Etiology
Post-traumatic
Idiopathic
Patterns
1. Osteoarthritis with osteophytes


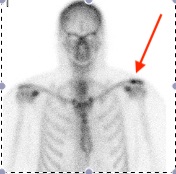
Osteolysis
Area of distal clavicle resorption
- due to repetitive microtrauma
- typically weight lifters or manual workers


Symptoms
Anterosuperior shoulder pain
- difficulty sleeping on affected side
Localised to ACJ
Signs

Visible deformity / swelling / osteophytes
Tenderness to direct palpation
- must compare to ensure other side is not tender
- may have bilateral ACJ OA)
Cross body adduction stress test

Chronopoulos et al. JBJS Am 2004
- 35 patients with isolated ACJ lesions
- cross body adduction stress test sensitivity of 77%
Diagnosis
Local anesthetic + Cortisone
- inject into joint
- diagnostic / therapeutic
Differential diagnosis
Intrinsic
- shoulder impingement / rotator cuff tear / calcific tendonitis
Extrinsic
- cervical root C4/5
- shoulder tip pain from abdominal pathology
Xray
Zanca view - AP 10° cephalic tilt with 50% penetration

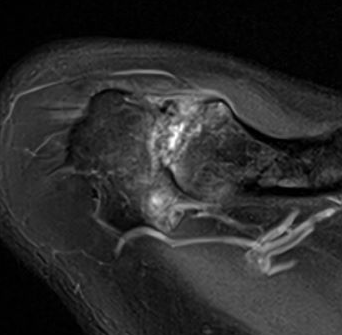
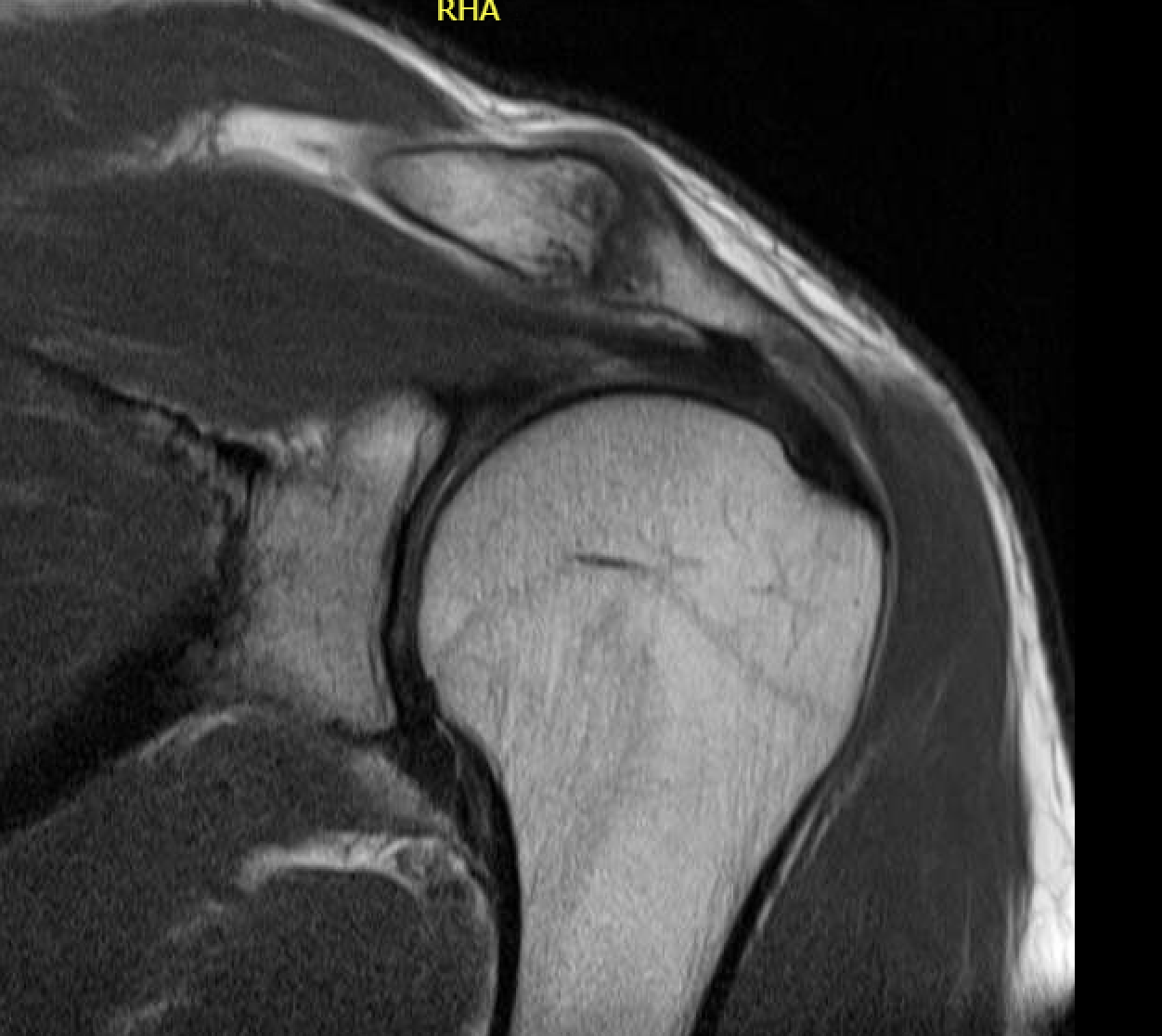
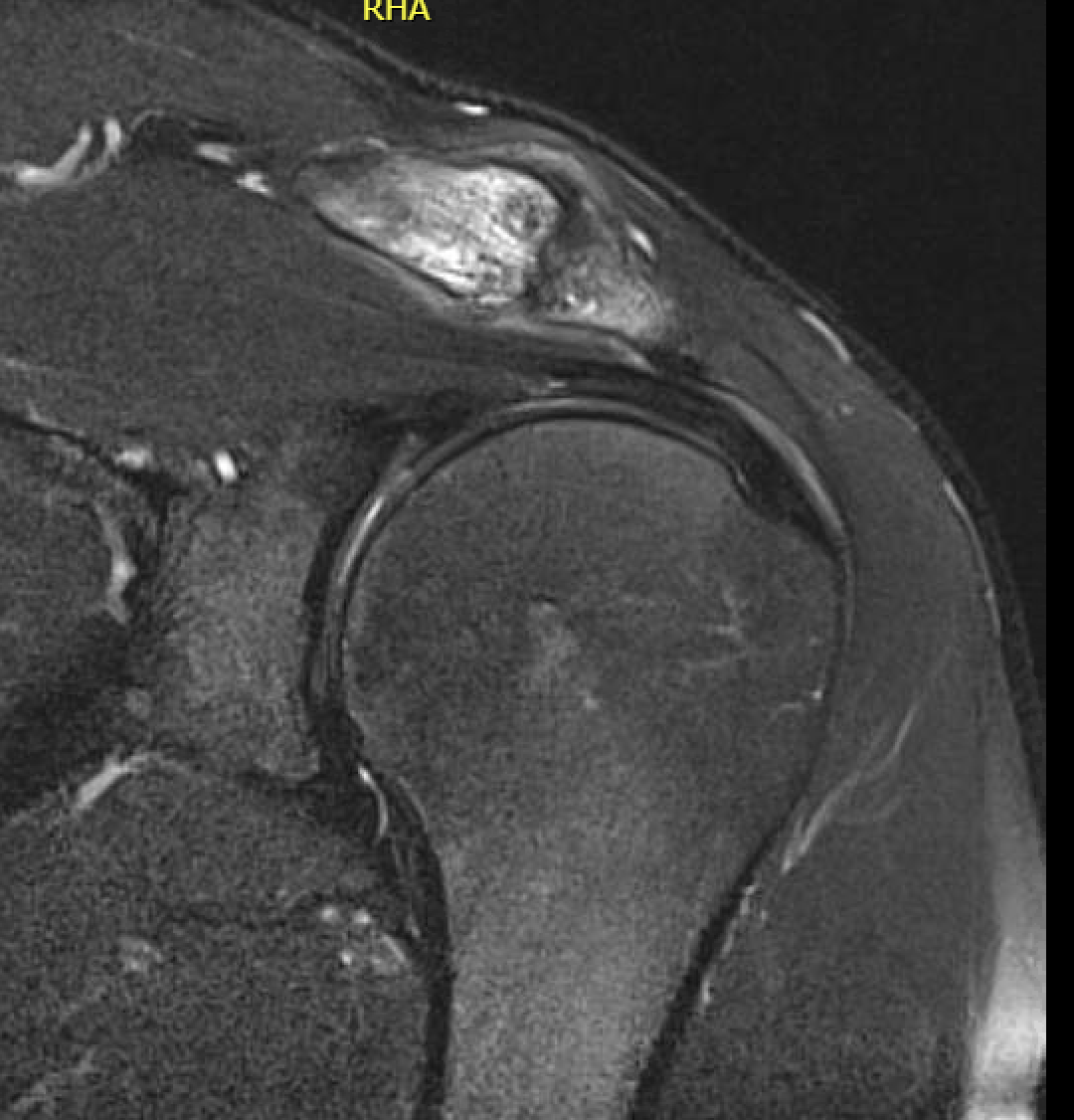
MRI
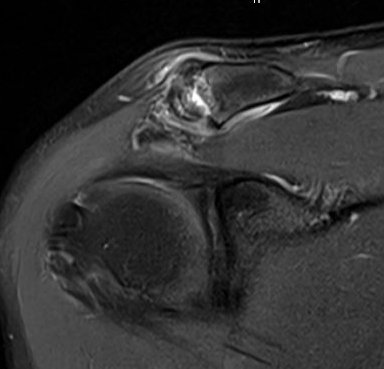
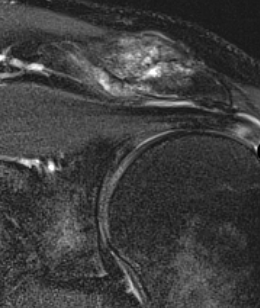
Acromioclavicular osteoarthritis
Stein et al. J Should Elbow Surg 2001
Grade I: Normal
Grade II: Capsular distension, bone marrow edema, mild joint narrowing
Grade III: Capsular distension, joint space narrowing, marginal osteophytes
Grade IV: Markedly abnormal ACJ with large osteophytes
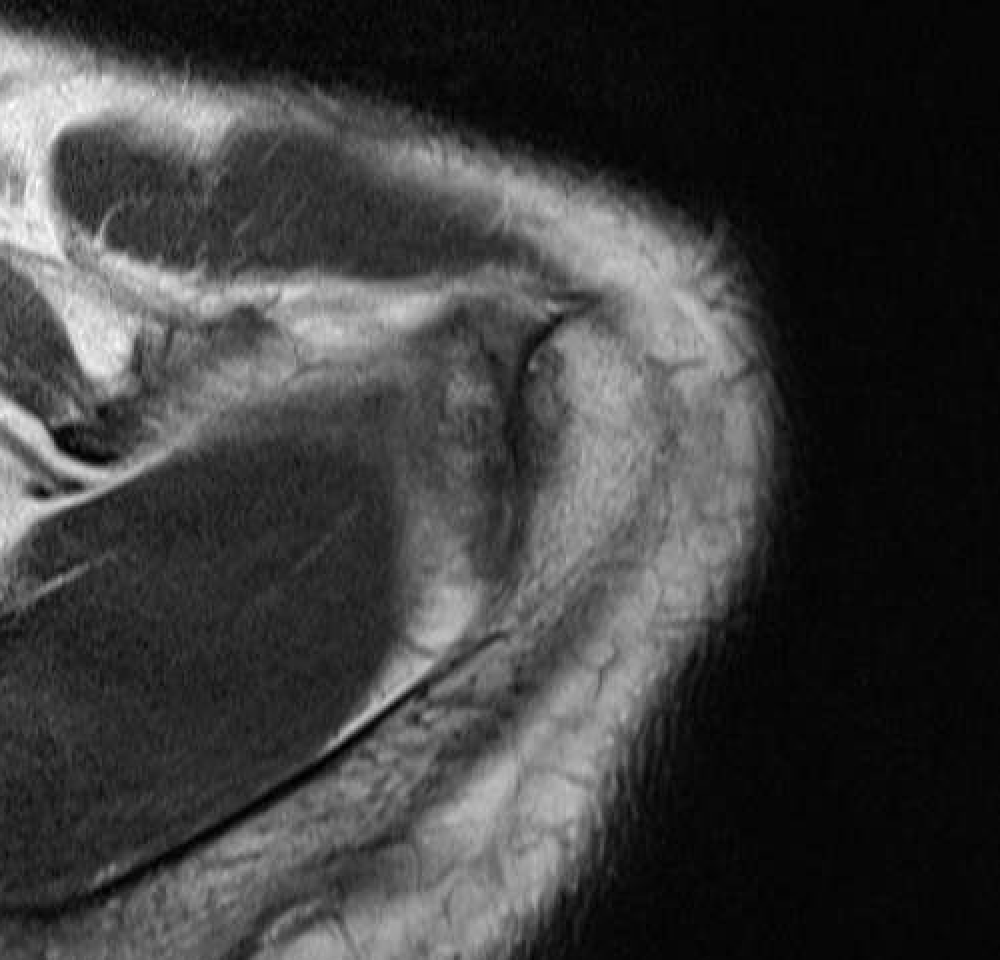
Acromioclavicular joint osteolysis
Bone Scan
Management
Issues
1. Isolated ACJ pathology
2. MRI diagnosed ACJ OA in the setting of rotator cuff tears
- meta-analysis of distal clavicle resection in patients undergoing rotator cuff repair
- 3 RCTs with 208 patients
- no difference in outcome scores
Nonoperative managements
Most patients respond well
- NSAIDs
- activity modification
- physiotherapy
- steroid injection
Operative
Indications for surgery
Isolated ACJ pathology
- x-ray and MRI evidence of degenerative change at ACJ
- tenderness at ACJ
- pain relieved by LA and cortisone injection to ACJ
- failure of non operative treatment
Aim
Resect sufficient distal clavicle to prevent abutment
Options
1. Open excision distal clavicle resection
2. Arthroscopic distal clavicle resection
Hohmann et al Arch Orthop Trauma Surg 2019
- systematic review of 4 studies and 319 patients
- no difference in outomes
Open distal clavicle resection

Technique
- incision centered over the ACJ
- minimal takedown of deltopectoral fascia and anterior deltoid
- incise ACJ capsule longitudinally in midline
- elevate subperiosteally and repair later for stability
- resect 1 cm of distal clavicle only so as to not destabilise clavicle
- must leave conoid / trapezoid ligaments intact
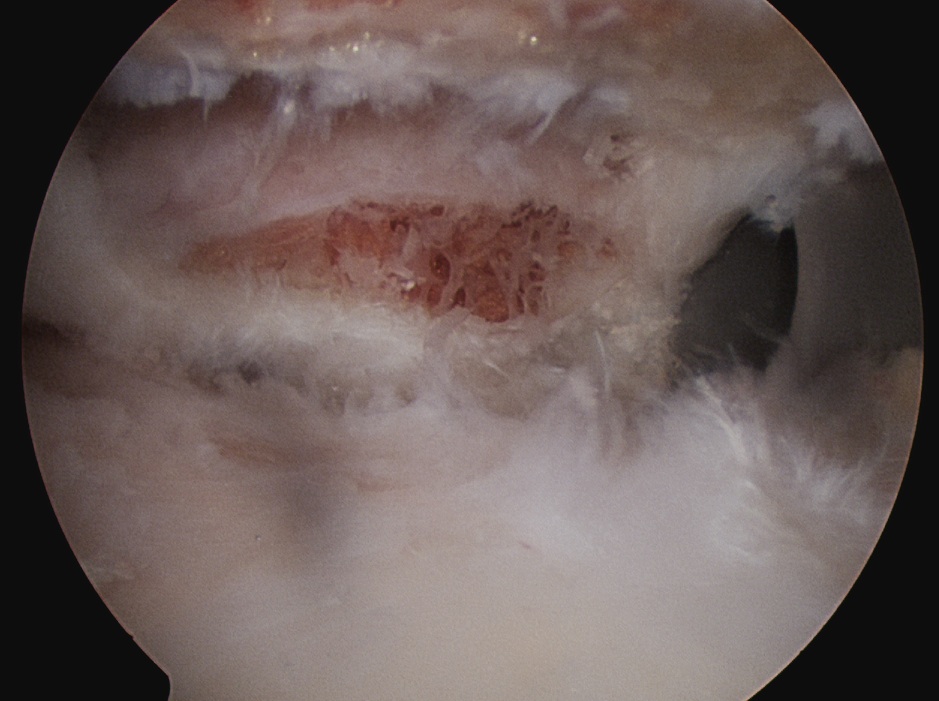
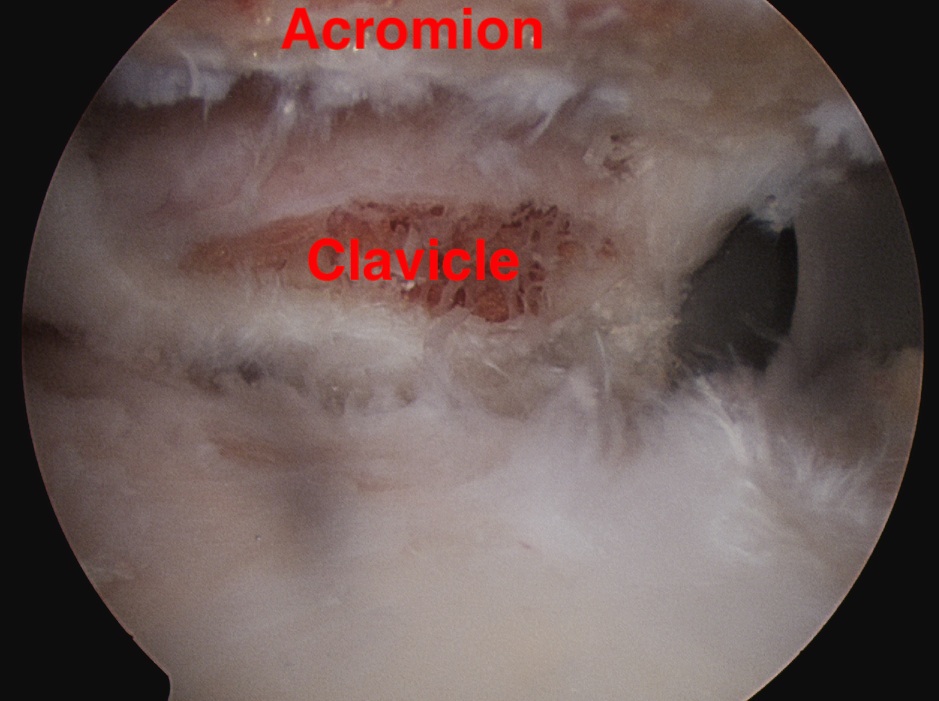
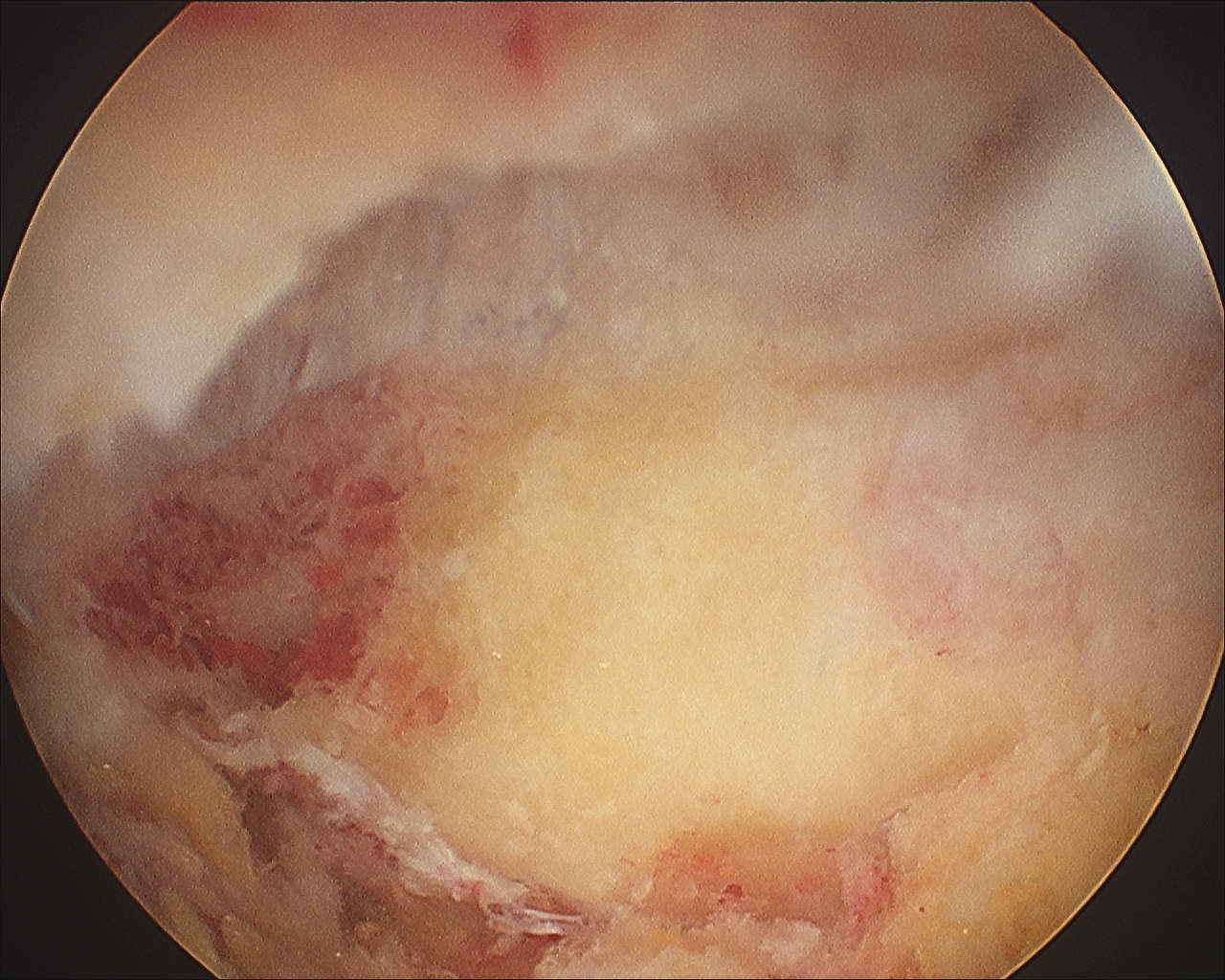
Arthroscopic Distal Clavicle Resection
Advantage
- minimal incisions
- preserves superior AC ligament and deltoid
- low risk of infection
Disadvantage
- potential inadequate resection
- particularly superior and posterior
Technique
1. Identify distal clavicle
- camera posterior portal, electrocautery lateral portal
- remove bursa in subacromial space
- follow anterior acromion medially with cautery
- identify the distal clavicle (push down on clavicle repetitively)
- clean and identify clavicle anterior and posterior
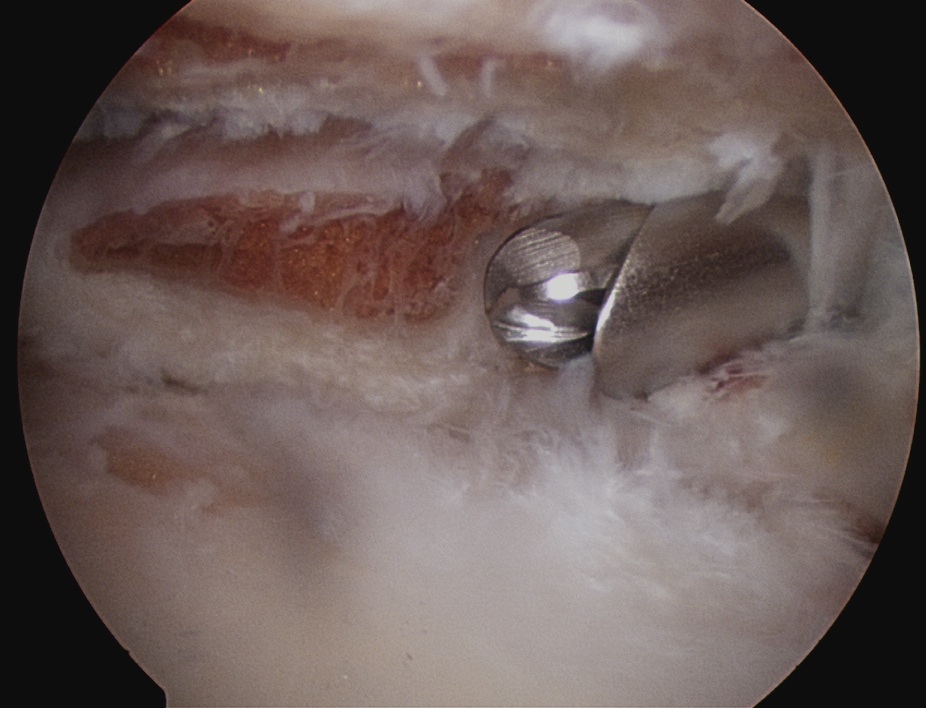
2. Anterior portal
- placed just at lateral aspect of distal acromion
- in line with AC joint
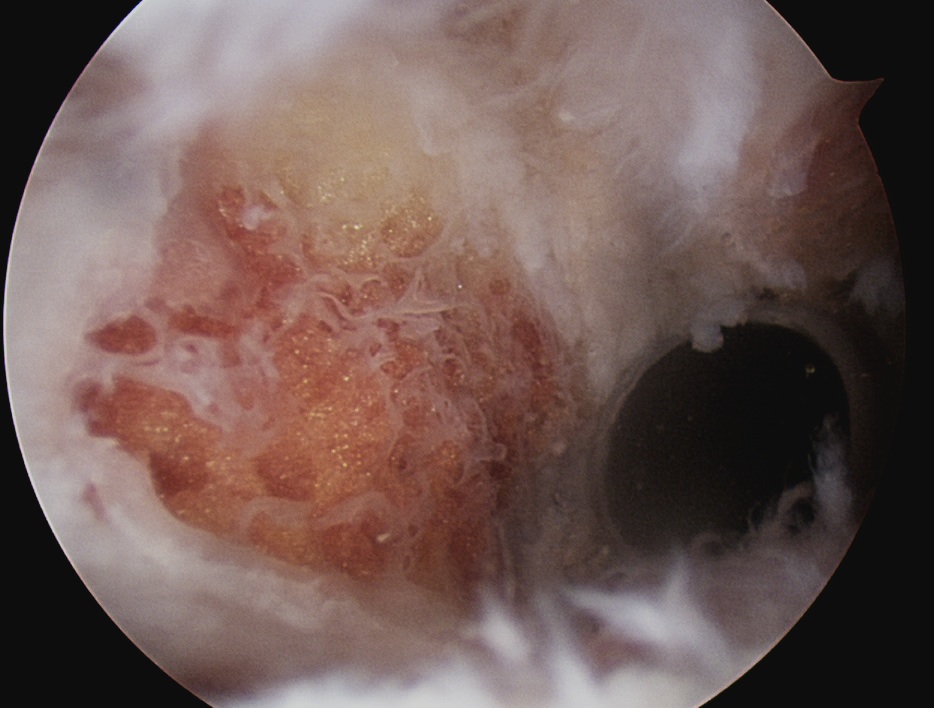
- remove anterior then posterior clavicle
- must remove full thickness of distal clavicle superiorly / be able to visualise superior AC ligament
- must not leave posterior edge
- can place camera in lateral portal to enhance view