

Epidemiology
Men aged 20 - 40
Etiology
Usually occurs in gym with bench press
Increased risk with steroid use / growth hormone
Bodendorfer et al Orthop J Sports Med 2020
- systematic review of 23 papers and 664 injuries
- all male, average age 31
- 63% occurred during weight training
Anatomy
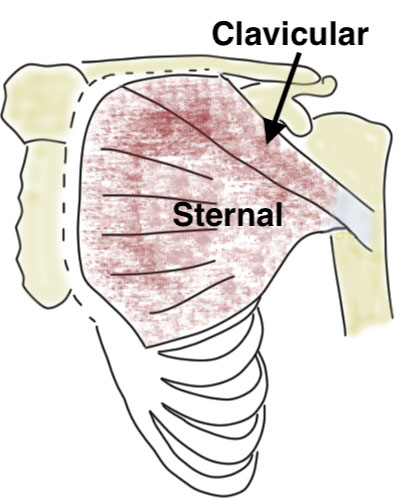
Clavicular and sternal head
- two tendons converge and rotate 90o
- insert lateral to bicipital groove
- superior fibres insert inferiorly and vice versa
Tendon is composed of two lamina
- anterior lamina is clavicular head
- posterior lamina is sternal head
| Clavicular head | Sternal head | Action |
|---|---|---|
| Attaches: medial clavicle and upper sternum | Attaches: Sternum and costal cartilages first 6 ribs | Shoulder adductor / flexor / internal rotator |
| Inserts: lower most aspect of bicipital groove | Inserts: upper most aspect of bicipital groove | |
|
Lateral pectoral nerve C5-7 |
Lateral pectoral nerve C5-7 Medial pectoral nerve C8-T1 |
History
Usually recall significant incident
- tearing sensation
- may hear a pop
- often severe swelling and bruising
Only later when it settles is the cosmetic and functional deficiency apparent
Examination
Significant bruising in the acute phase


Frequently palpable cord present
- pectoral fascia still attached to antebrachial fascia
- not to be mistaken for pectoralis tendon
- prevents full retraction

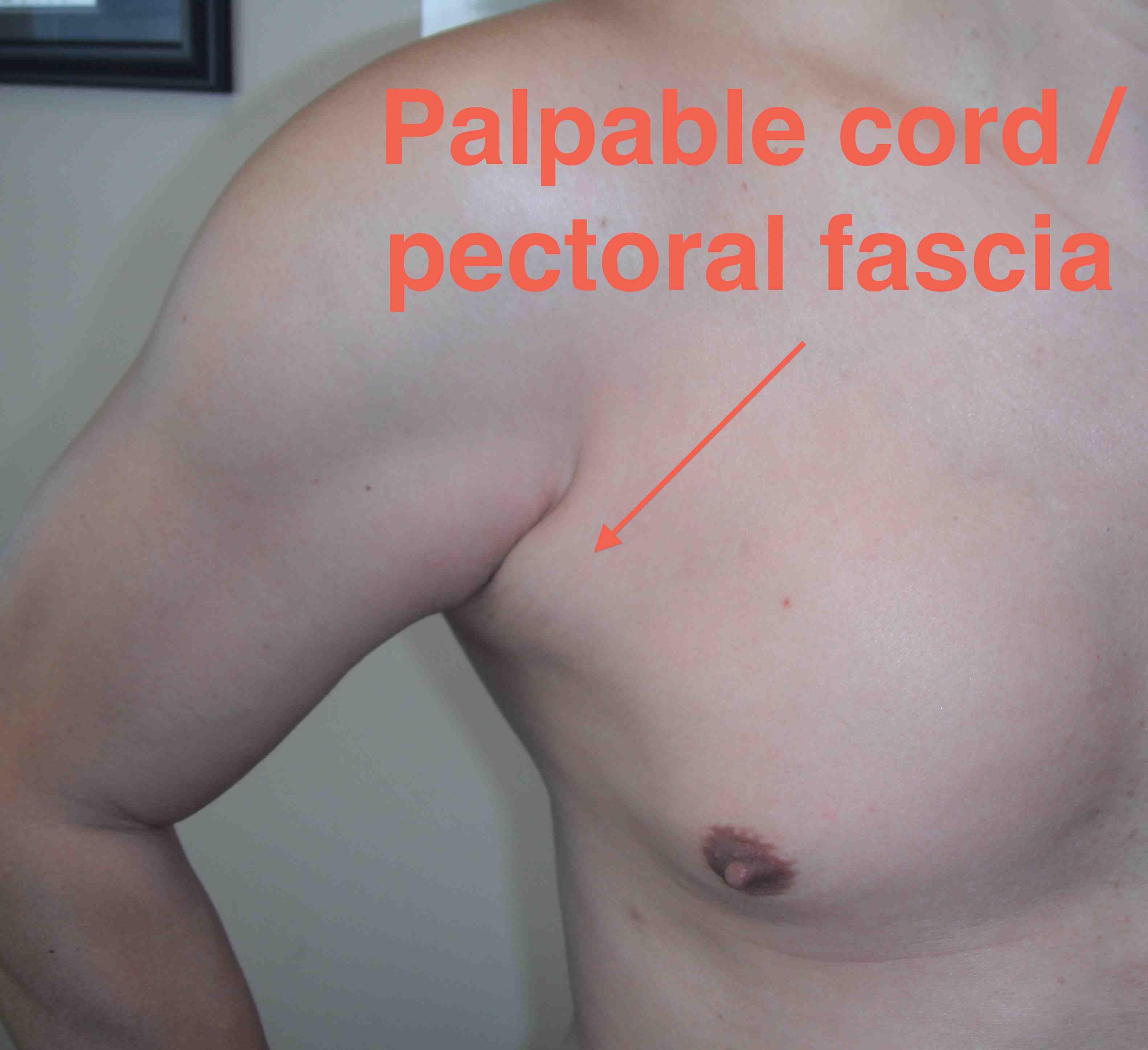
Asymmetry of chest wall


Asymmetry of chronic right pectoralis major with contraction
Pathology
Types
Tendon avulsions off bone
Musculotendinous tears
Isolated tears sternal head > clavicular head
Incidence
- 100 pectoralis major tears
- 35% tendon avulsions
- 60% tears of the musculotendinous juntion
- 5% intra-muscular tears
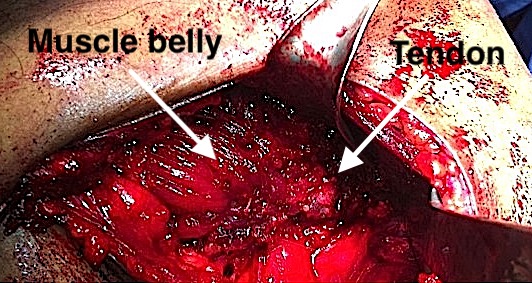
Musculotendinous tears
Avulsion of muscle off tendon at musculotendinous junciton
- not amenable to suture repair
- need allograft reconstruction
Synovec et al Orthop J Sports Med 2020
- MRI study of 72 patients
- 75% sensitive and 80% specific for musculotendinous tears
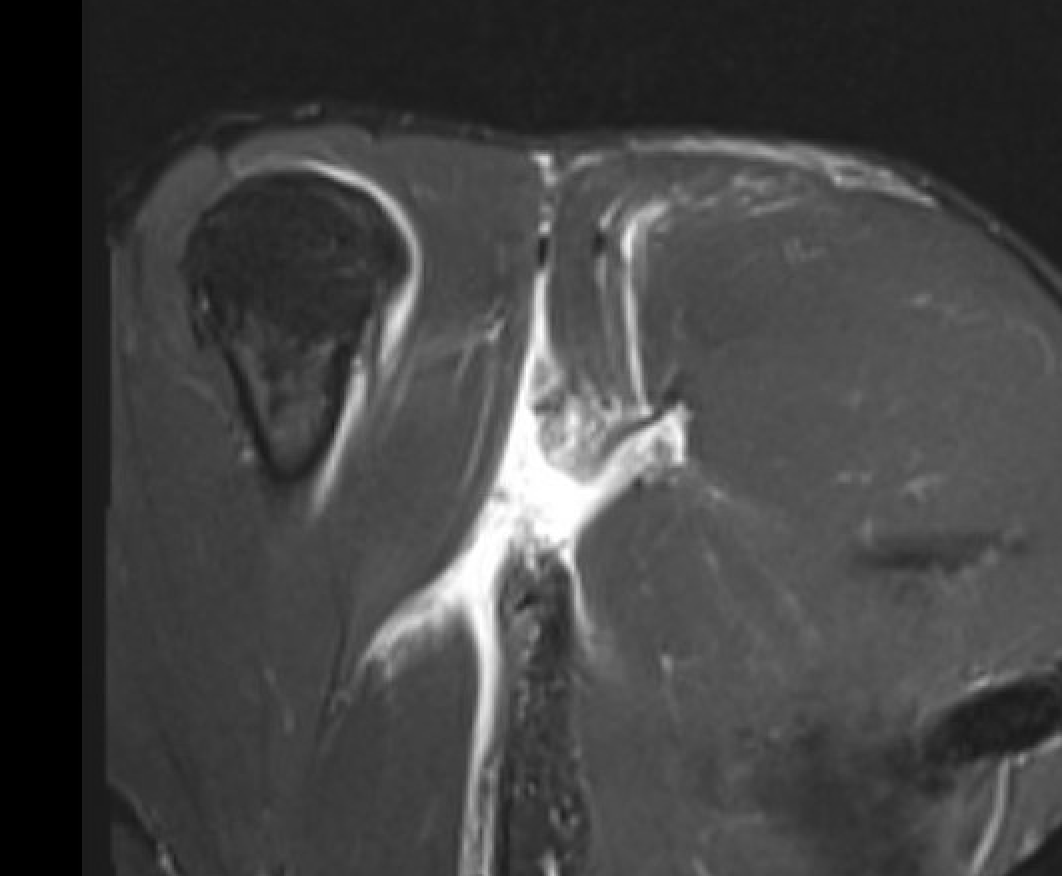
MRI
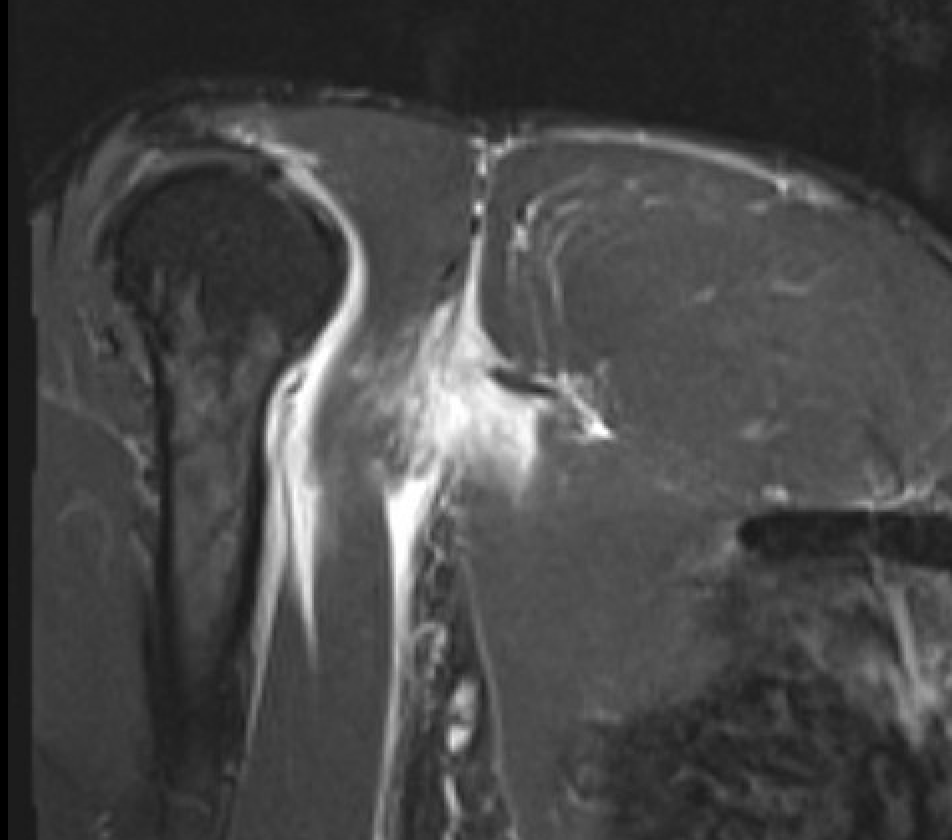
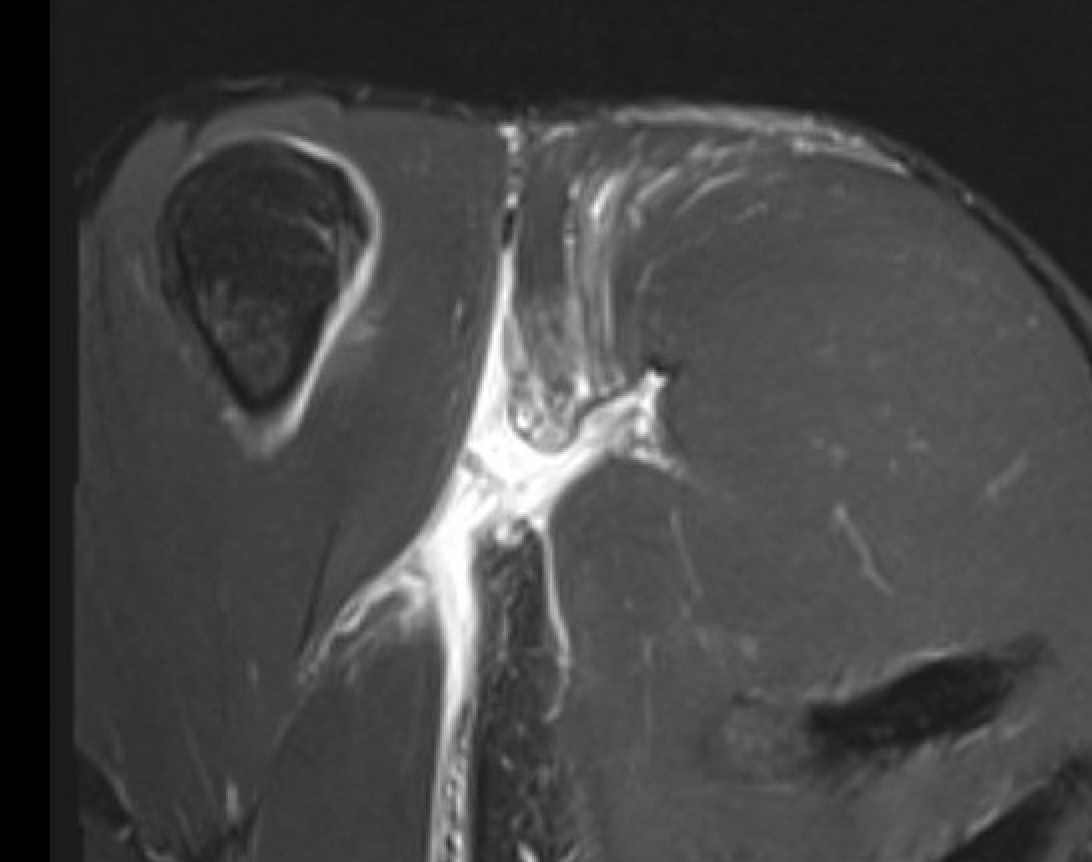
Coronal T2 Right shoulder demonstrating tendon avulsion of both sternal and clavicular heads
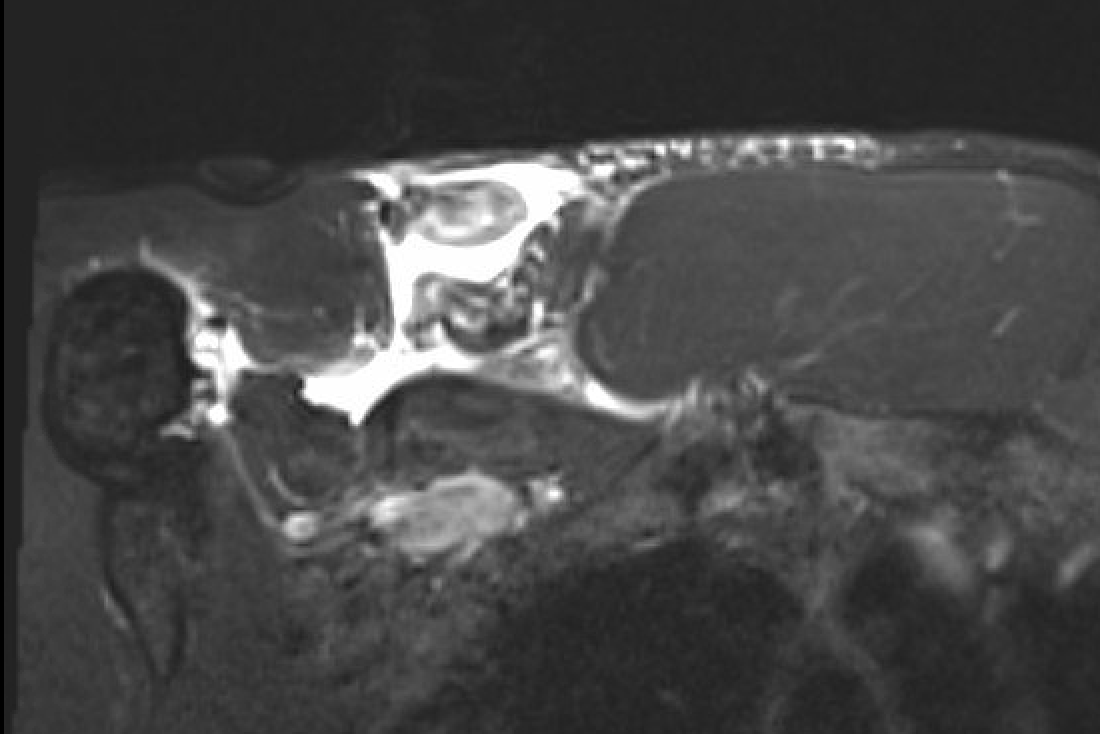
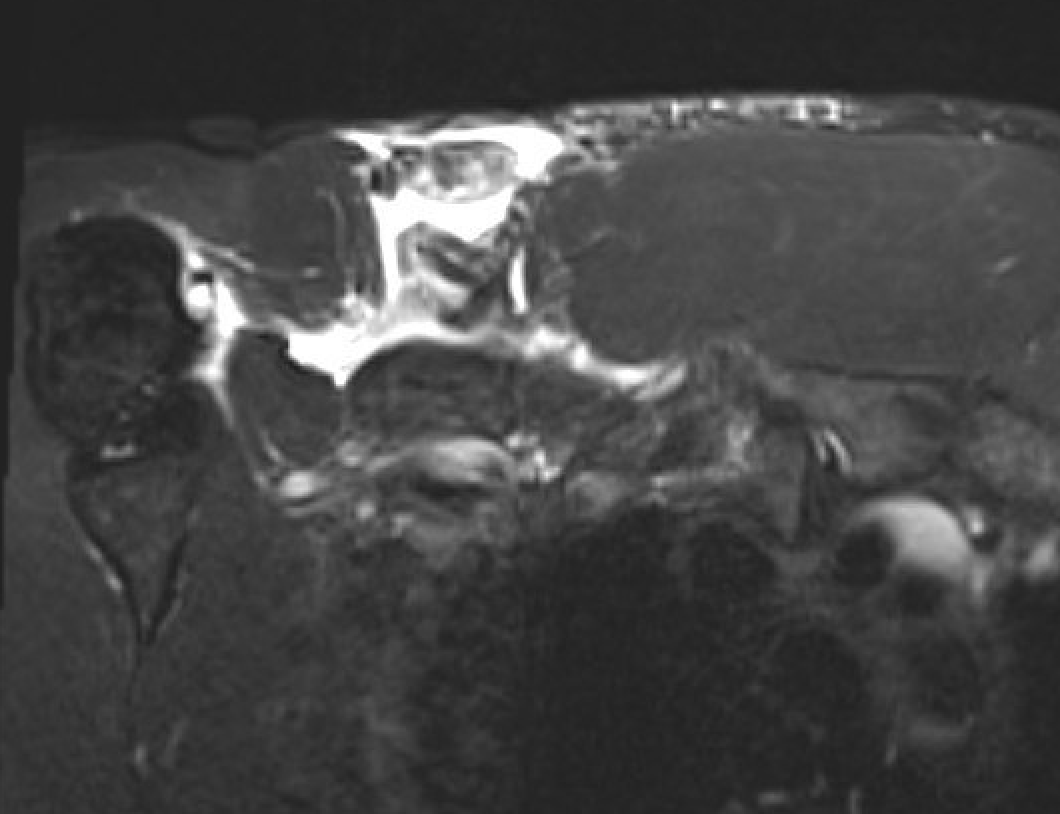
Axial T2 Right shoulder demonstrating tendon avulsion of both sternal and clavicular heads
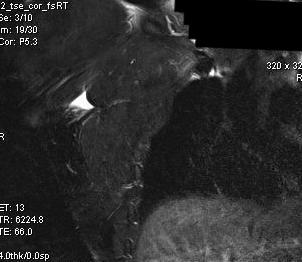

Coronal T2 MRI Right shoulder demonstrating musculotendinous avulsion
Management
Non operative
Elderly / low function
Chronic setting
Bodendorfer et al Orthop J Sports Med 2020
- systematic review of operative versus nonoperative treatment
- operative treatment superior in functional outcomes / strength / cosmesis
Operative
Indications
Acute tears in young patients
Cosmesis i.e. body builders
Acute repair of tendon avulsions
Options - bone trough / suture anchors / cortical buttons

Axillary incision right shoulder
Bone Trough Technique
Beach chair
- incision in axillary skin crease and deltopectoral approach
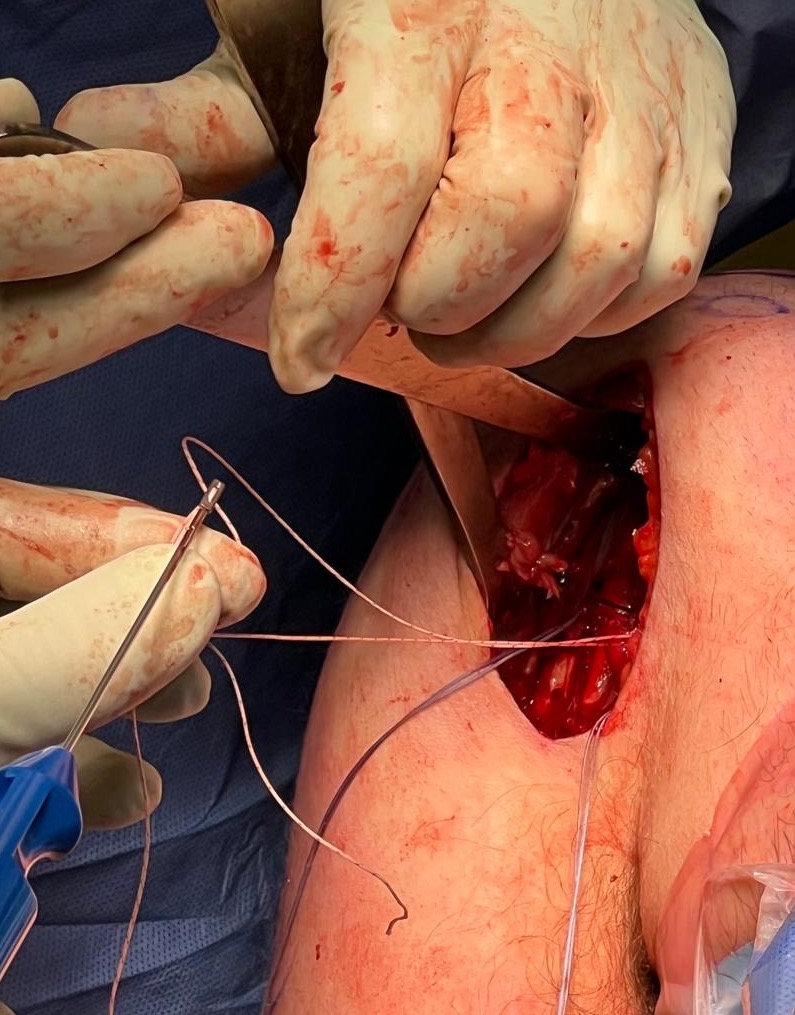
- find pectoralis major tendons medially and Krackow with high strength sutures
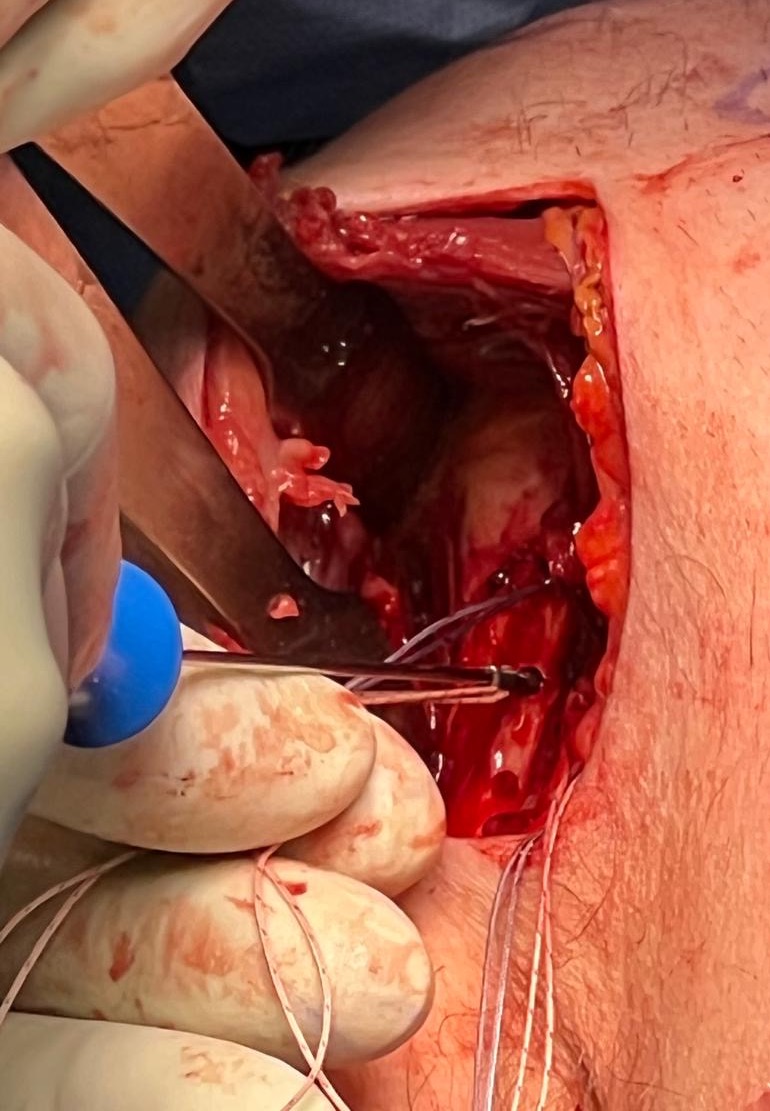
- place Hohmann retractor under deltoid to expose humerus
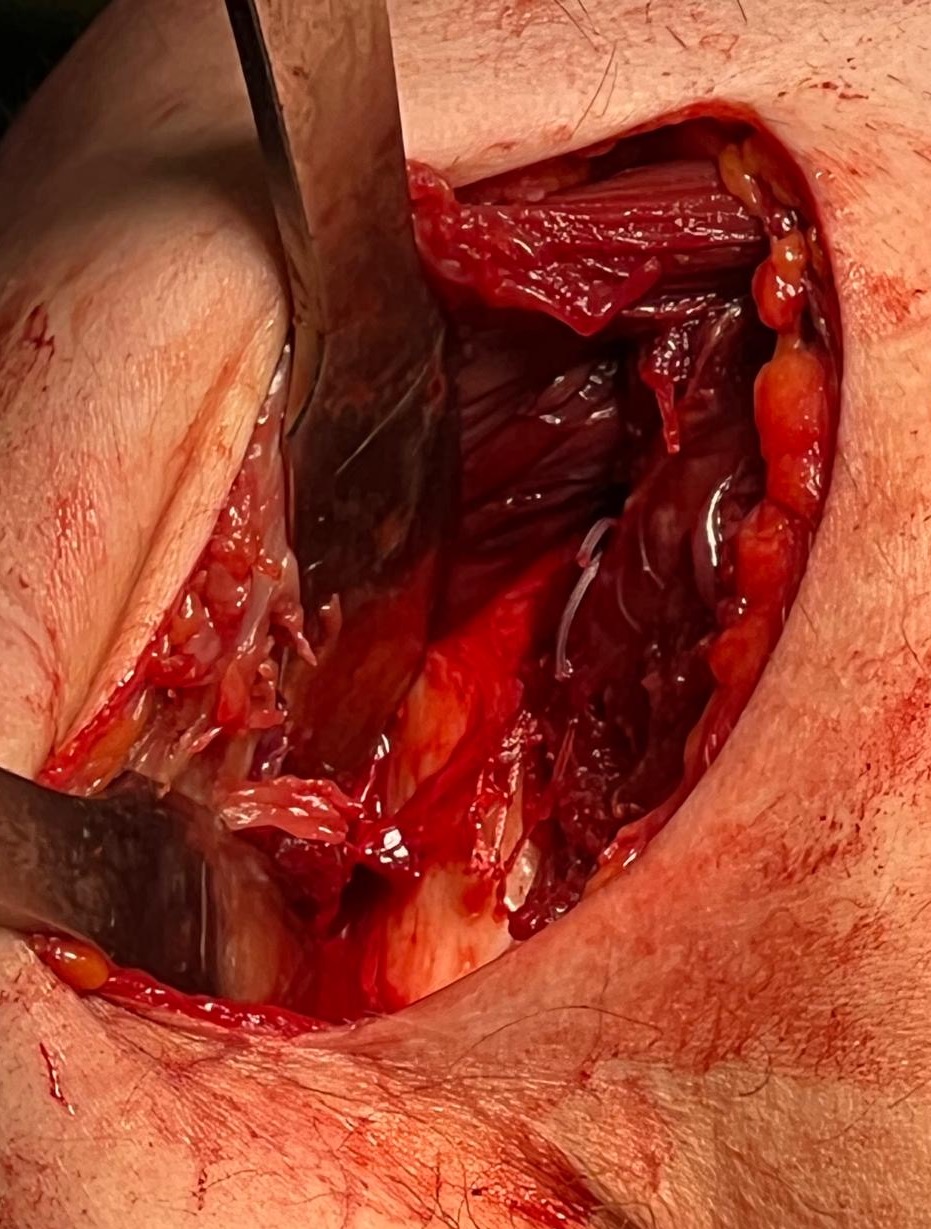
- identify long head of biceps and drill one inch trough in humerus lateral to long head of biceps
- make drill holes with 2 mm drill lateral to trough
- use suture passer to pass sutures into trough and out lateral drill holes
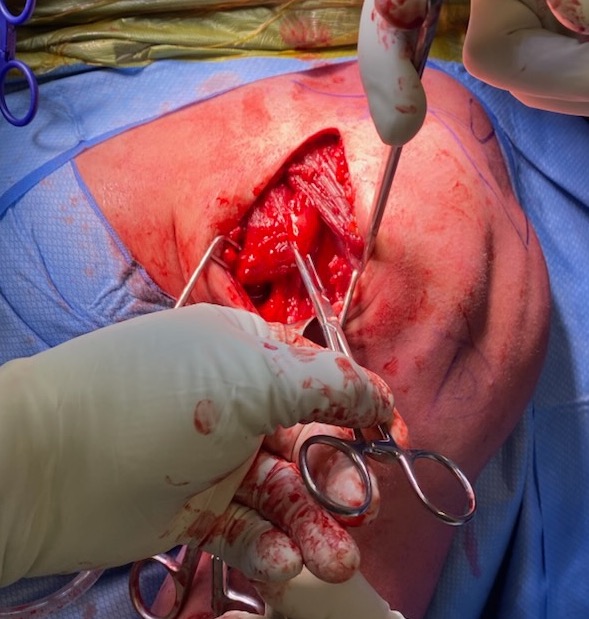
- pull tendon into trough and tie sutures
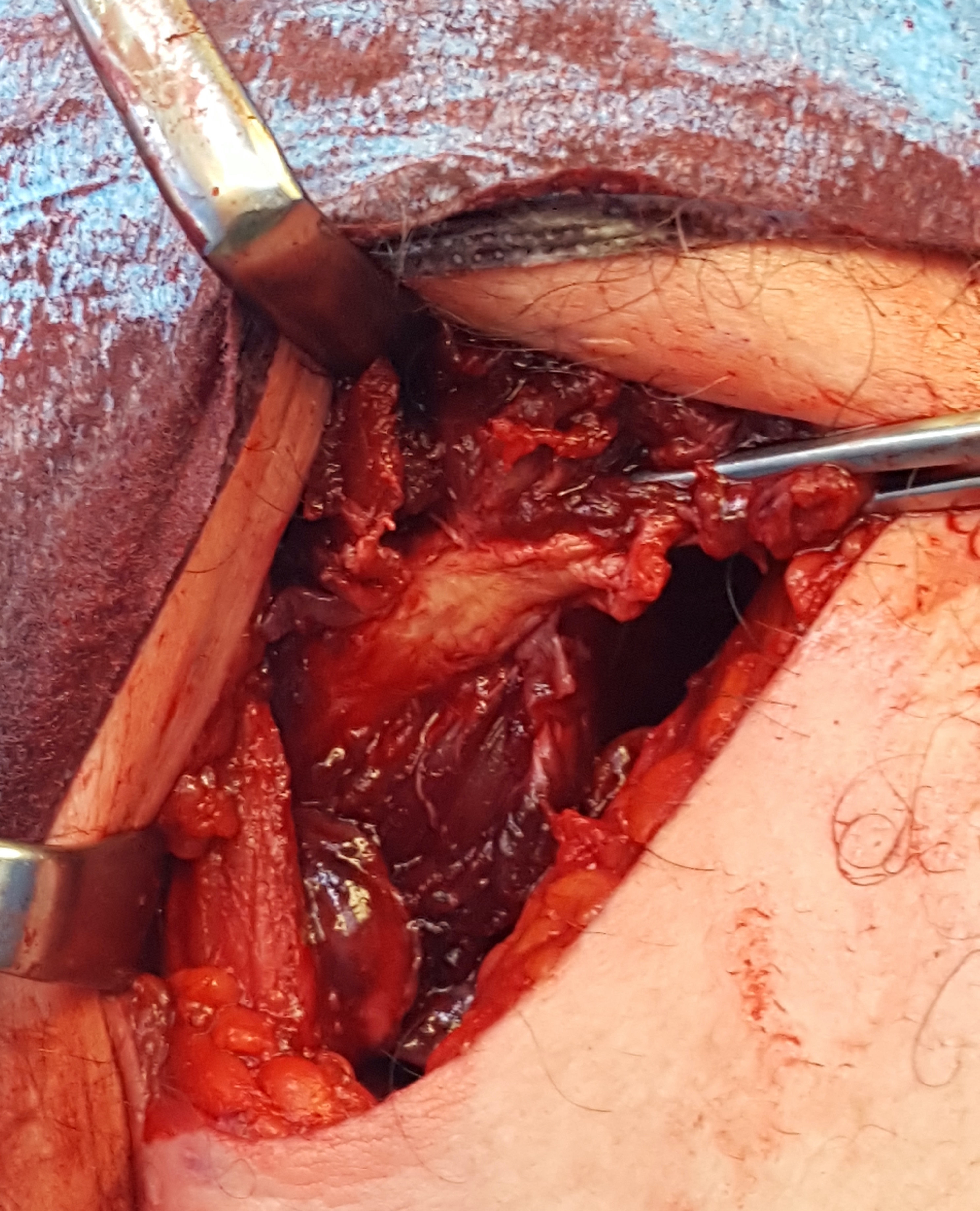
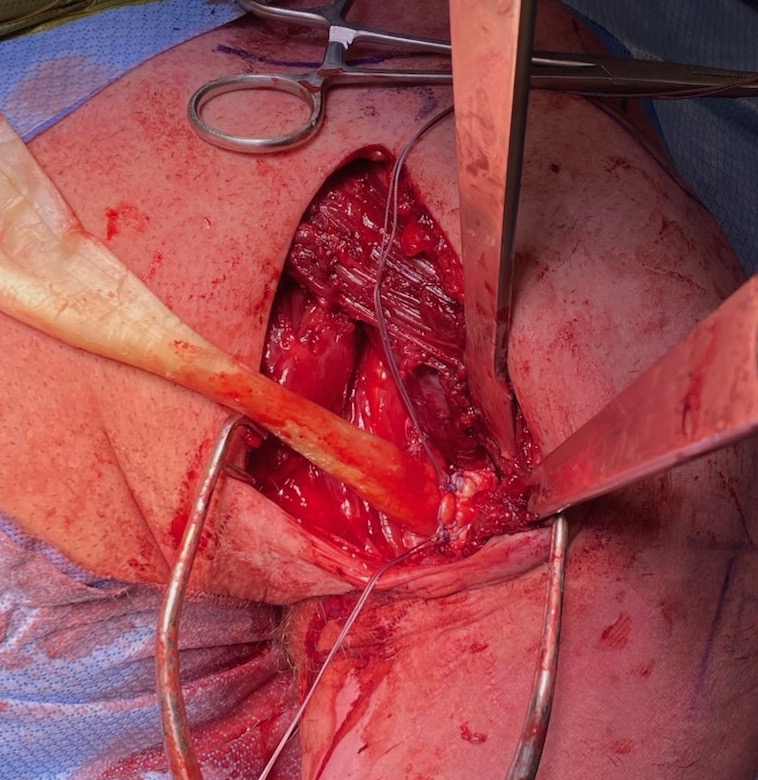
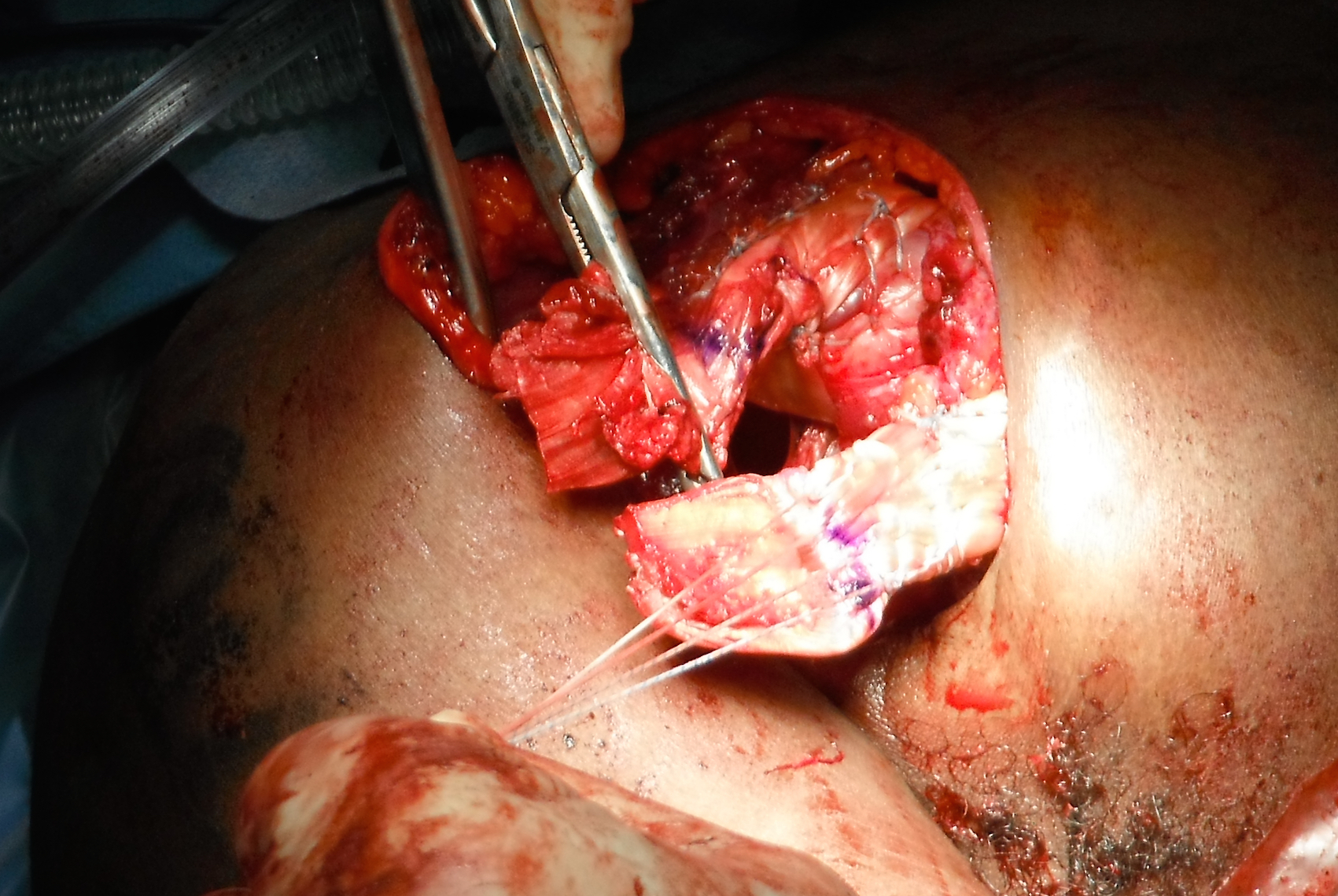
Axillary crease incision in right shoulder, with Kocher forceps on the torn pectoralis major tendon
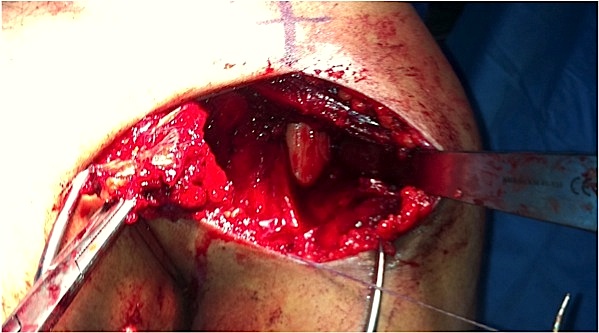
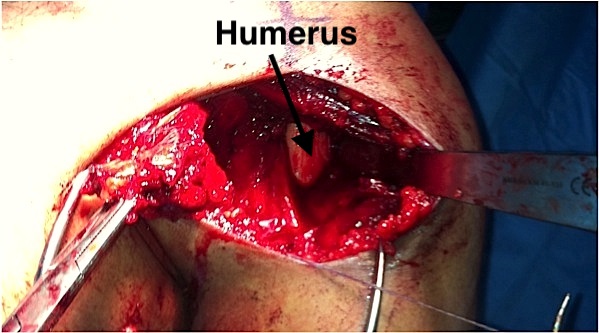
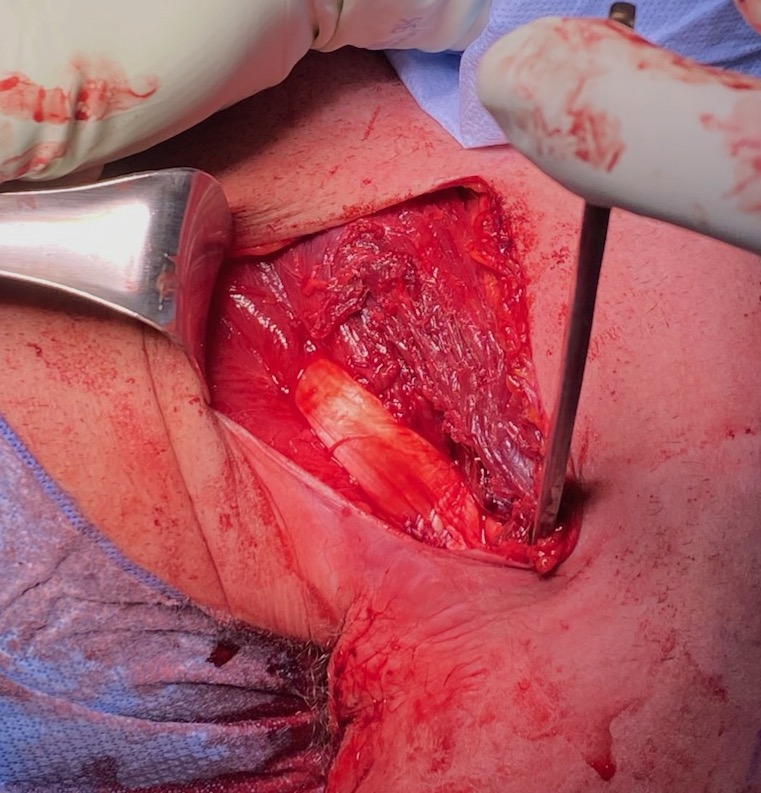
Right shoulder, with Hohmann retractor exposing humerus
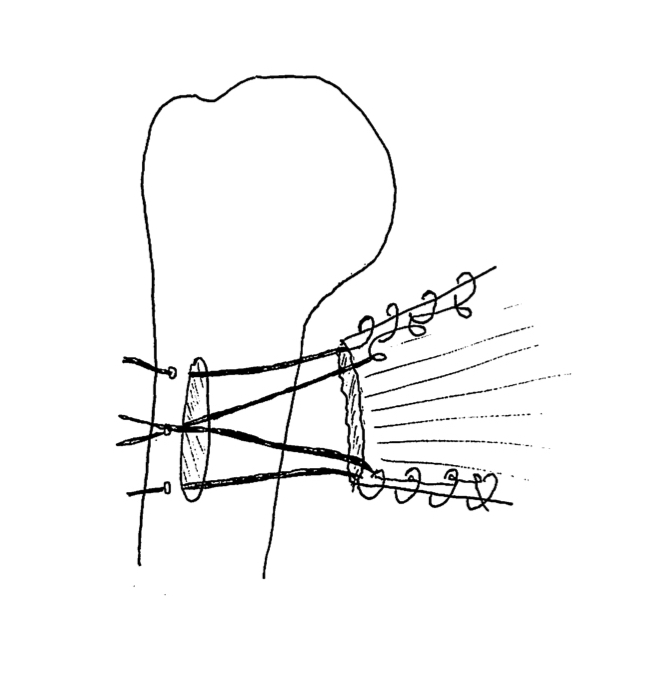
Bone trough with sutures passed through lateral drill holes
Completed repair
Cortical button technique
Arthrex surgical technique video pectoralis major
Arthrex surgical technique repair with cortical button

Results
Bodendorfer et al Am J Sports Med 2020
- systematic review of operative repair
- no difference between different surgical techniques
- acute repair superior to chronic repair
Bodendorfer et al Orthop J Sports Med 2020
- systematic review of operative v nonoperative treatment
- complication rate 14%
- infection <1%
- DVT < 1%
- re-rupture 3%
- persistent pain 3%
Balazs et al Am J Sports Med 2016
- 214 military patients undergoing surgery
- at 12 months, 95% return to active duty
Allograft Reconstruction of Musculotendinous / Chronic Pectoralis Major tears
Technique
Surgical technique video allograft reconstruction
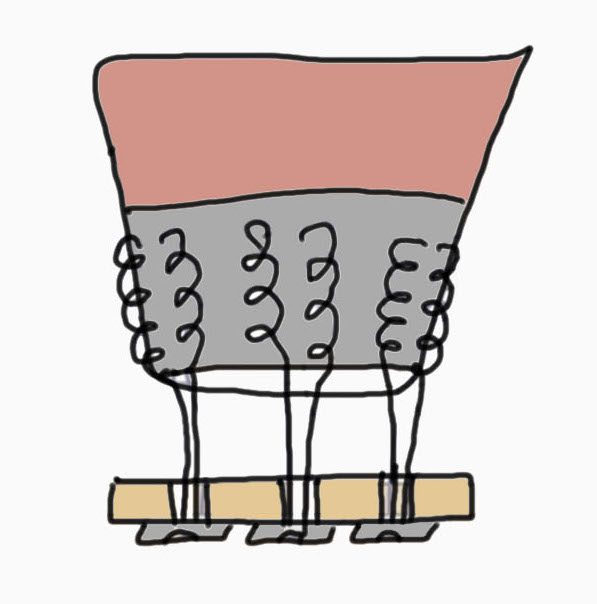
Tendoachilles graft with bone block cut off
- pass through allograft tendon through muscle in pul ve taft method
- tie down into bone trough in humerus as per usual technique

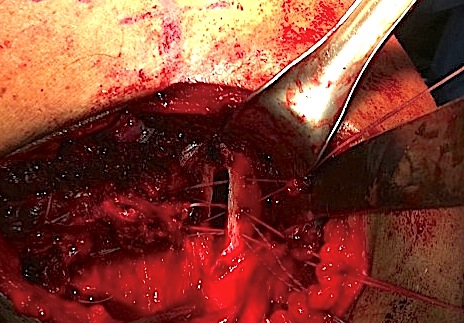
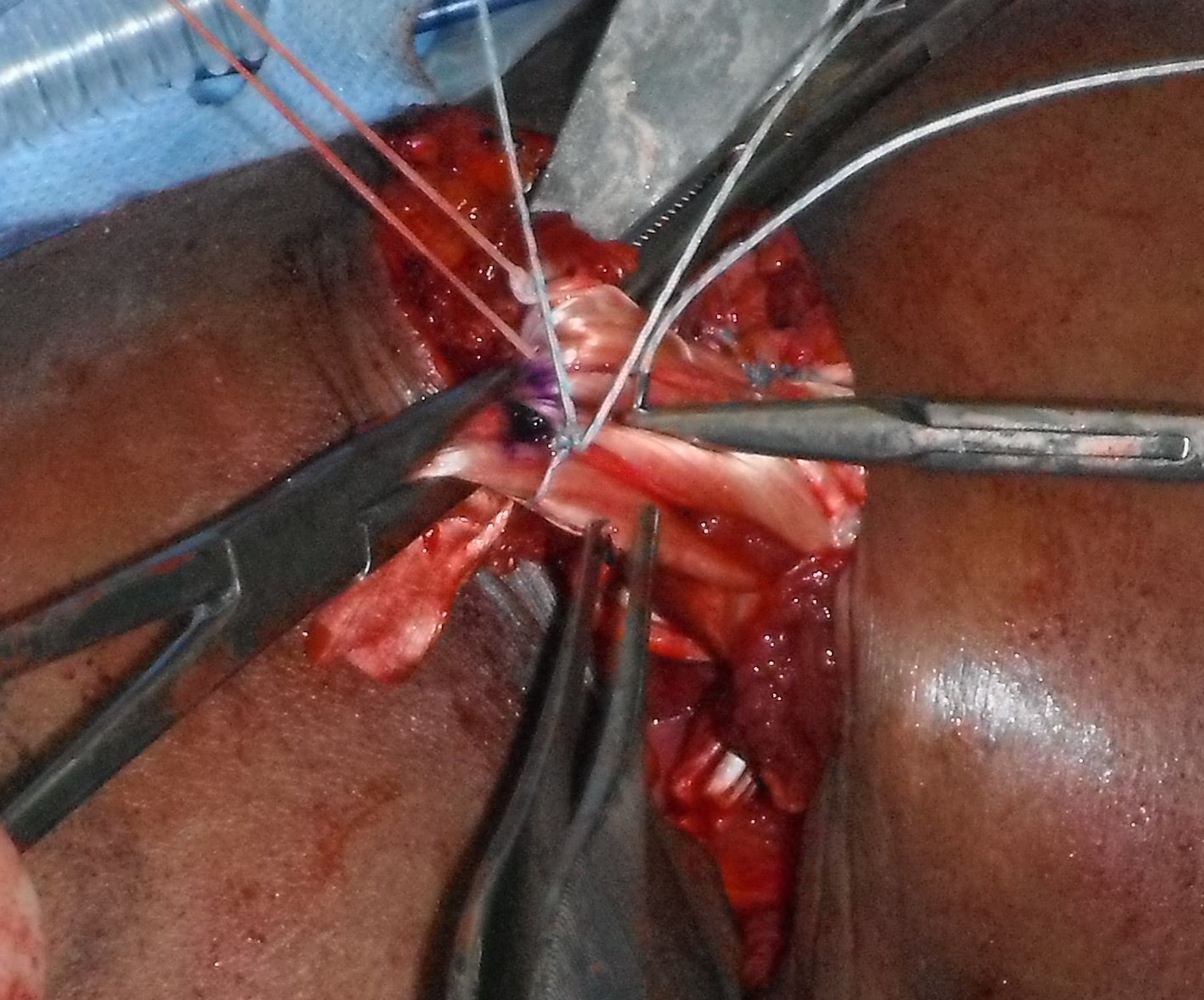
Acute musculotendinous pectoralis major rupture
Allograft reconstruction: achilles tendon sutured anchored to humerus, and pul ve taft through muscle belly
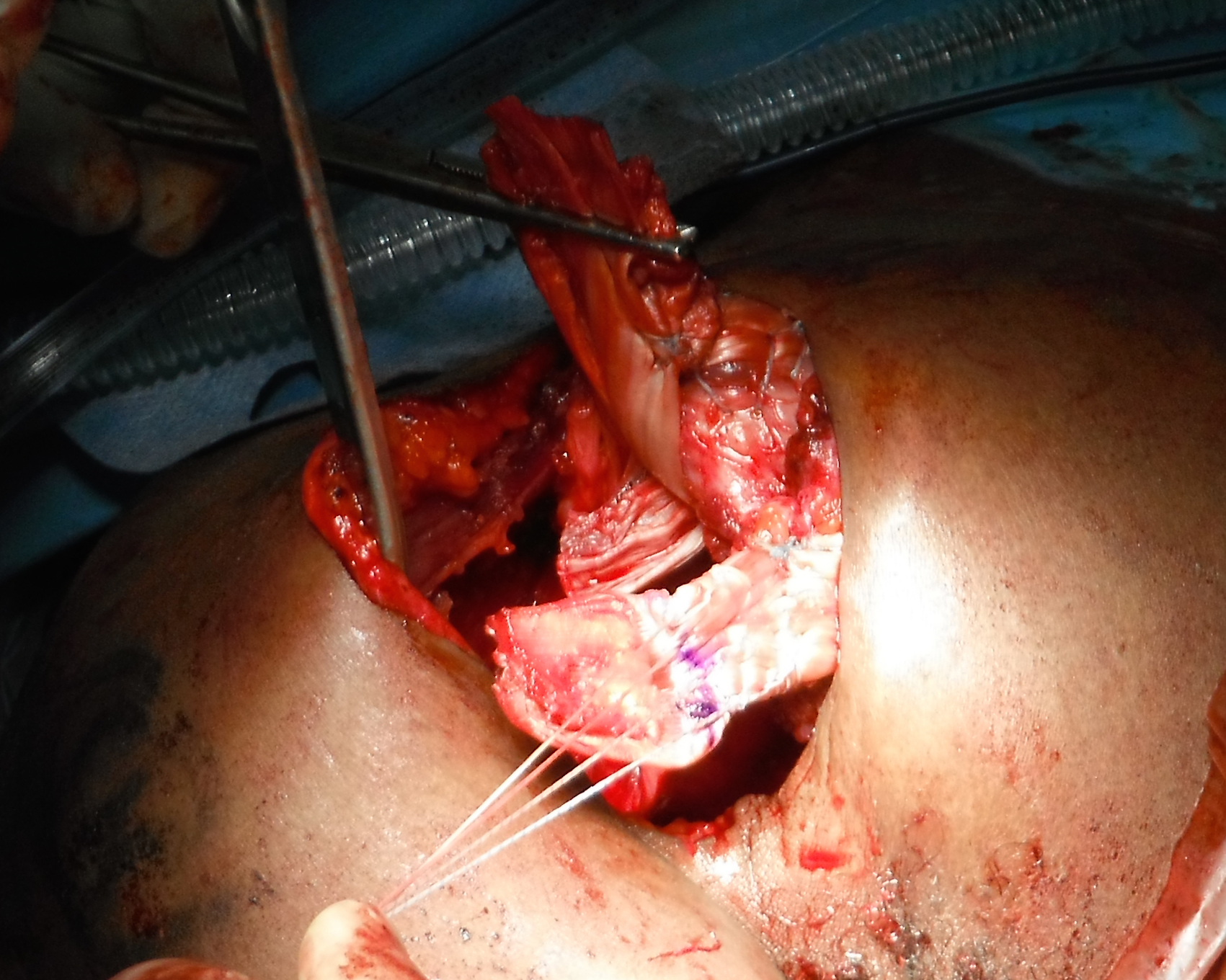
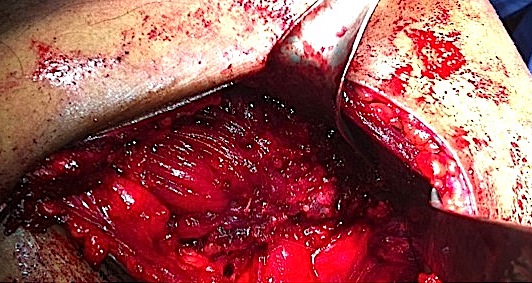
Right shoulder: allograft has been passed through sternal and clavicular muscle bellies and is being sutured back onto itself
- 9 military patients requiring allograft reconstruction
- 5/9 had good or excellent results