Definitions
Massive tear
- > 5cm or retracted glenoid margin
- likely not reparable
Irreparable
- not able to be completely repaired despite modern techniques
- some large tears are not reparable depending on chronicity and patient size
Posterosuperior defects
- most common, involve infraspinatus and supraspinatus
Examination

Pseudoparalysis



Supraspinatus and infraspinatus wasting
Infraspinatus tear
- + Hornblower's sign
- external rotation lag
X-ray
Reduced acromiohumeral space / superior migration of the humeral head

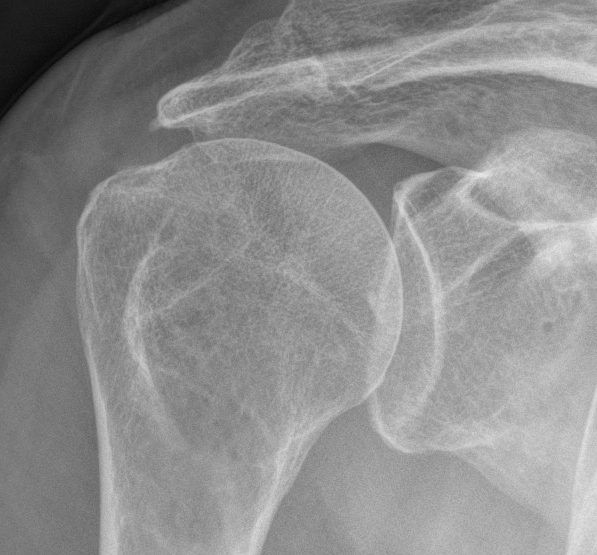
Rotator cuff arthropathy - acetabularization of the acromion


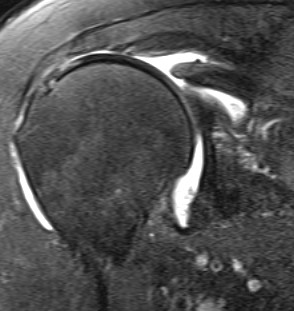
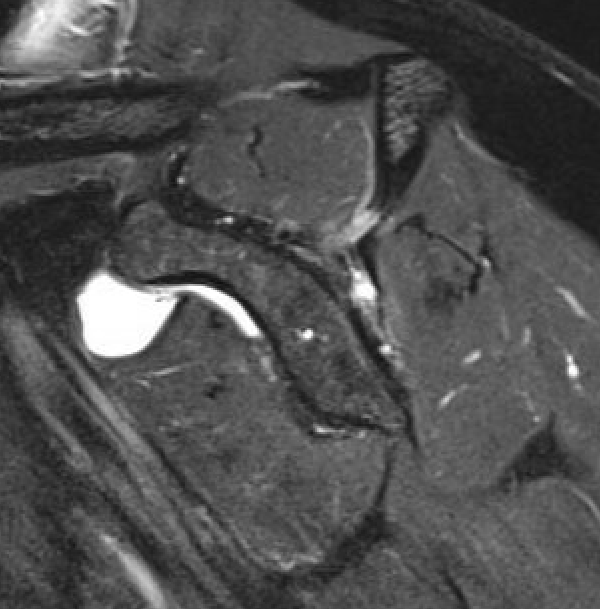
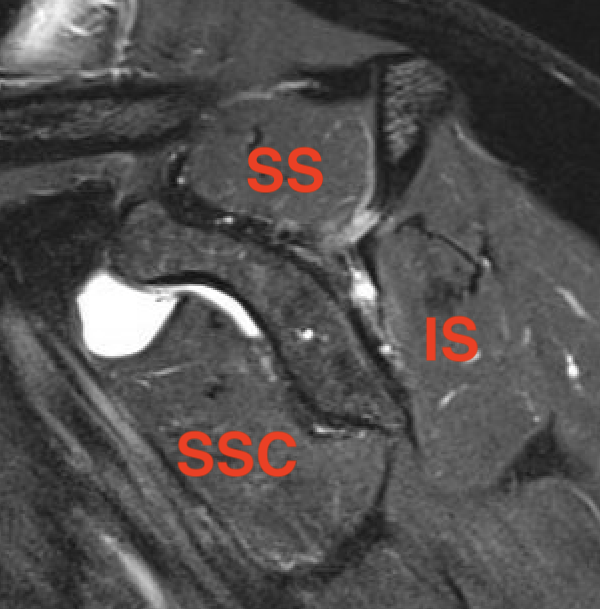
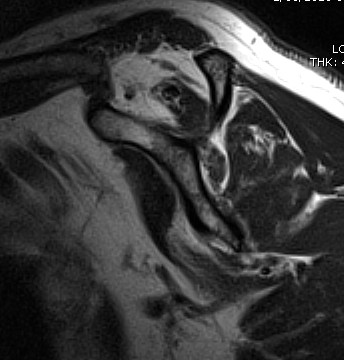
MRI
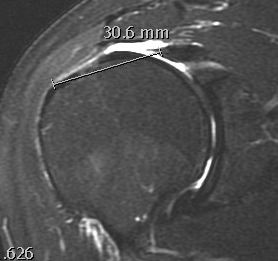
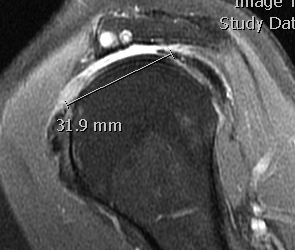
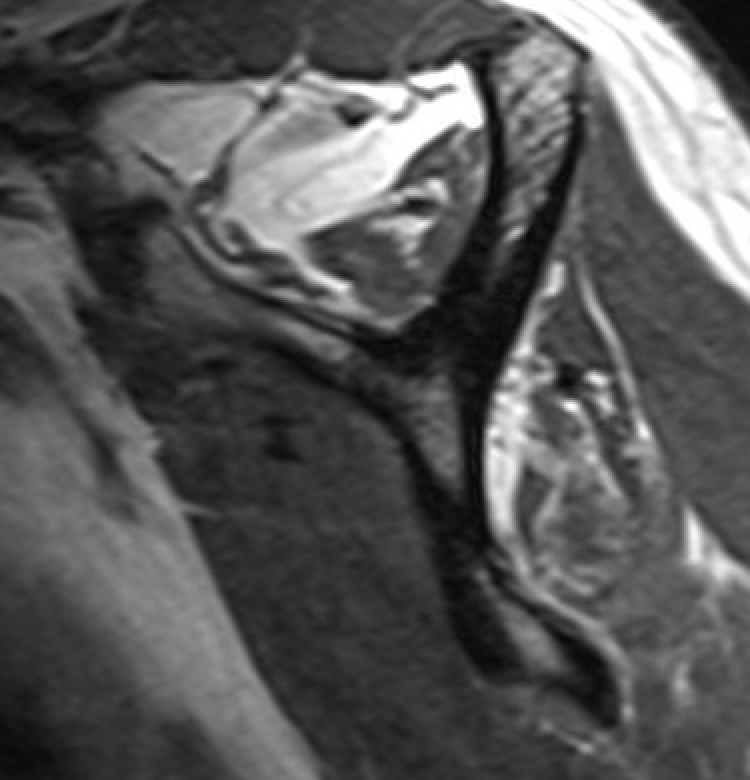
Measure tear in the coronal and sagittal plane

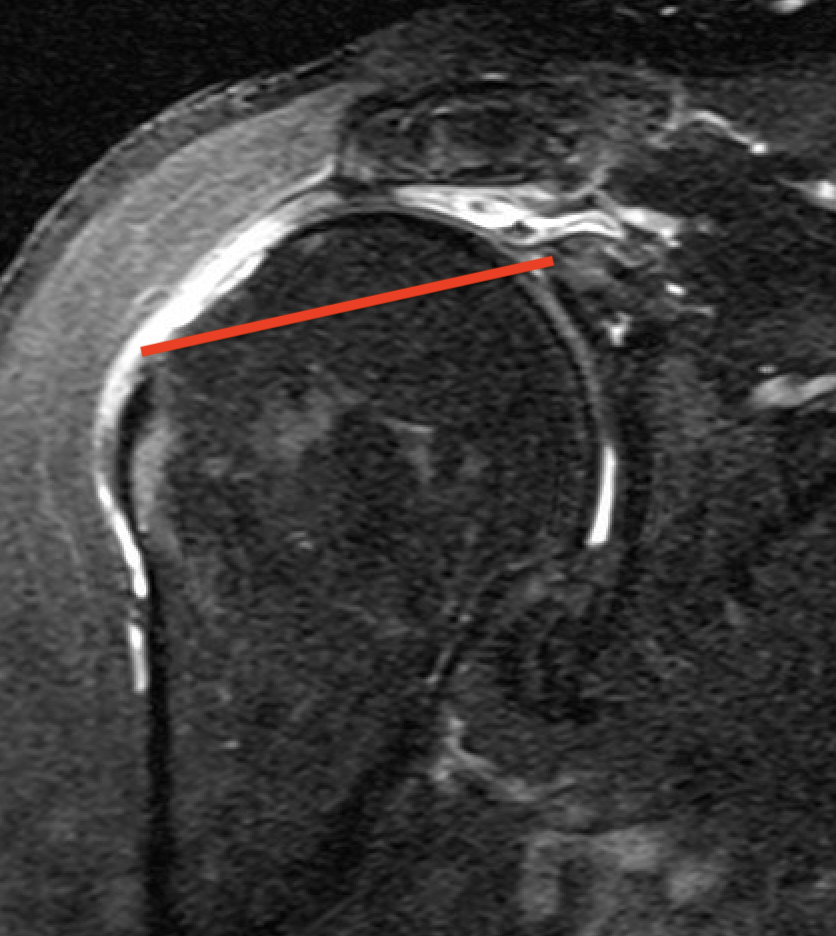
Massive rotator cuff tear of the supraspinatus and infraspinatus tendon - retracted to glenoid
Goutallier classification
Amount of fatty degeneration in rotator cuff muscle belly on a T1 sagittal MRI
Stage 0: normal muscle
| Stage 1 | Stage 2 |
|---|---|
|
Some fatty streaks MRI shows some fatty streaks in supraspinatus |
More muscle than fat MRI shows grade 2 in supraspinatus |
 |
 |
| Stage 3 | Stage 4 |
|---|---|
|
Equal fat and muscle MRI demonstrates grade 3 supraspinatus and infraspinatus |
More fat than muscle MRI demonstrates grade 4 infraspinatus |
 |
 |
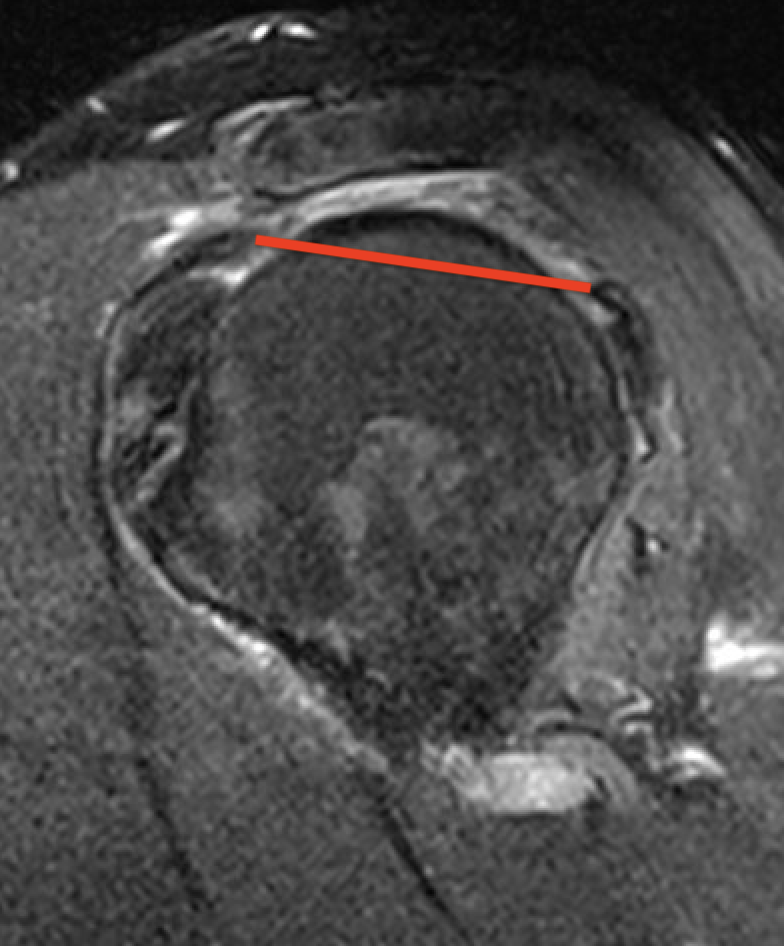
Supraspinatus atrophy
Tangent sign
- sagittal MRI
- line connecting superior coracoid and superior border scapular spine
- if supraspinatus muscle is below line, there is significant atrophy
- positive tangent sign / significant atrophy associated with larger tears / irrepairable tears
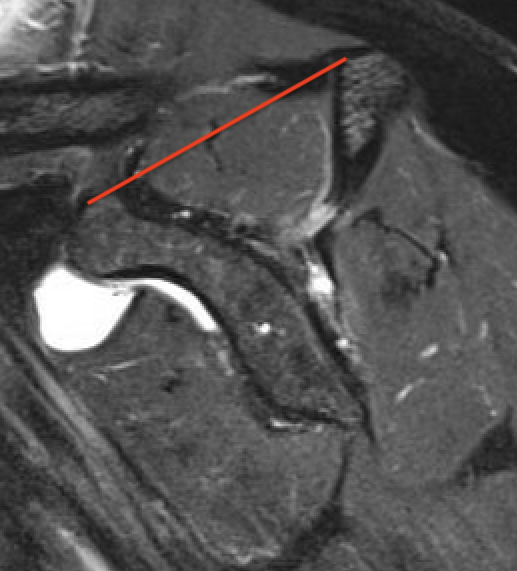
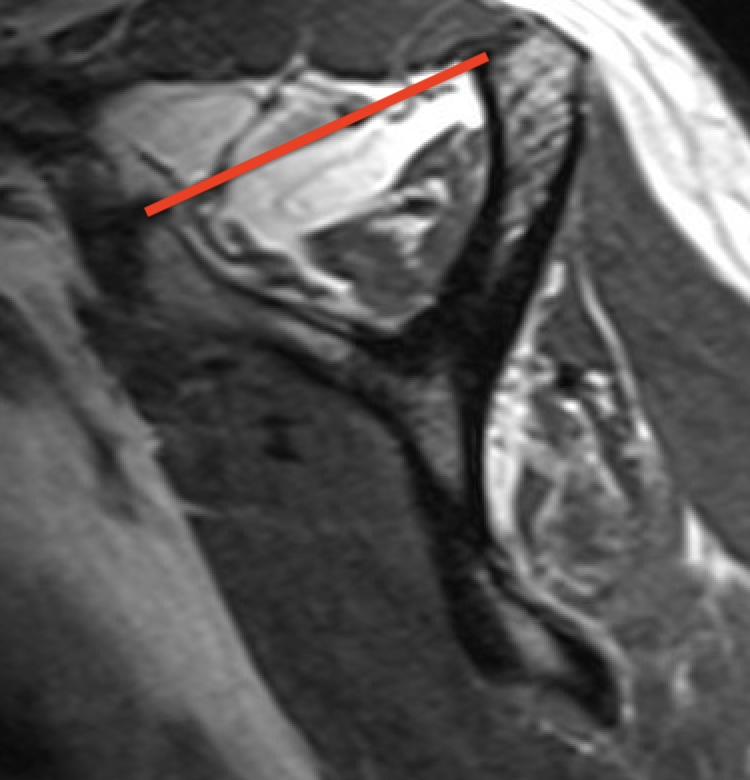
Negative tangent / no atrophy Positive tangent / significant supraspinatus atrophy
MRI predictors of reparability
- 60 patients with large and massive tears
- irreparability associated with retraction to or beyond glenoid
- irreparability associated with tangent sign / advanced fatty infiltration / superior migration humeral head
- 120 patients with large and massive tears
- irreparability associated with modified grade III Patte (retraction to medial 5th humeral head)
- associated with 94% chance or irreparability
- irreparability also associated with reduce acromiohumeral distal / superior migration humeral head
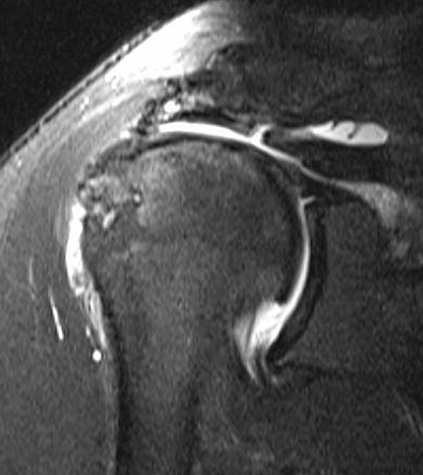
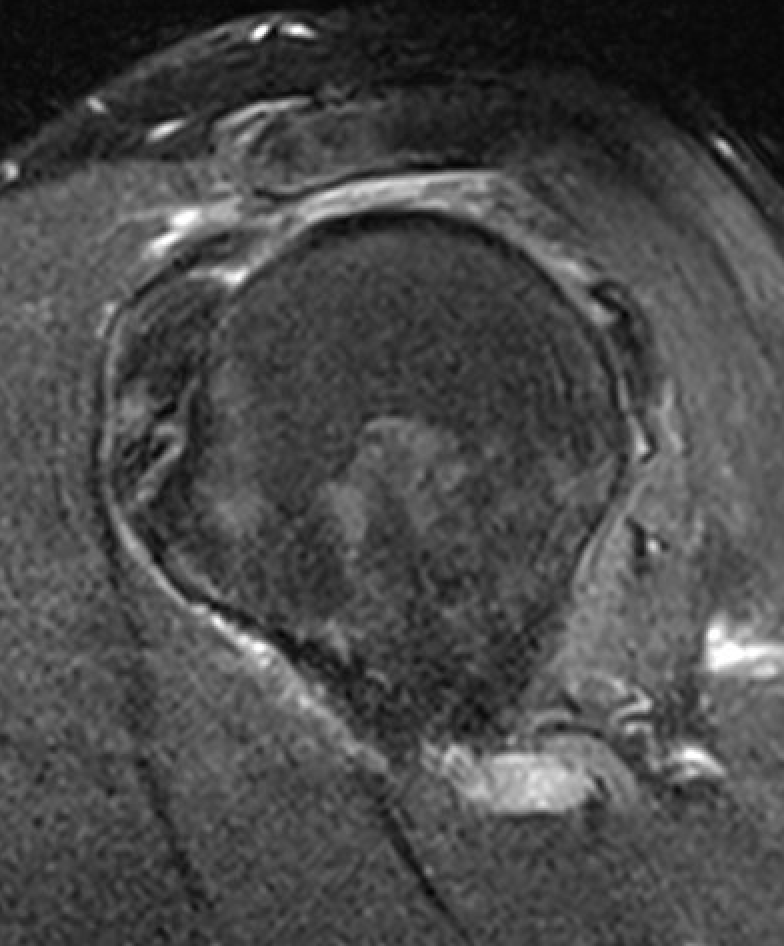
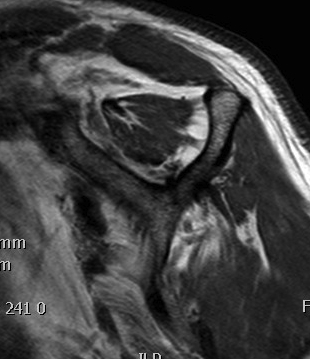
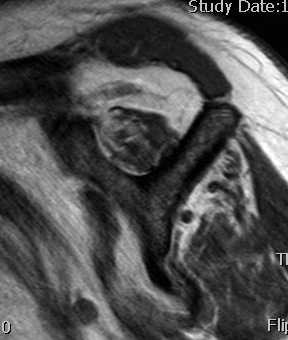
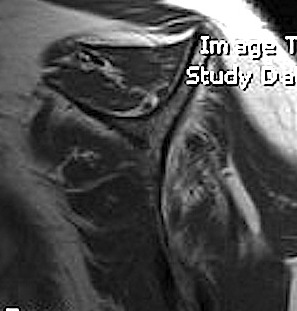
Examples of rotator cuff tears that are likeley irreparable
Non operative management
Physiotherapy
- prospective cohort study of 450 patients with symptomatic full-thickness atraumatic cuff tears
- 6-12 weeks of physiotherapy
- only 27% elected for surgery (most in first 6 months)
- low expectation of physiotherapy, workers comp., and high functional demand predicted later surgery
Injections
Jiang et al J Orthop Surg Res 2023
- systematic review of cortisone v HA v PRP for rotator cuff tears
- 12 RCTs and 1000 patients
- short term pain relief with HA
- longer term pain relief and functional improvement with PRP
Operative management
Options
Partial rotator cuff repair +/- biceps augmentation
Tendon transfer
- latissimus dorsi tendon transfer (LDTT)
- lower trapezius transfer (LTT)
Superior capsular reconstruction (SCR)
Balloon spacer
Reverse TSA
Results
SCR versus LDTT
- systematic review of SCR v LDTT
- 1000 patients
- better outcomes with SCR and lower infection rate (0.2 v 3%)
- higher graft failure with SCR (12% v 7%)
- 42 patient RCT of SCR v LDTT
- better outcome scores with SCR
SCR v LTT
- 22 SCR v 36 LTT
- better ROM and functional outcomes with LTT
- reduced progression to OA with LTT (3% v 23%)
- lower graft retear with LTT (8% v 64%)
- 32 SCR v 72 LTT
- better pain relief and flexion with SCR
- better external rotation with LTT
LDTT versus LTT
- 48 LDTT v 42 LTT
- superior ROM and functional outcome with LTT
- reduced progression to OA with LTT (7% v 31%)
Partial repair of rotator cuff
Theory
Repair subscapularis and infraspinatus
- restore balanced force couplet
- act in conjuction to depress humeral head
- allow deltoid to work
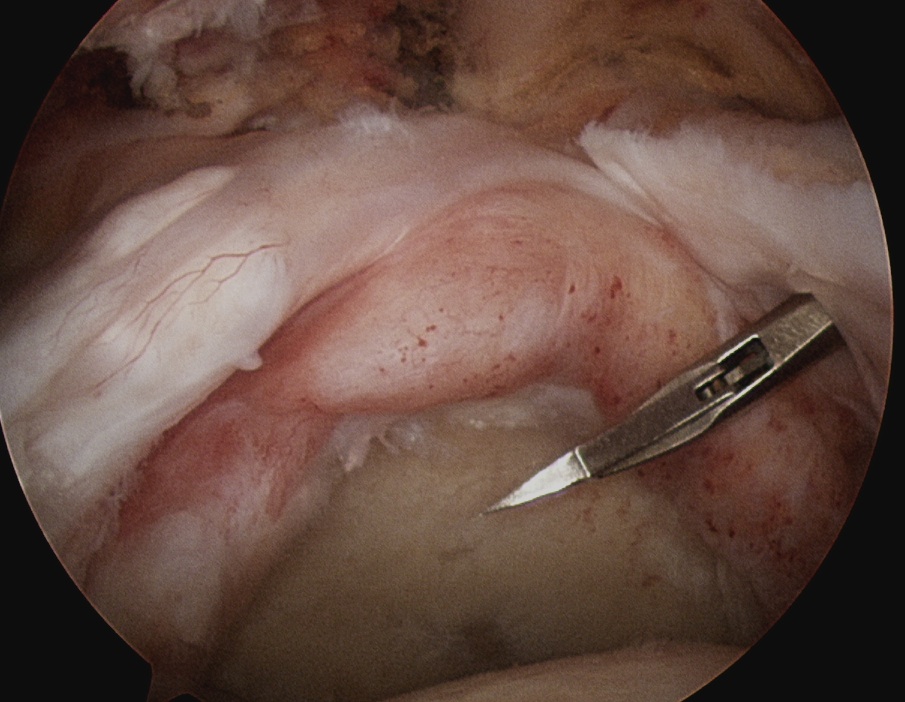
Technique
Vumedi arthroscopic repair of massive rotator cuff tear video
Subacromial arthroscopy
- leave coracoarcomial ligament intact to prevent humeral head escape
- subscapularis repair
- mobilize supraspinatus and infraspinatus above and below glenoid
- repair infraspinatus above equator
- repair supraspinatus as able
- typically leave area of humeral head exposed

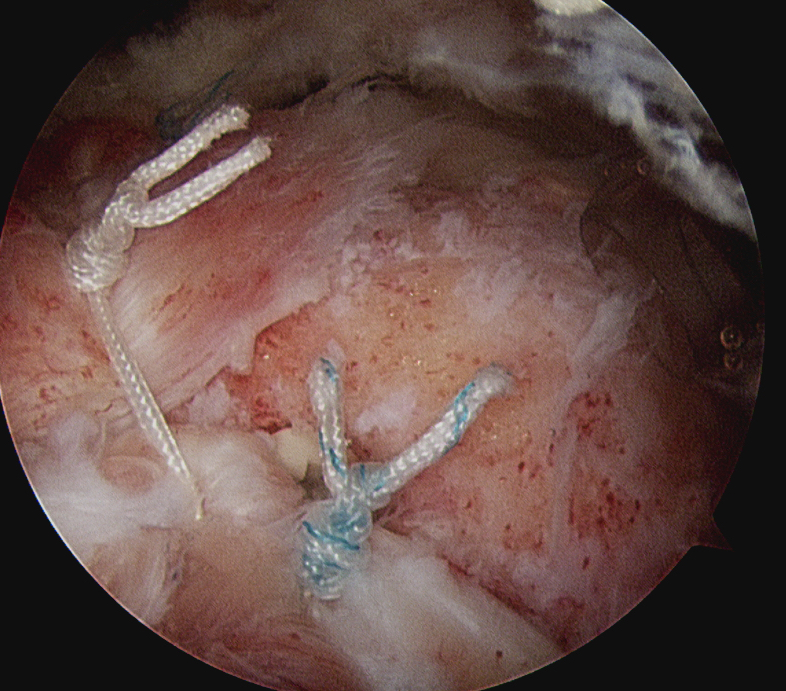
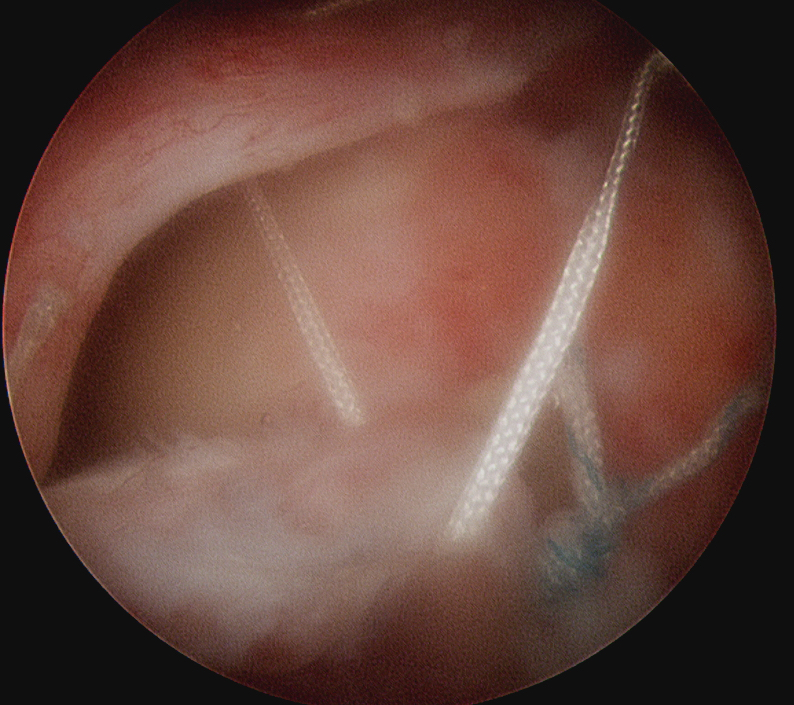
Margin convergence sutures
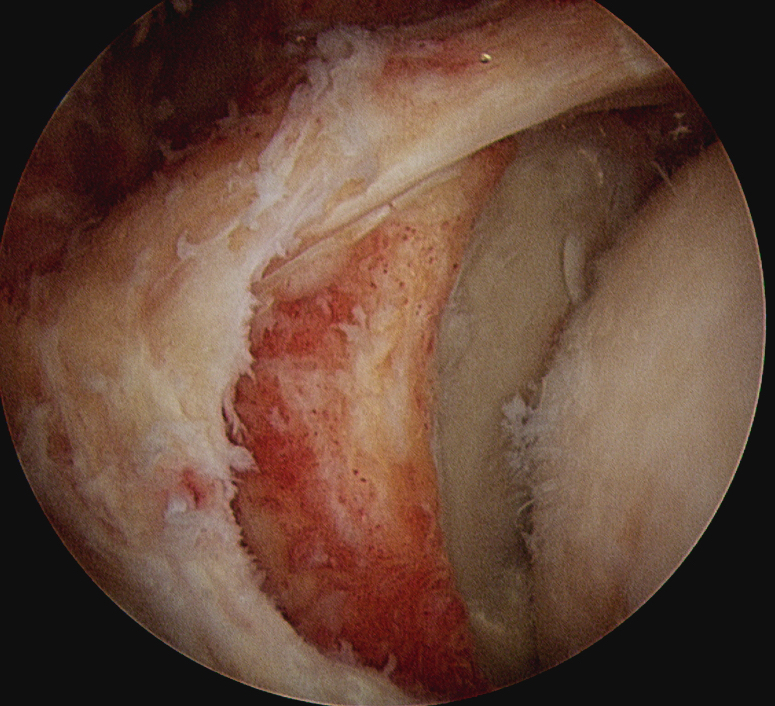
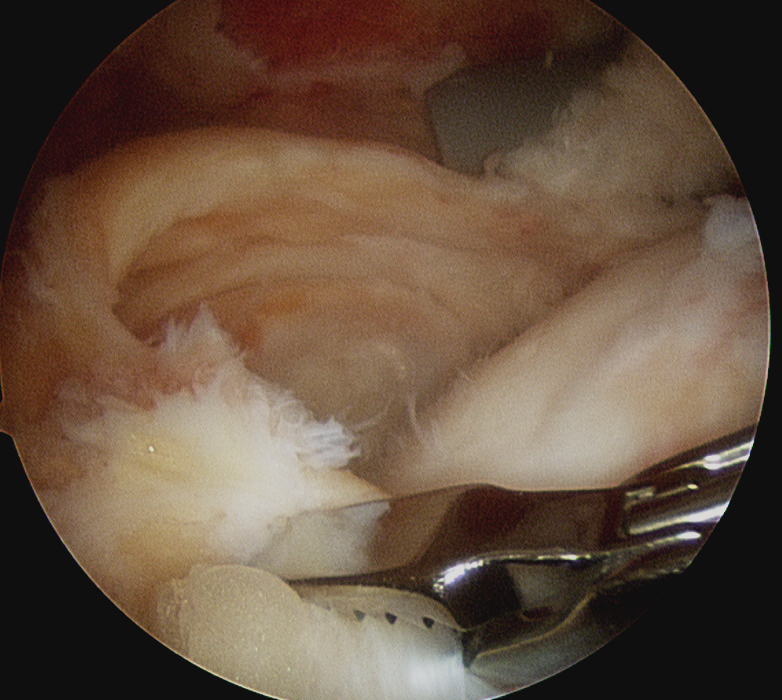
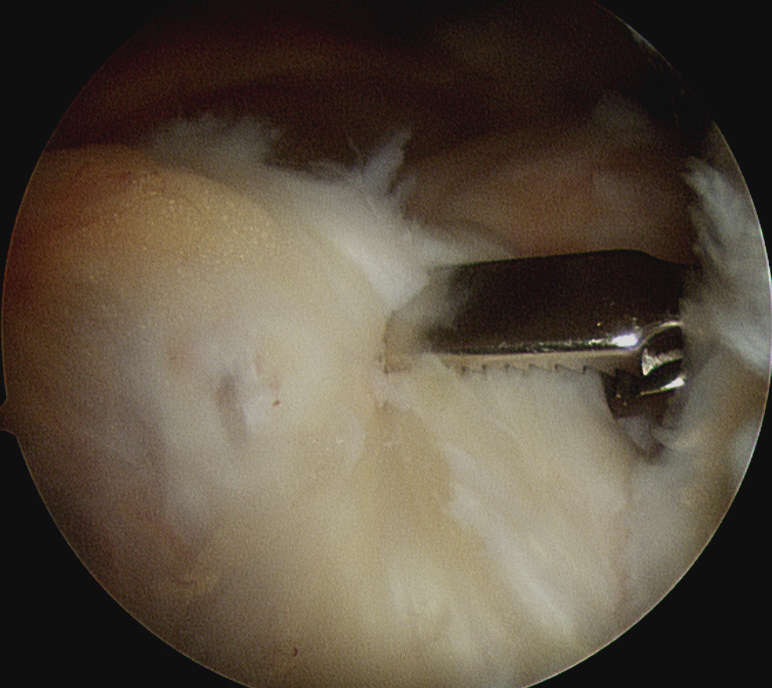
Release infraspinatus tendon posteriorly and assess mobility
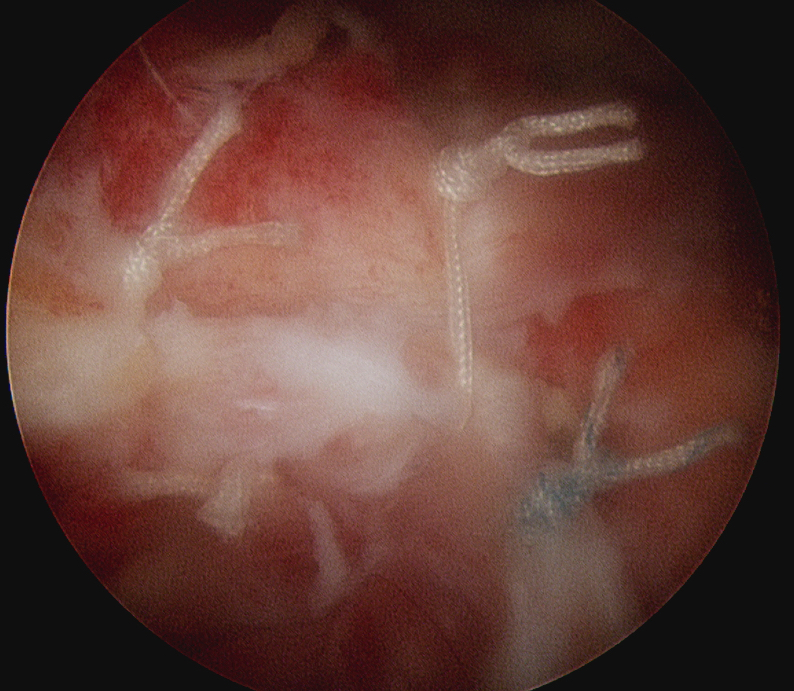
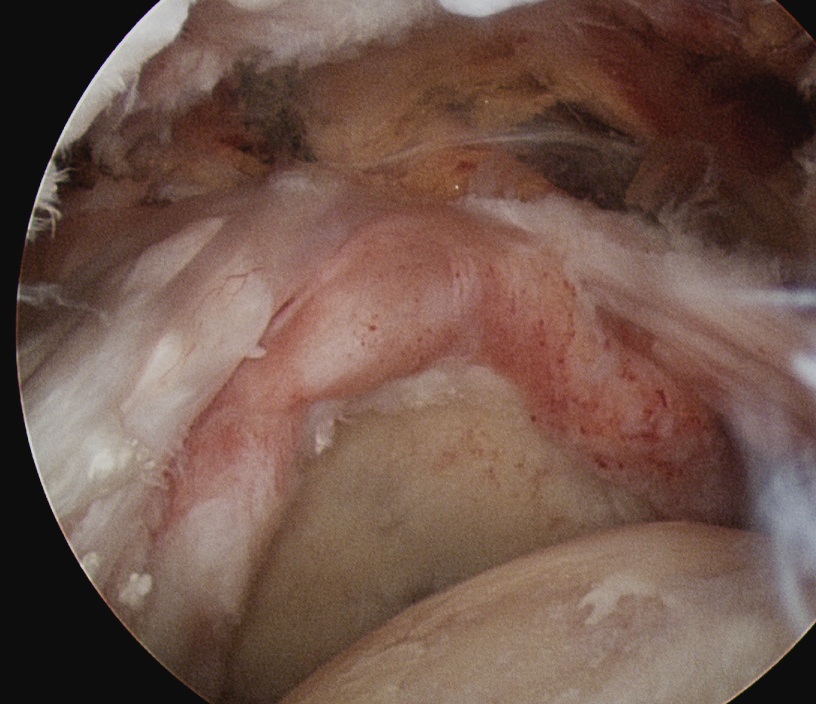
Repair infraspinatus with a combination of margin convergence and posterior suture anchors onto posterior greater tuberosity
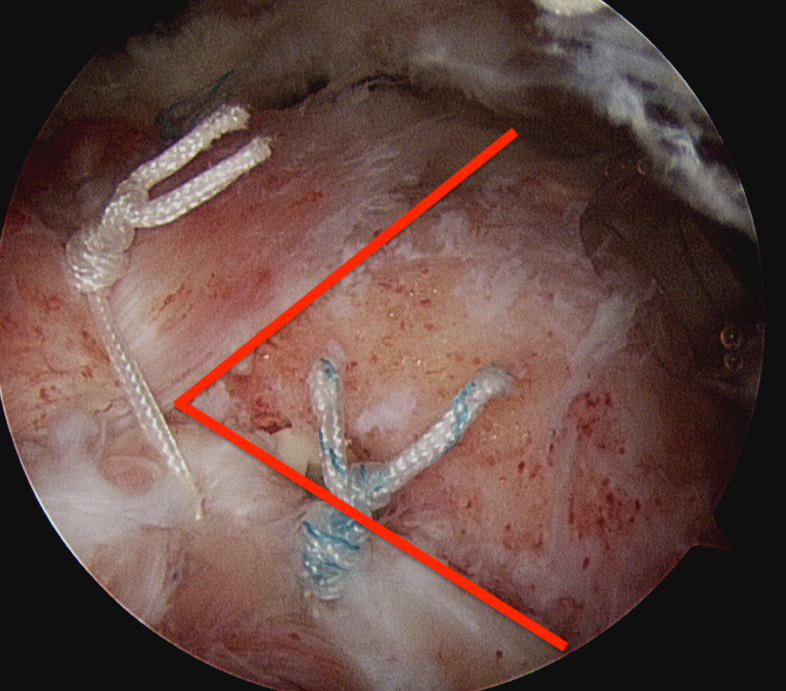
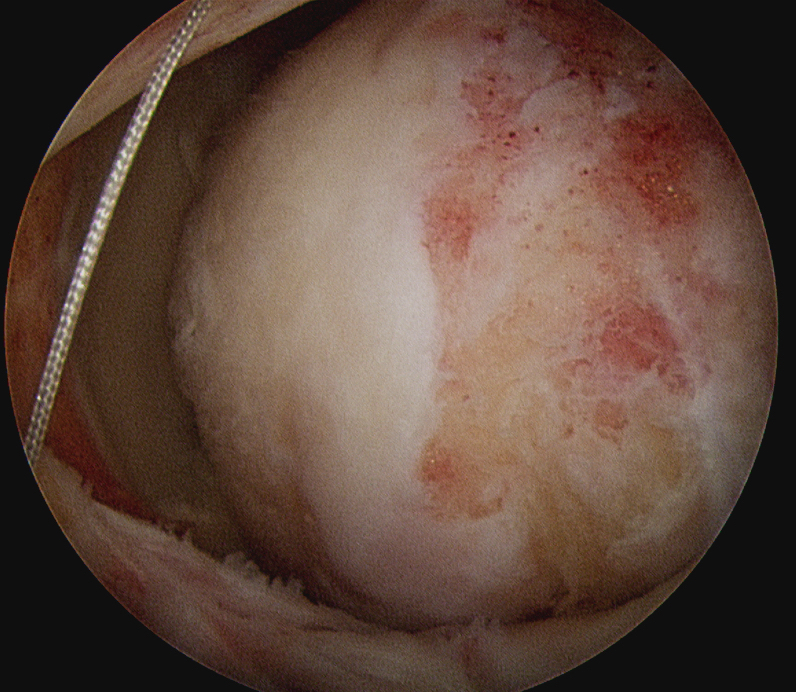
True partial repair of the rotator cuff with exposed triangle of greater tuberosity
Results
Latissimus Dorsi Tendon Transfer (LDTT)
Indications
Irreparable tear / retear / young patient with manual job
Contra-indications
Subscapularis deficiency
Technique
Vumedi LDTT arthroscopic assist video
Lateral decubitus position / beach chair
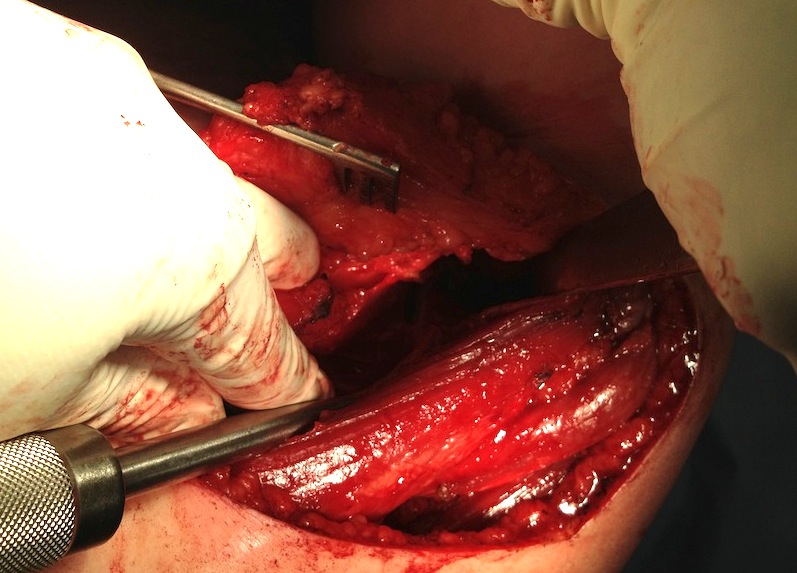
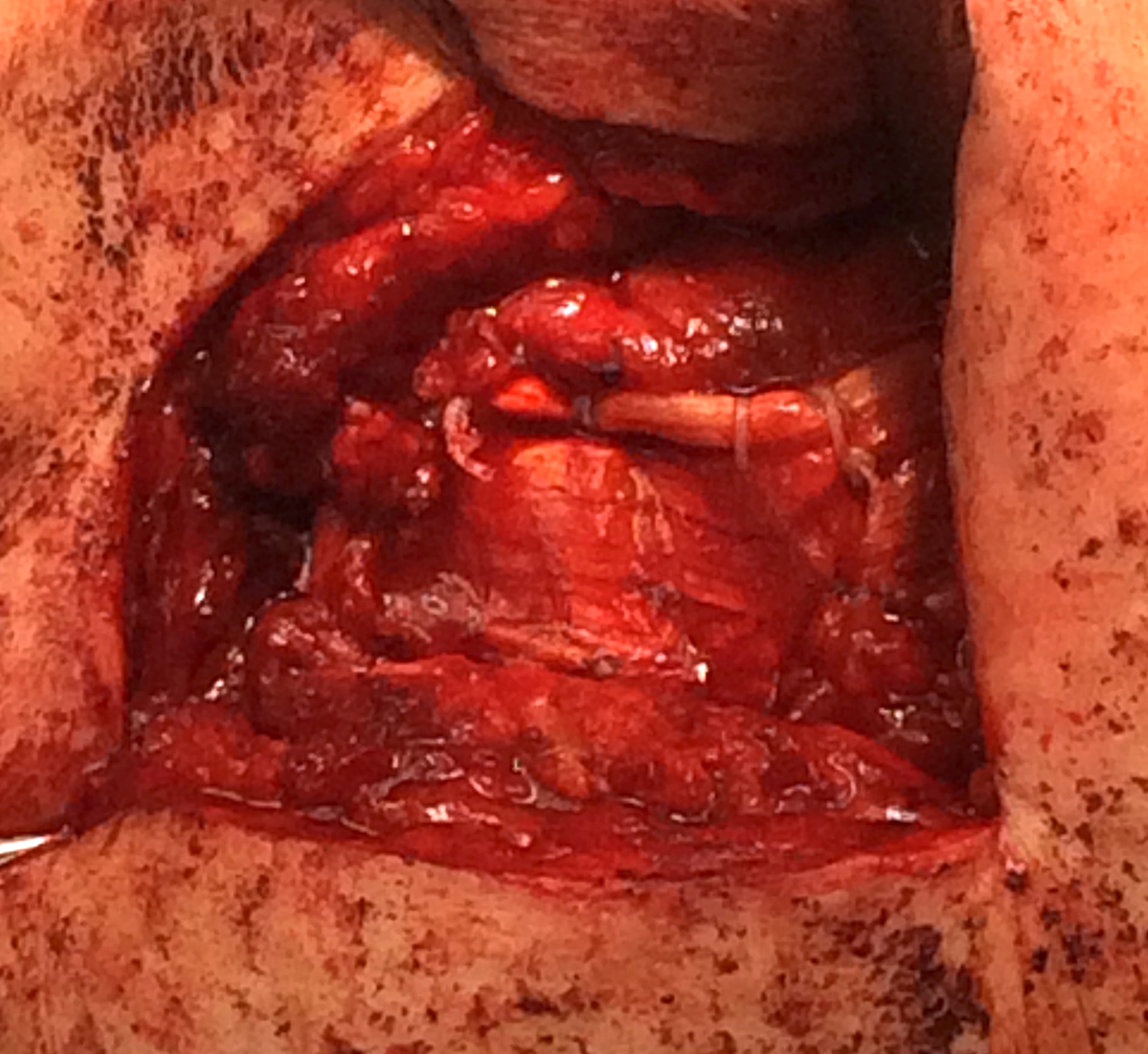
Harvest latissimus dorsi tendon
- arm forward flexed to 90 degrees and internally rotated
- L shaped incision
- inferior margin deltoid, lateral aspect of latissimus dorsi
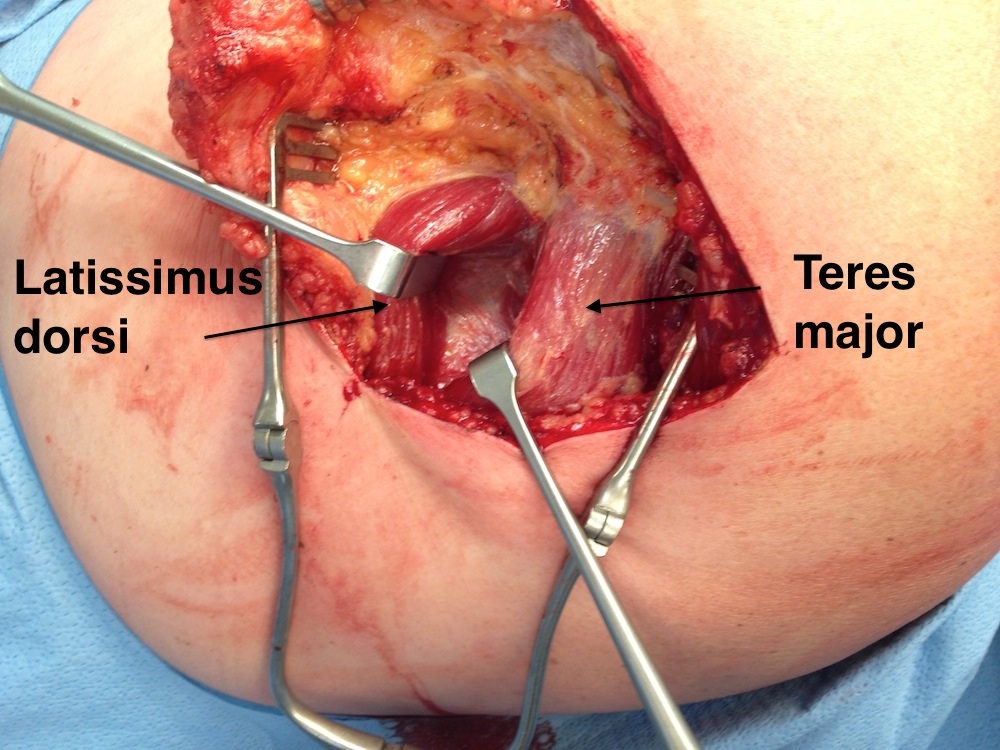
- find L dorsi muscle most lateral and release
- identify tendon insertion on humerus, can be confluent with T major tendon
- release tendon from insertion to maximize length, avoid injury to radial nerve
- suture each margin with strong suture, leave limbs long to pass tendon
- release muscle belly for length / above and below / must identify and preserve pedicle

Identify LDTT muscle belly most lateral and follow up onto humerus
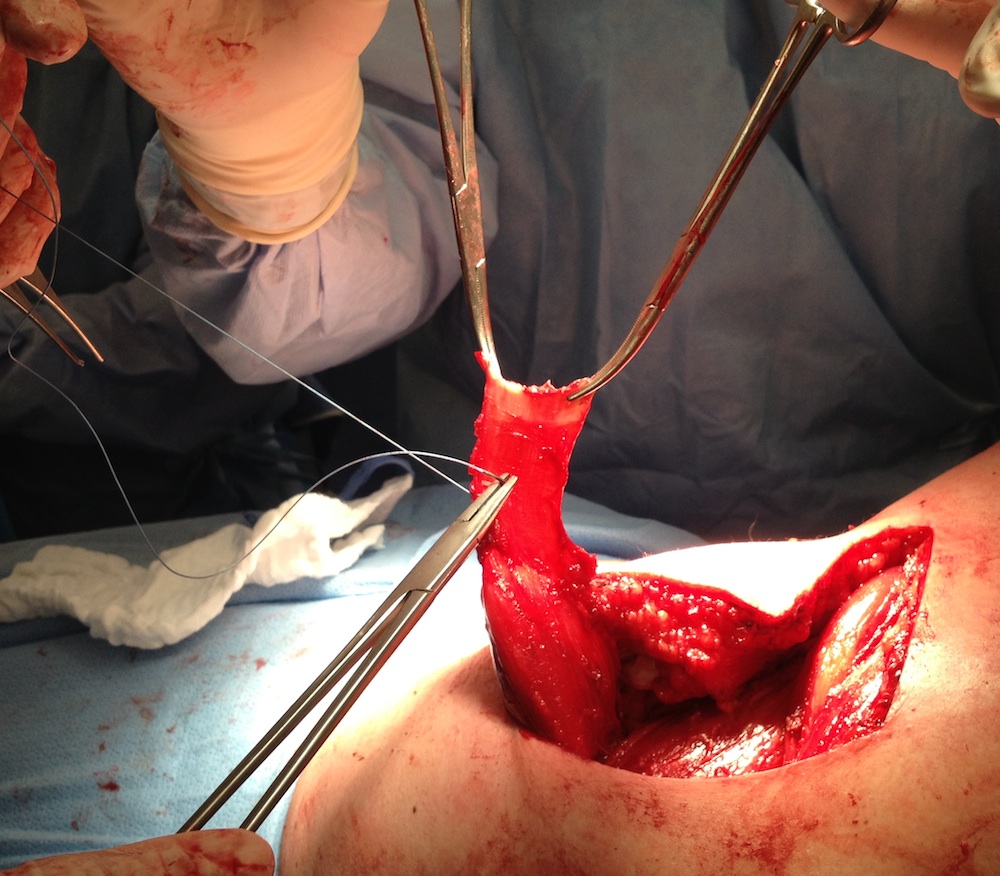
Follow tendon up onto the humeral insertion and release, suture tendon
Detach deltoid from lateral acromion +/- perform arthroscopically
- tunnel tendon under deltoid & acromion
- suture anchors repair to greater tuberosity +/- subscapularis
Put patient in external rotation brace for 6 weeks
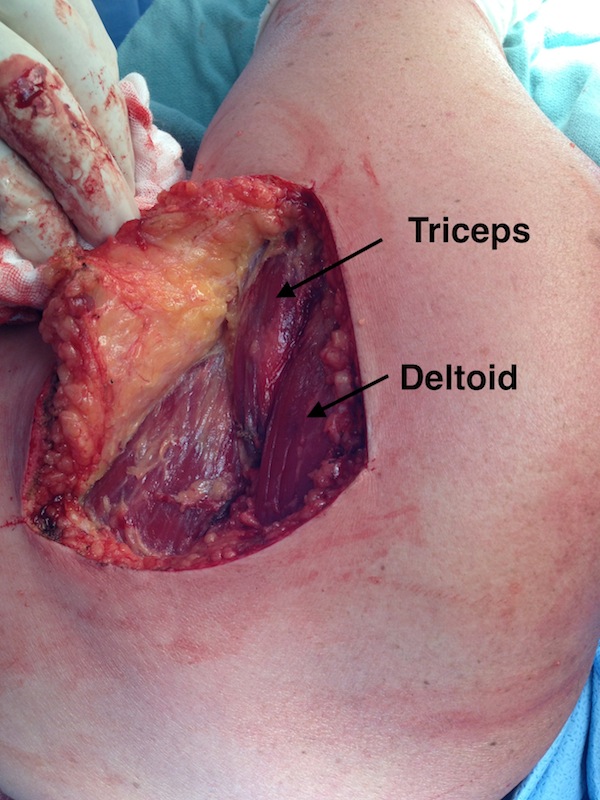
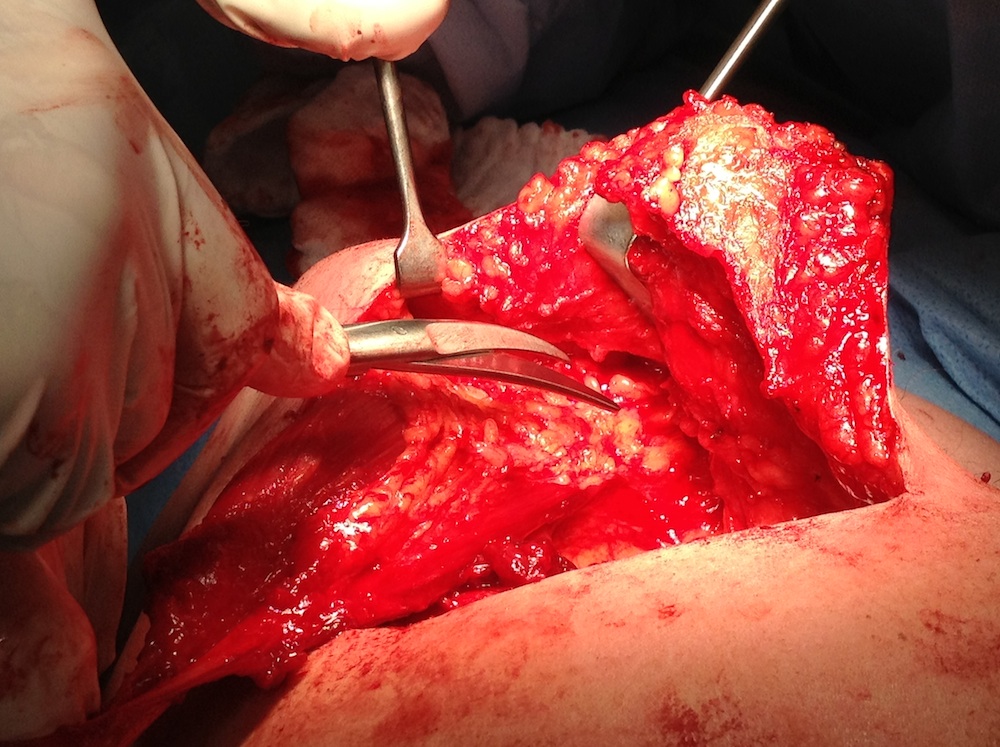
Identify posterior deltoid and tunnel tendon under posterior deltoid into subacromial space
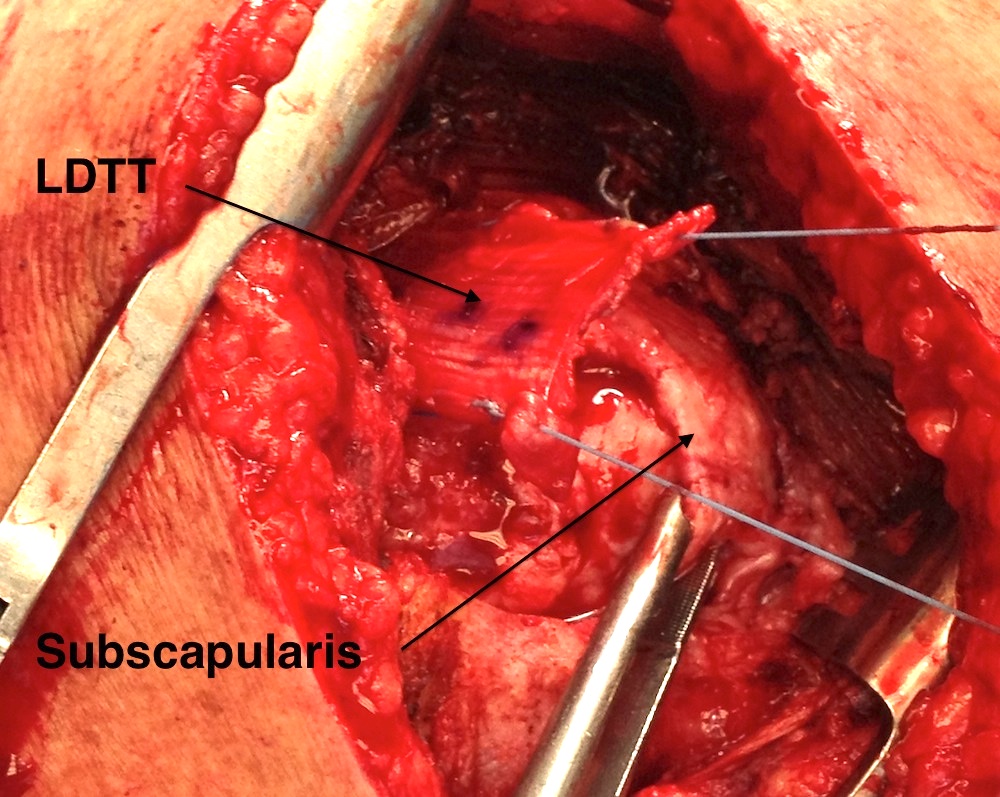
Repair with suture anchors to greater tuberosity and to subscapularis
Results
- systematic review of long term LDTT results in 400 patients
- evidence of improved outcomes
- complication rate 13%
- revision rate 6%
Lower trapezius transfer (LTT)
Issues
Advantage - line of pull in line with infraspinatus
Disadvantage - tendon very short and must be augmented with allograft / autograft
Technique
Vumedi lower trapezius tendon harvest video
Vumedi lower trapezius transfer video
Arthroscopy techniques LTT PDF

Shoulder arthroscopy
- clear subacromial space
- repair subscapularis / biceps tenodesis or tenotomy
- debride insertion onto greater tuberosity
Beachchair / lateral decubitus
- drape to expose entire scapula
- incision 2 cm below medial scapula spine
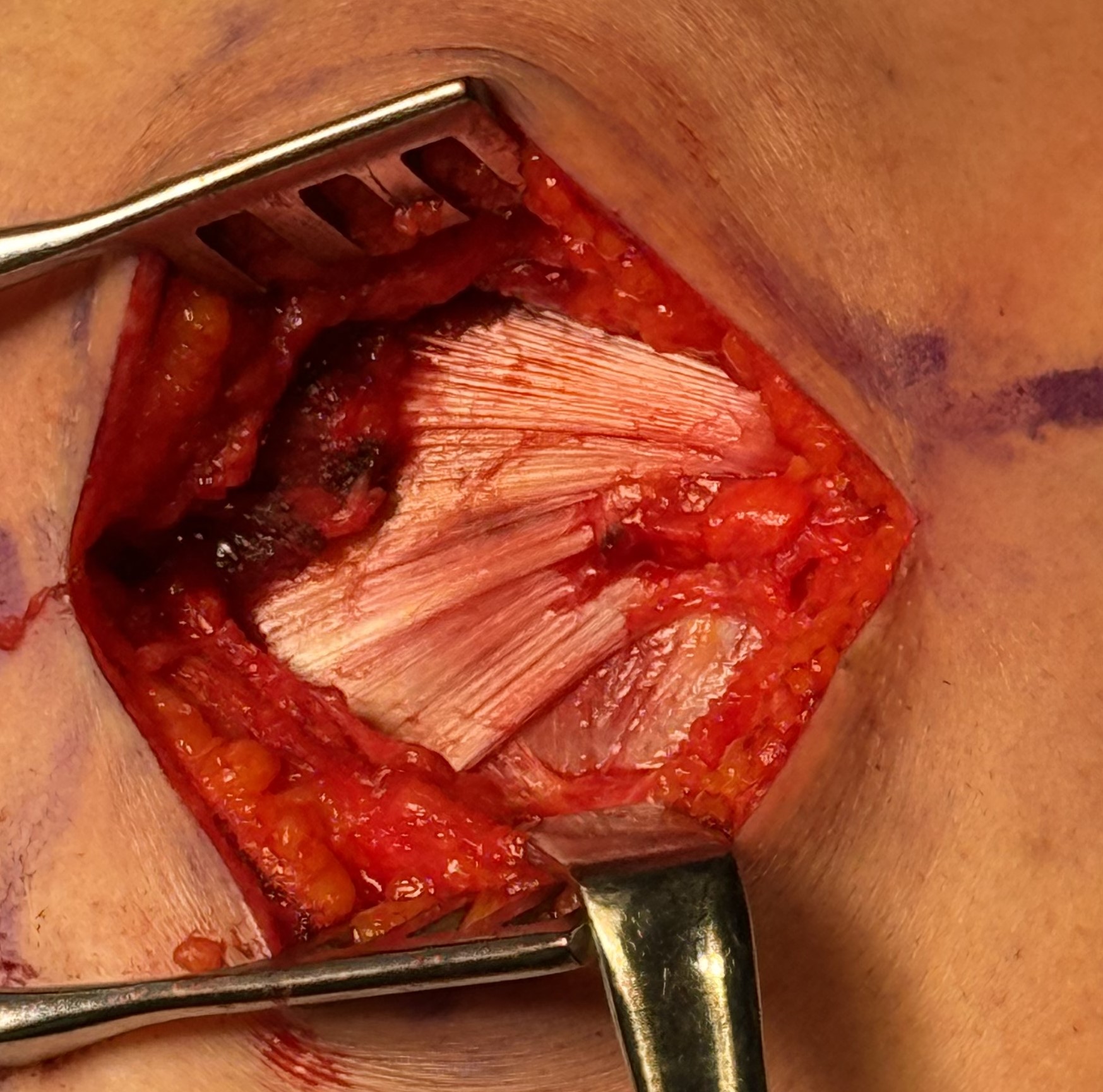
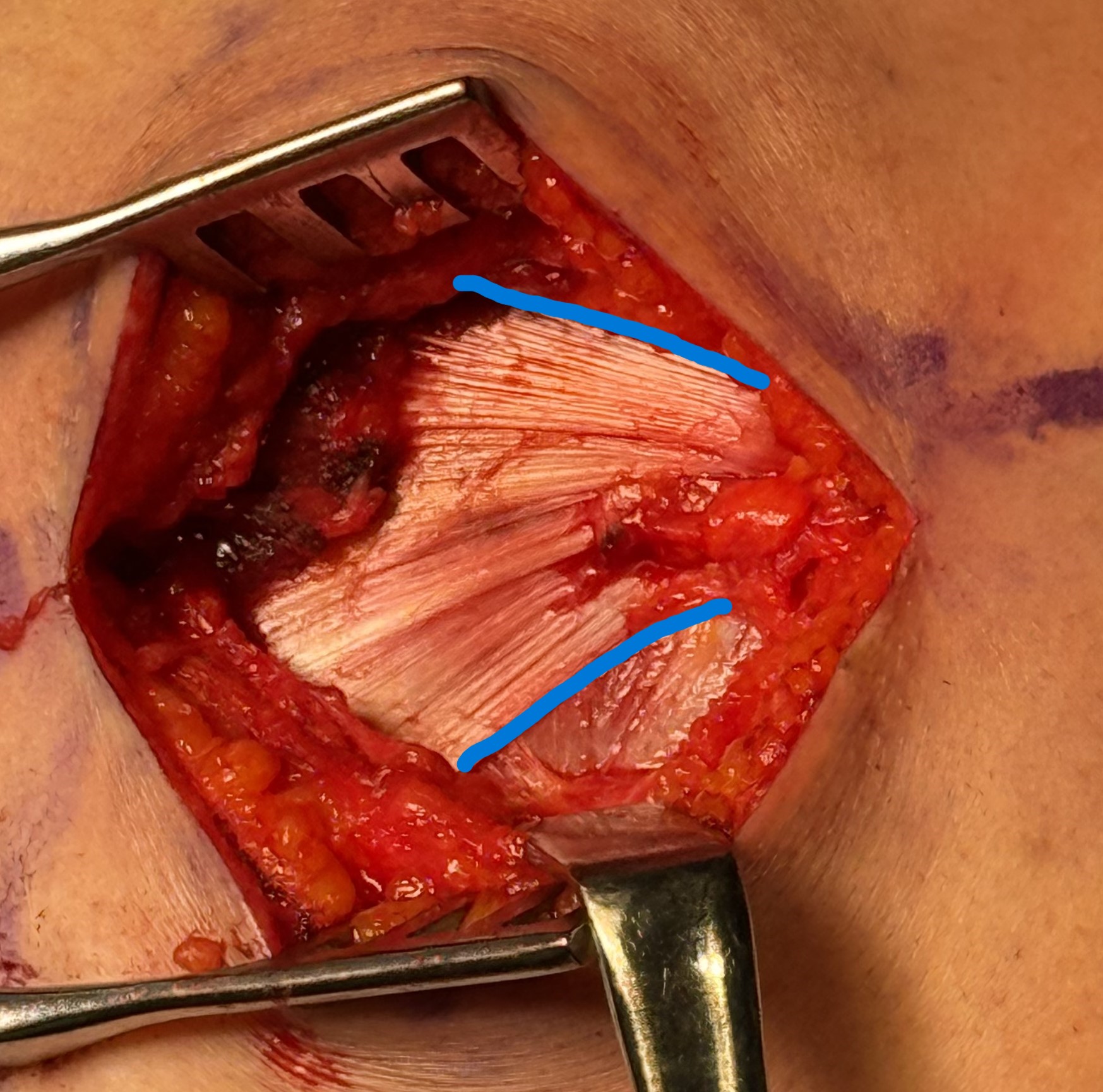
- identify lower trappezius tendon superficial to infraspinatus
- detach from insertion scapula spine and release tendon
- separate from middle trapezius
- spinal accessory nerve is deep to muscle and runs 2 cm medial to scapula
- reinforce tendon with running sutures
Tendoachilles allograft augmentation
- tendon is too short and needs to be 15 cm long
- need to augment with hamstring autograft / tendoachilles allograft
Create subcutaneous tunnel to subacromial space
- develop interval between infraspinatus and posterior deltoid
- pass allograft into subacromial space and double row repair to greater tuberosity
- repair open v arthroscopic
Pulvertaft weave allograft to lower trapezius
- arm in 30 degrees of abduction and external rotation
Results
De Marinis et al Arthroscopy 2024
- systematic review of 7 studies and 160 patients
- increased ROM: flexion 10 degrees, external rotation 11 degrees
- complication rate 18% with seroma / hematoma most common
- reoperation rate 8%
- revision to rTSA 5%
Superior capsular reconstruction
Concept
Static stabilizer
- between glenoid and greater tuberosity of humerus
- restrict superior migration of humeral head
Technique
Grafts
- fascia lata autograft
- acellular dermal allograft
Subacromial arthroscopy
- prepare superior surface of glenoid and greater tuberosity
- measure defect size with arm in 30 degrees abduction and 15 degrees external rotation
- place 2 - 3 anchors in glenoid (consider Neviaser portal)
- place 2 medial row anchors in greater tuberosity
- pass all sutures through graft outside of shoulder
- suture shuttle into shoulder and tie knots
- lateral row fixation on glenoid
- can tie to infraspinatus posteriorly
- don't tie to subsubscapularis anteriorly as can restrict ROM
Results
- systematic review of SCR 7 studies and 350 patients
- graft retear 13%
- satisfaction rates 73 - 90%
- systematic review of SCR 17 studies and 519 patients
- no difference in functional outcome between allograft and autograft
- retear rate: autograft 27%, allograft 21%
Subacromial spacer
Concept
Stryker InSpace Subacromial Spacer
- biodegradable balloon filled with saline
- remains inflated for 3 - 4 months
- degrades over 12 months
- recenters humeral head in glenohumeral joint

Technique
Stryker InSpace surgical technique PDF
Vumedi subacromial spacer video
Results
- double blind RCT of 117 patients
- START:REACTS trial
- spacer v arthroscopic debridement and biceps tenotomy
- at 12 months outcomes favored debridement only group
- study stopped
- 2 year follow up of 100 patients in START:REACTS trial
- outcomes still favored debridement group
- multicentered RCT of 184 patients
- spacer v partial repair
- no difference in outcome
- better forward flexion with spacer