Definition
Failure of fusion of secondary ossification centers
Epidemiology
Incidence 3 - 8%
Bilateral in 60%
Anatomy
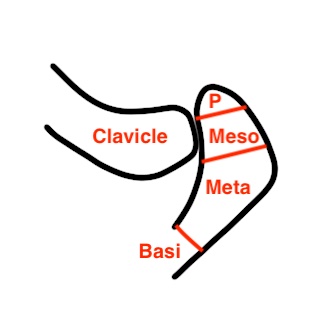
4 ossification centers present in acromion
- pre-acromion
- meso-acromion
- meta-acromion
- basia-cromion
The basiacromion fuses to spine of scapula by 12
Pre / Meso / Meta appear by 18
- unite by age 22 - 25
- if un-united by age 25 = Os Acromiale
Types
1. Meso-Acromion
- most common (94%)
- level with posterior aspect clavicle
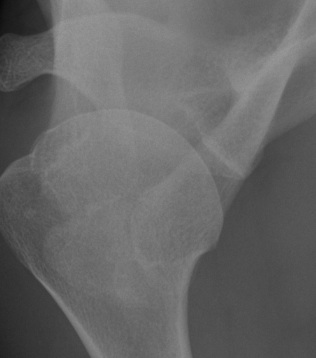
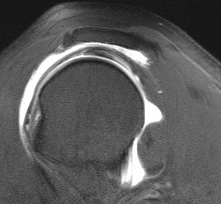
Axillary lateral
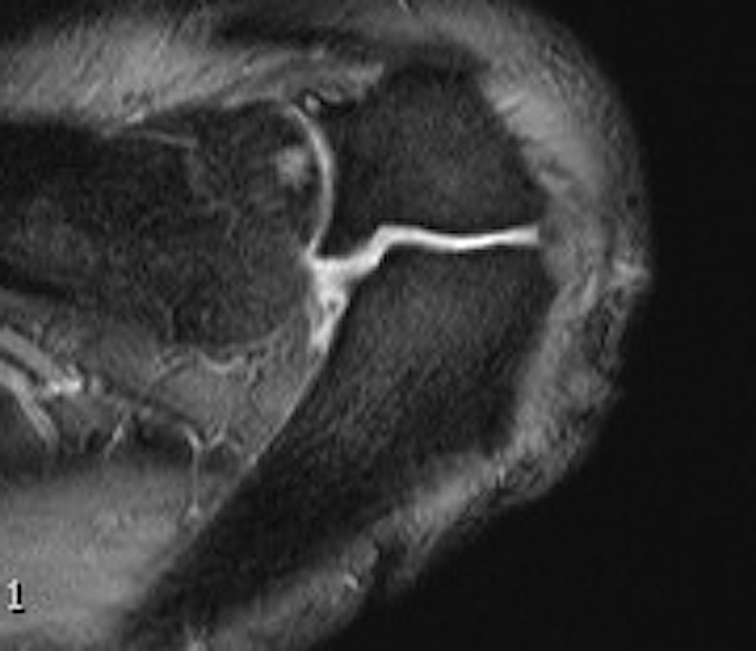
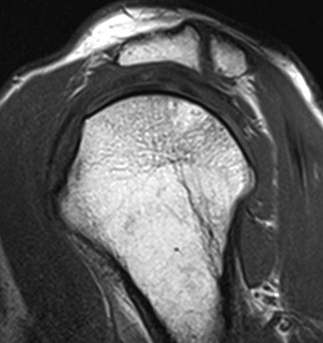
Axial MRI Sagittal MRI
2. Pre-acromion
Uncommon - level with anterior border acromion
3. Meta-Acromion
Rare
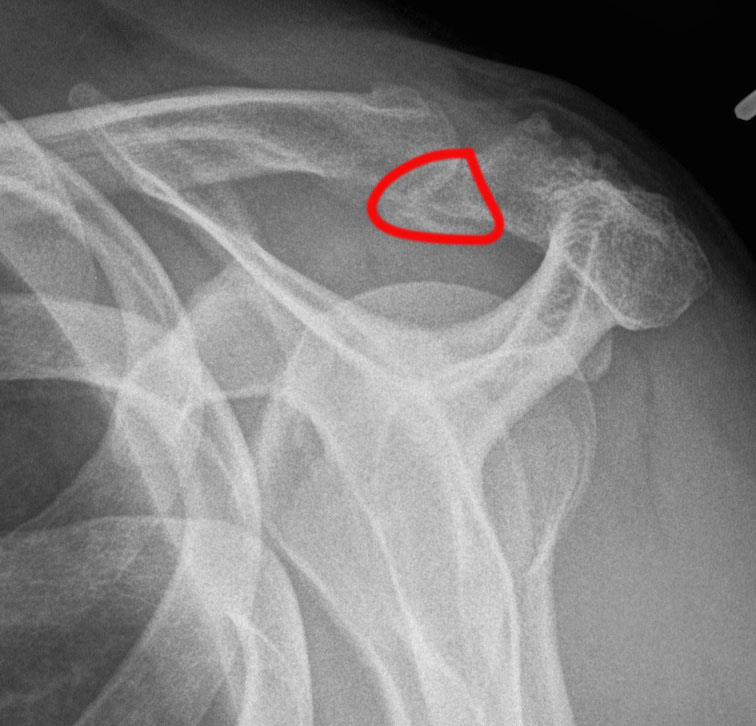
X-ray
Best seen on axillary lateral
Factors favoring diagnosis of os acromiale over fracture
- bilateral occurrence (xray other side)
- rounded borders with uniform space


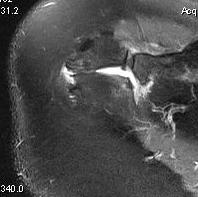
MRI
Useful investigation - may show edema if problematic / mobile / causing pain
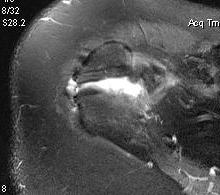
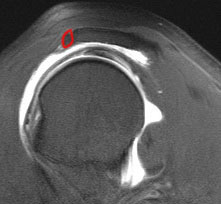
Axial MRI with meso-acromiale
Bone scan
Can be useful
- unlikely to be symptomatic if cold
- may be symptomatic if hot
Symptoms
Pain
- inflammation at nonunion site (inflammation on MRI)
- fragment moves with deltoid contraction and causes impingement symptoms


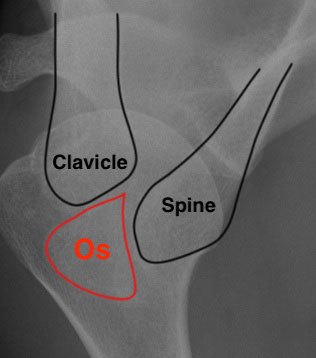
Axillary lateral showing meso-acromion Scapula lateral xray showing os acromiale
Management
Indications
Failure of non operative treatment
Symptomatic os acromiale
Options
1. Excision
2. ORIF
Purnell et al. J Orthop Surg Res 2019
- systematic review of prospective and retrospective cases
- excision: 92% good or excellent results
- ORIF: 82% good or excellent results, 67% complication rate (non union, infection, seroma, removal hardware)
- acromioplasty: 67% good or excellent results
1. Excision
Indications
Pre-acromion or meso-acromion
Options
Open - risk compromising deltoid insertion
Arthroscopic - leaves deltoid attach intact
Results
- arthroscopic excision in 11 shoulders of athletes
- all returned to sport at 14 weeks
- no loss of strength detected
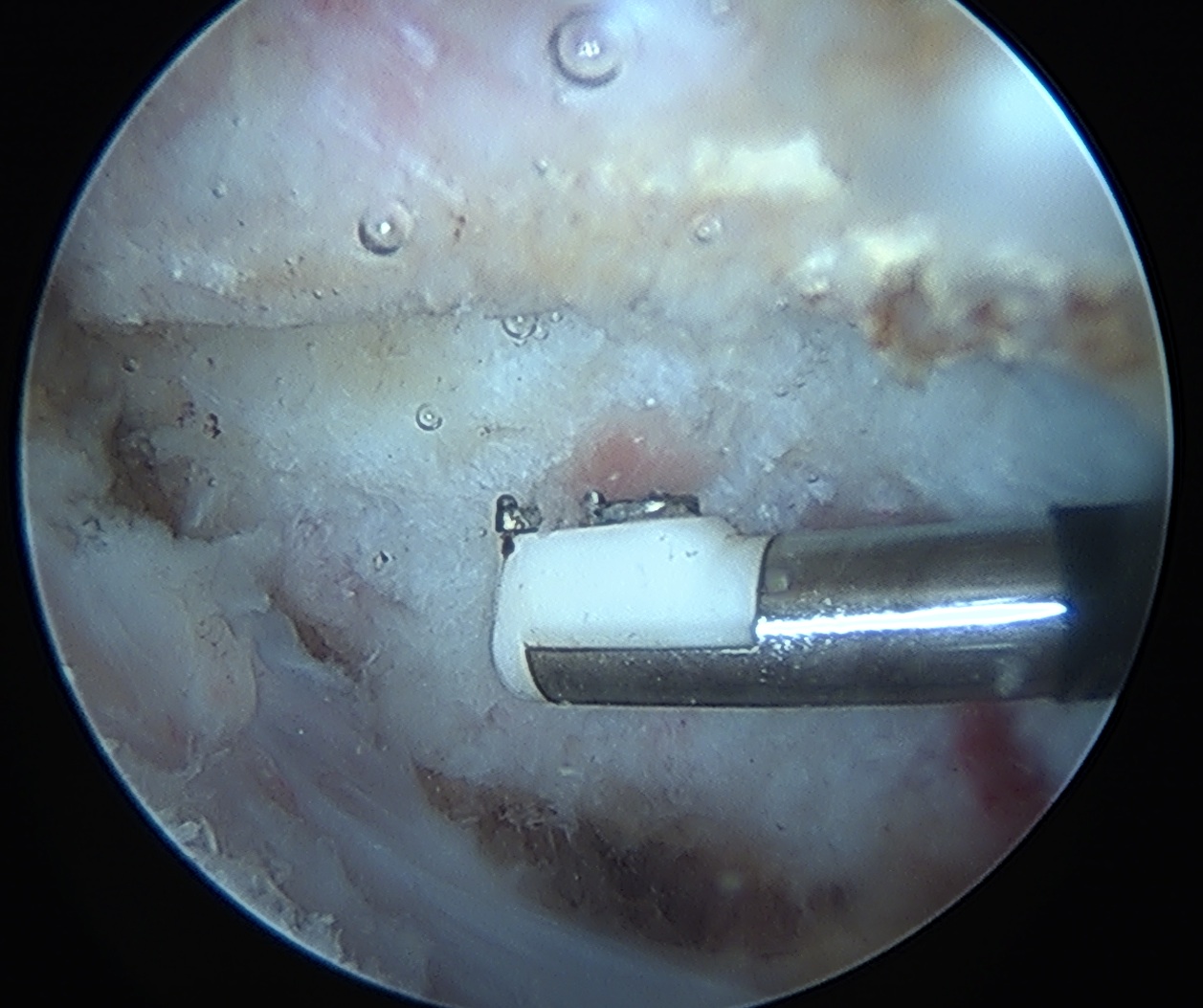
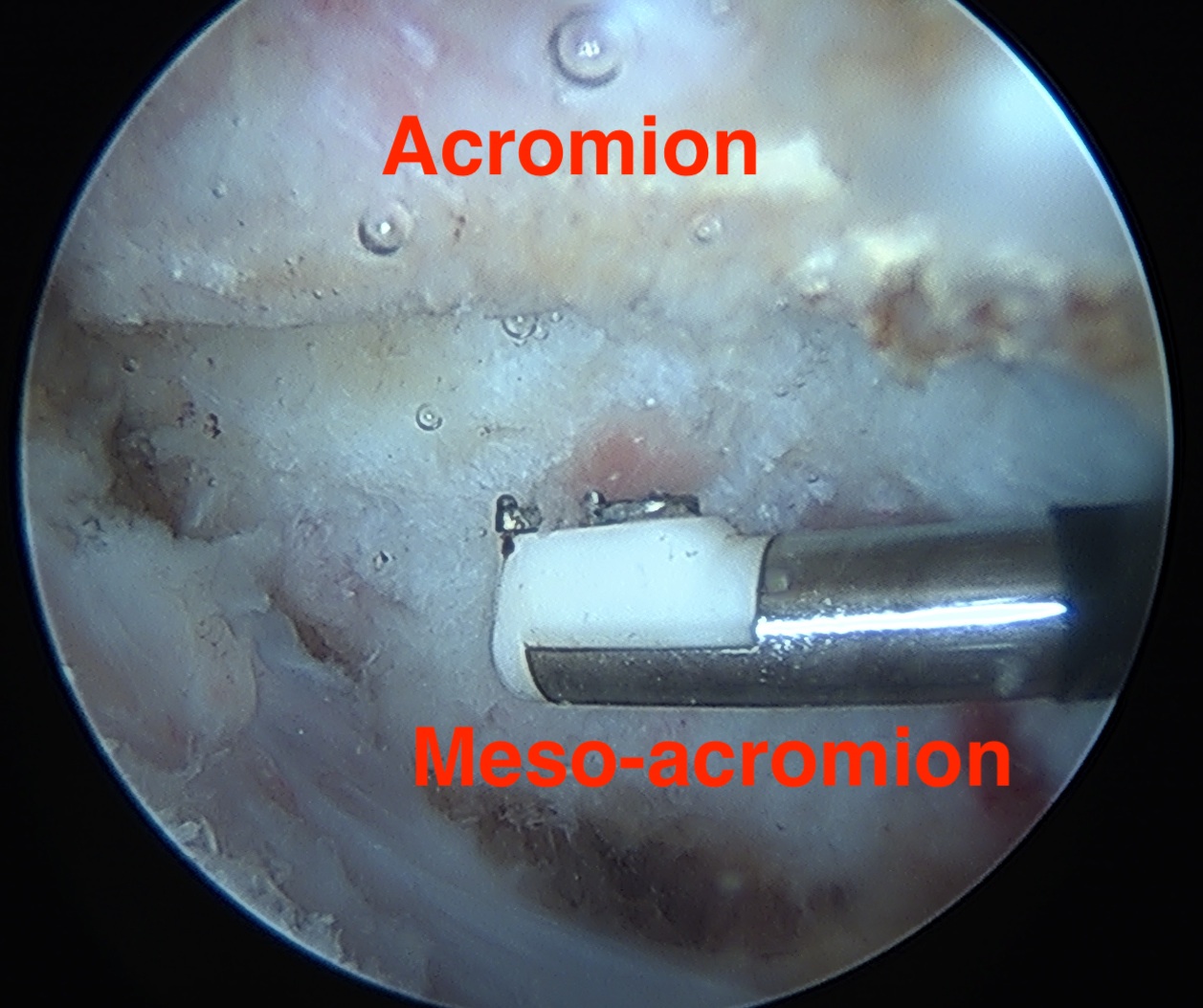
Vumedi video arthroscopic excision of os acromiale
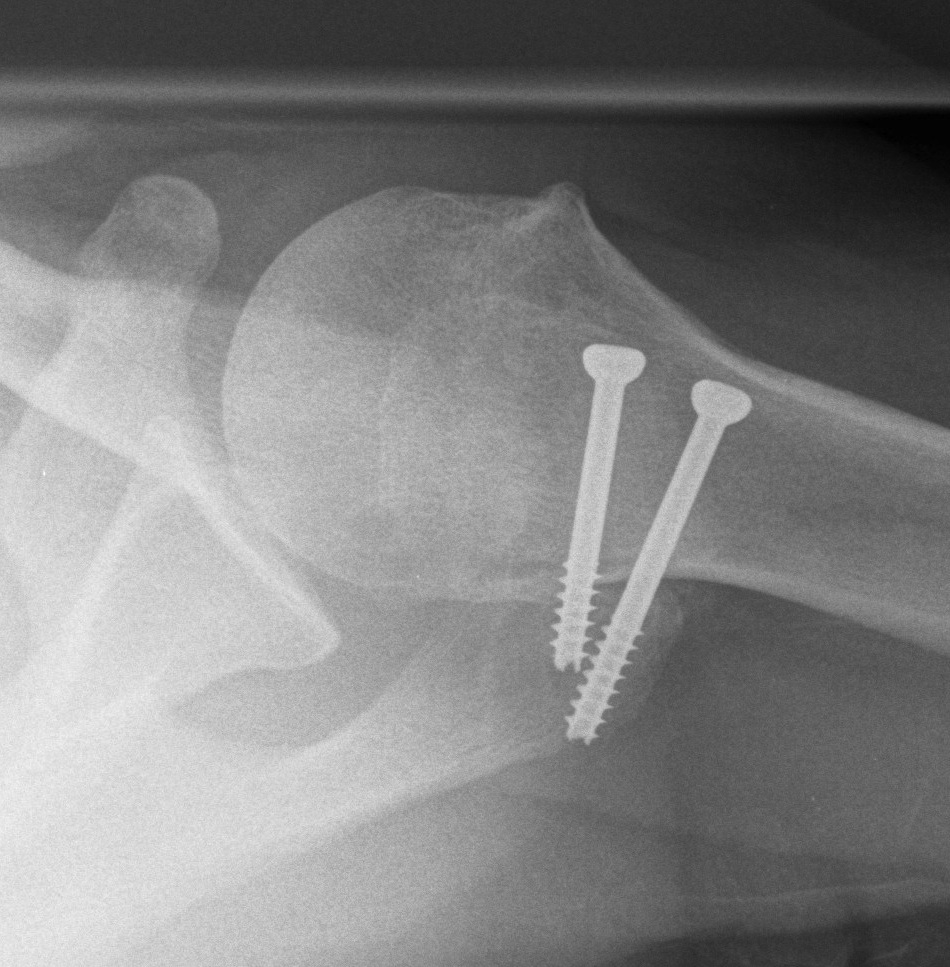
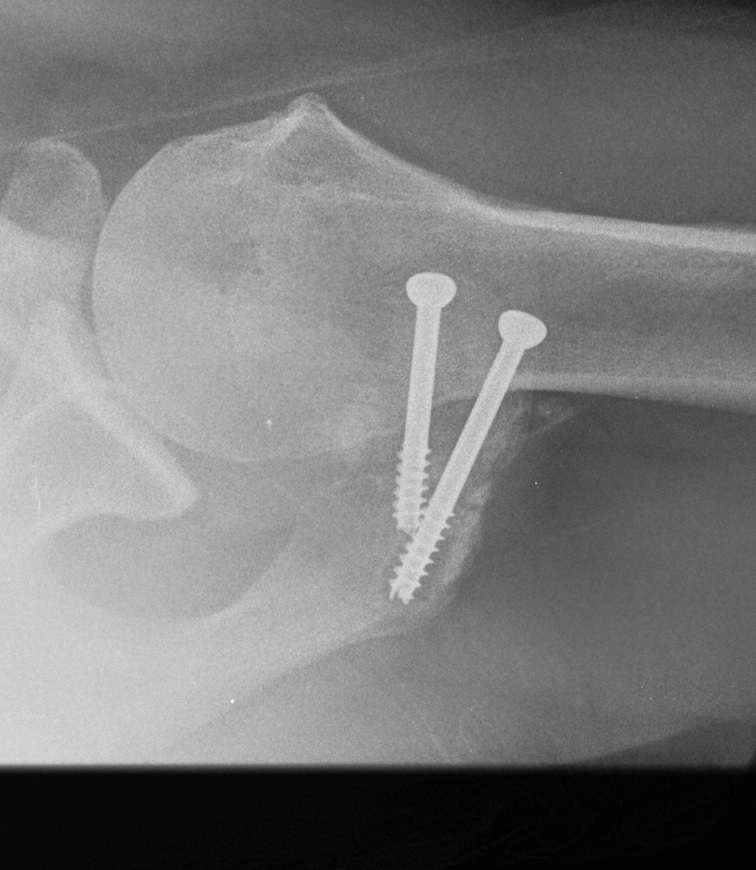
2. ORIF
Indications
Large fragment / mesoacromion
- take down non union
- bone graft / 2 x AP 3.5 mm screws / TBW
- especial care with deltoid reattachment
Vumedi video os acromiale fixation
Outcomes
Atinga et al J Should Elbow 2018
- 32 cases treated with screw fixation and bone graft
- 100% union at 3 months
- 1 infection, 1 seroma, 4 removal of metal work
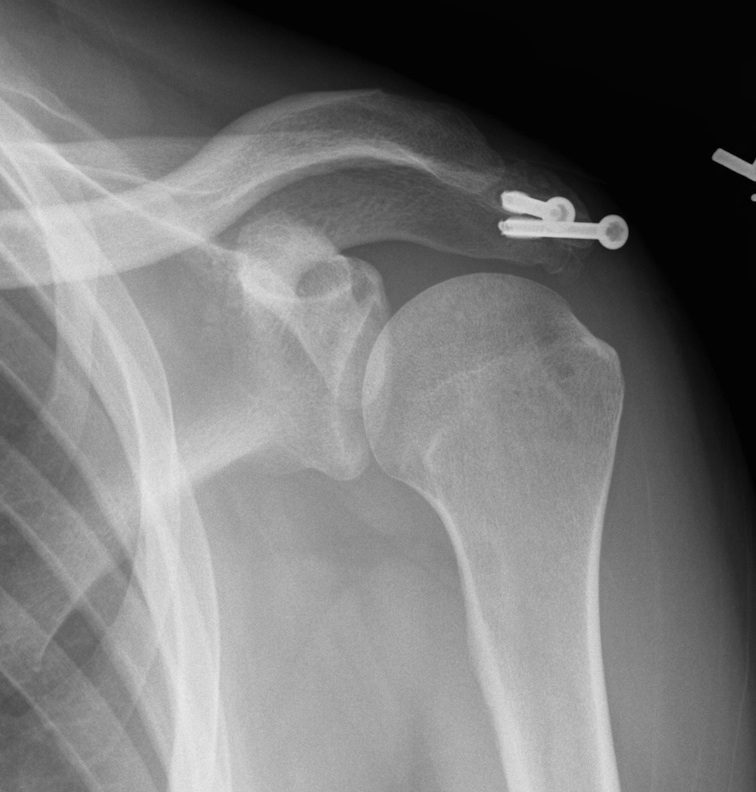
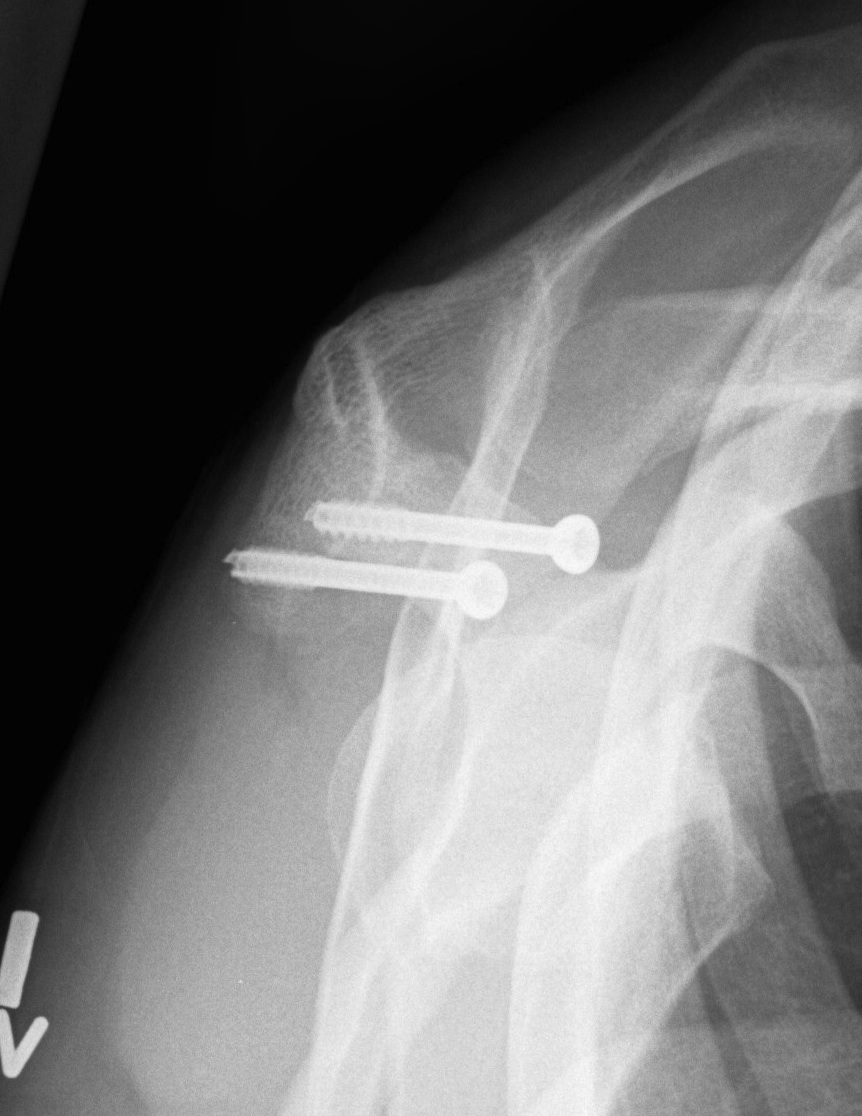
Risks
Nonunion
- remove screws
- arthroscopic resection


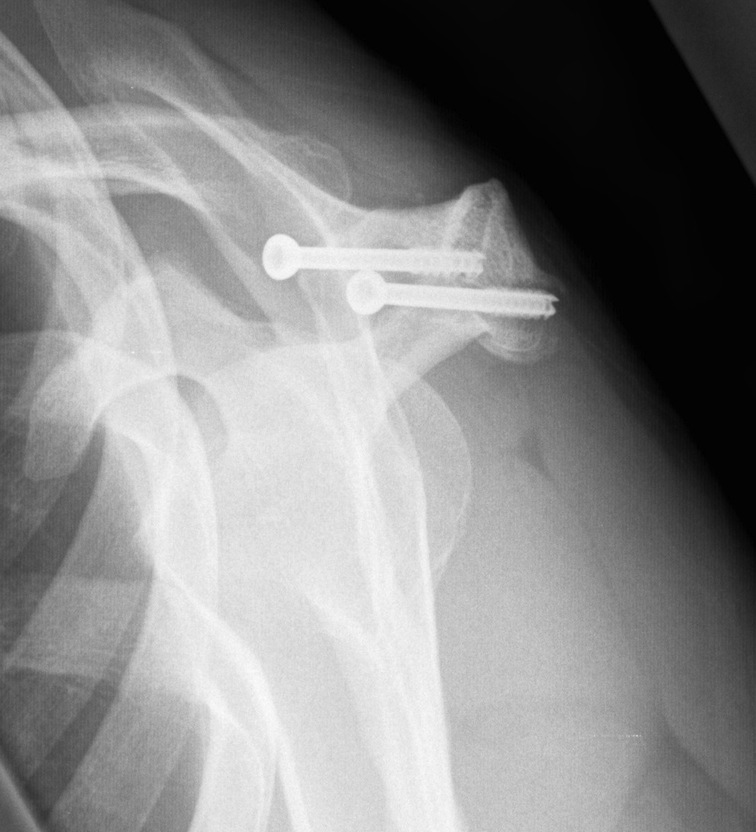
Non union with evidence of lysis around screws