coronoid process repair (4/24)
- no recurrent instability
External fixation
- 26 patients with complex elbow dislocation required external fixators
- mean loss of range of motion 30 degrees
- 37% complications
- 26% secondary surgery
- 1 recurrent instability
Dislocation with olecranon fracture
www.boneschool.com/proximal-ulna-fracture-dislocations