


Epidemiology
Quite rare in the adult population
Usually discussed with radial head fractures
Indications for surgery


> 30o angulated
Displacement
Surgical Options
ORIF
- headless Compression Screws
- low profile plates
Radial head arthroplasty
Results
Keil et al J Orthop Surg Res 2018
- 14 patients undergoing surgery for radial neck fractures
- 50% revision surgery
- stiffness, pain, failure of fixation, nonunion
- more common with use of plates than with screws alone
- more complex fractures needed plates
- 34 complex head and neck fractures undergoing ORIF with modern locking plates
- 1 nonunion
- 1 poor result
- 32% plate removed
- excellent flexion / extension
- supination 60 degrees, pronation 70 degrees
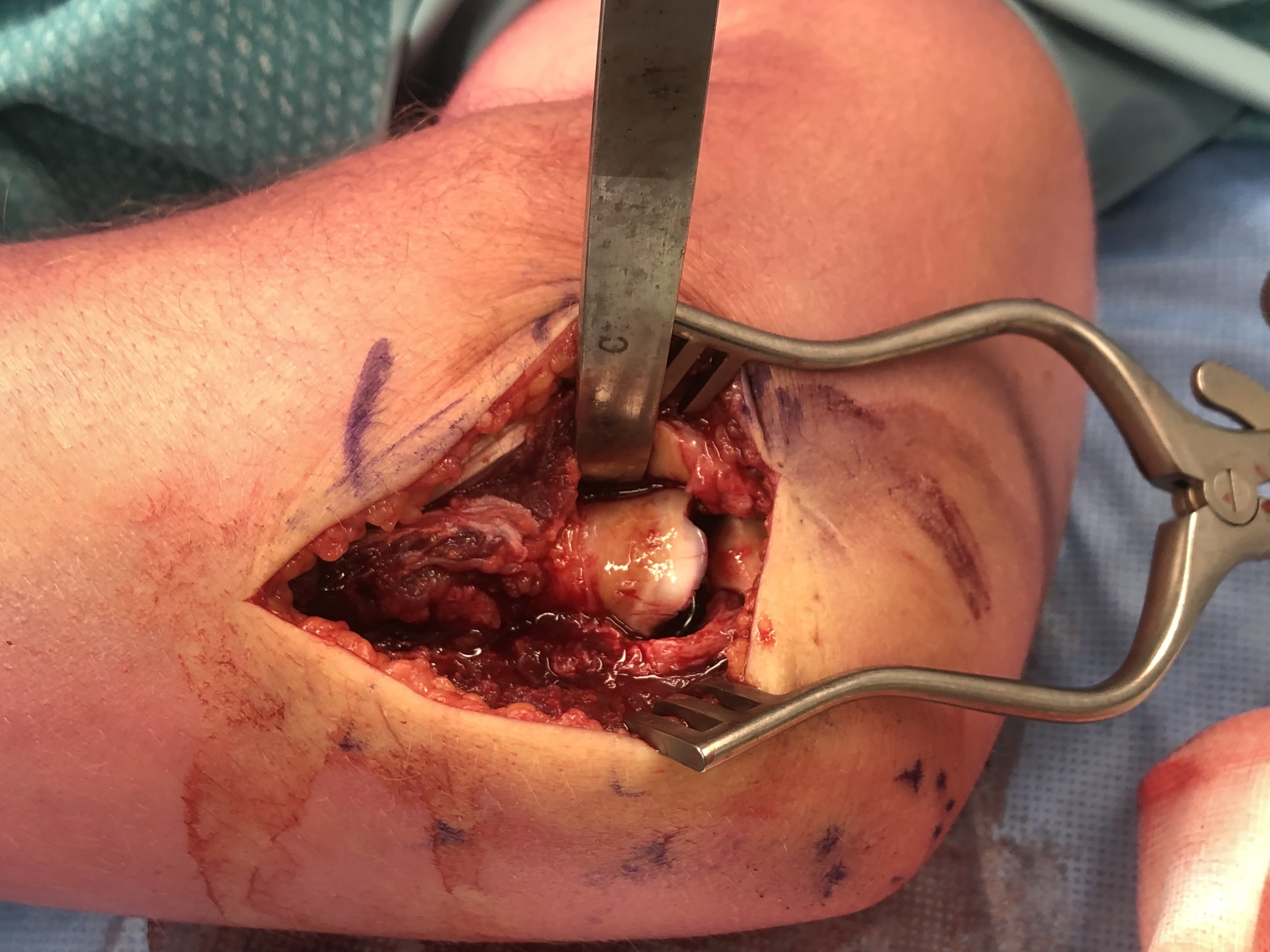
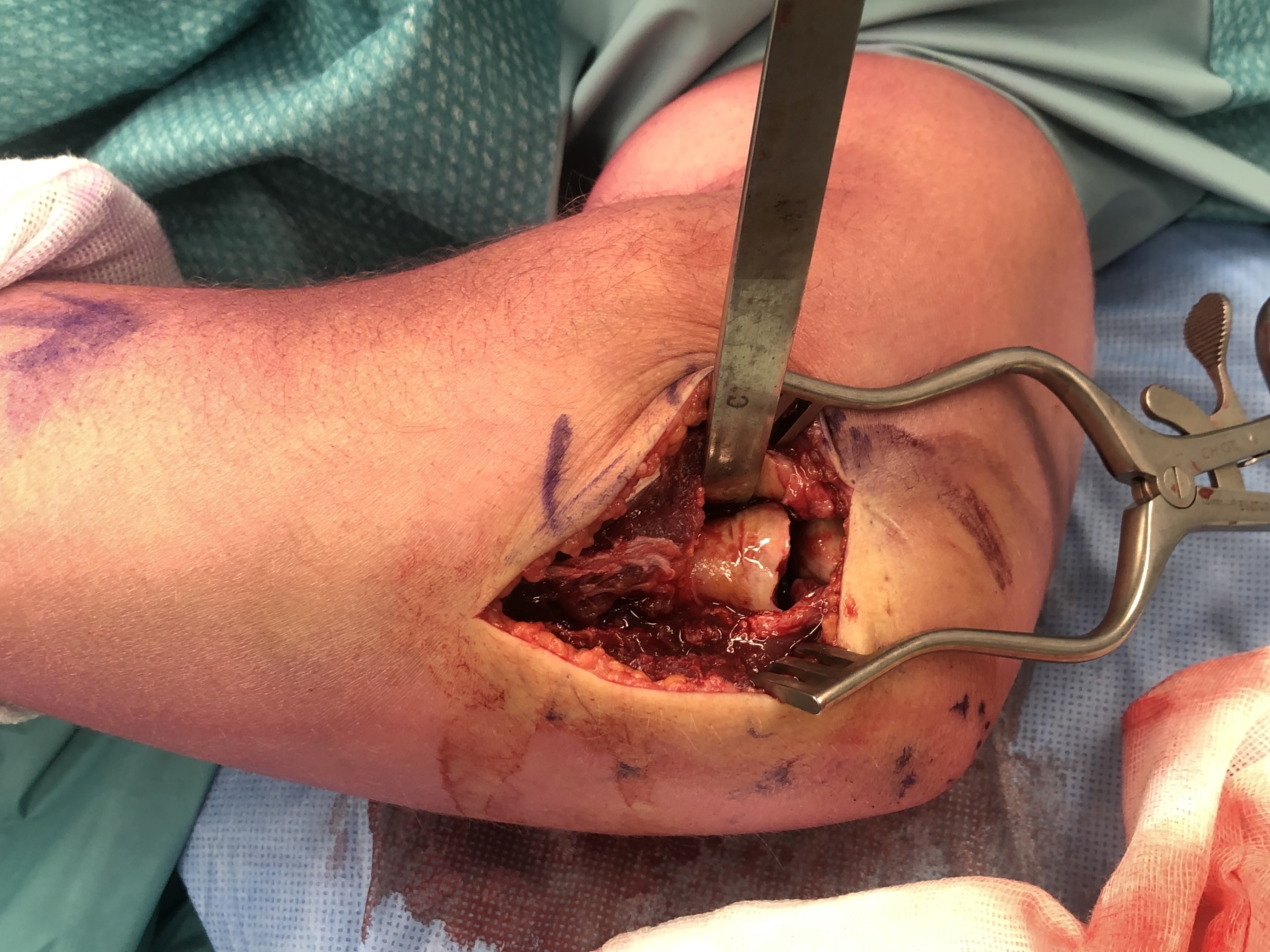
Approach
Lateral approach
- divide annular ligament
- elevate supinator from radius lateral to medial
| Kocher approach | Kaplan approach | Hotchkiss approach | Boyd approach | |
|---|---|---|---|---|
| Interval |
Between anconeus and ECU
|
Interval between EDC and ECRB |
Split EDC |
Elevate Anconeus and ECU Detach supinator from ulna |
| Disadvantage |
May risk injury to LCL |
May risk injury to PIN
|
May risk injury to PIN | May risk injury to PIN |
| Advantage |
May make LCL repair easier
|
Protects LCL | Protects LCL | Protects LCL |
AO surgery lateral approaches to elbow
Headless compression screws
Kocher / Kaplan approach
- dissect muscles off capsule
- divide capsule in line with incision / create anterior and posterior flaps
- pronate forearm to protect PIN
- no Hohmann retractors anteriorly and limit distal dissection
- divide annular ligament
- reduce fracture
Identify safe zone for implants
- posterolateral portion of cartilage / yellow and thinner, non articulating cartilage
- 90o arc between radial styloid and Lister's tubercle
2.5 or 3.5 headless compression screws proximal to distal
Repair annular ligament


Completely displaced radial neck fracture



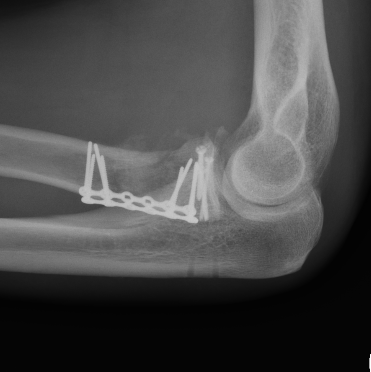
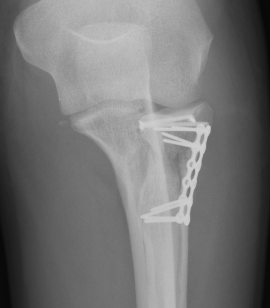
ORIF with plates



Approach
Lateral approach
For extended radial neck fractures may need anterior approach to forearm
AO surgery lateral approaches to elbow
AO surgery anterior approach to forearm
Technique
AO surgery reference T plating radial neck
Vumedi radial neck plating video
Vumedi radial neck plating video 2
Acumed radial head plating technique PDF
Medartis radial head and neck plating system
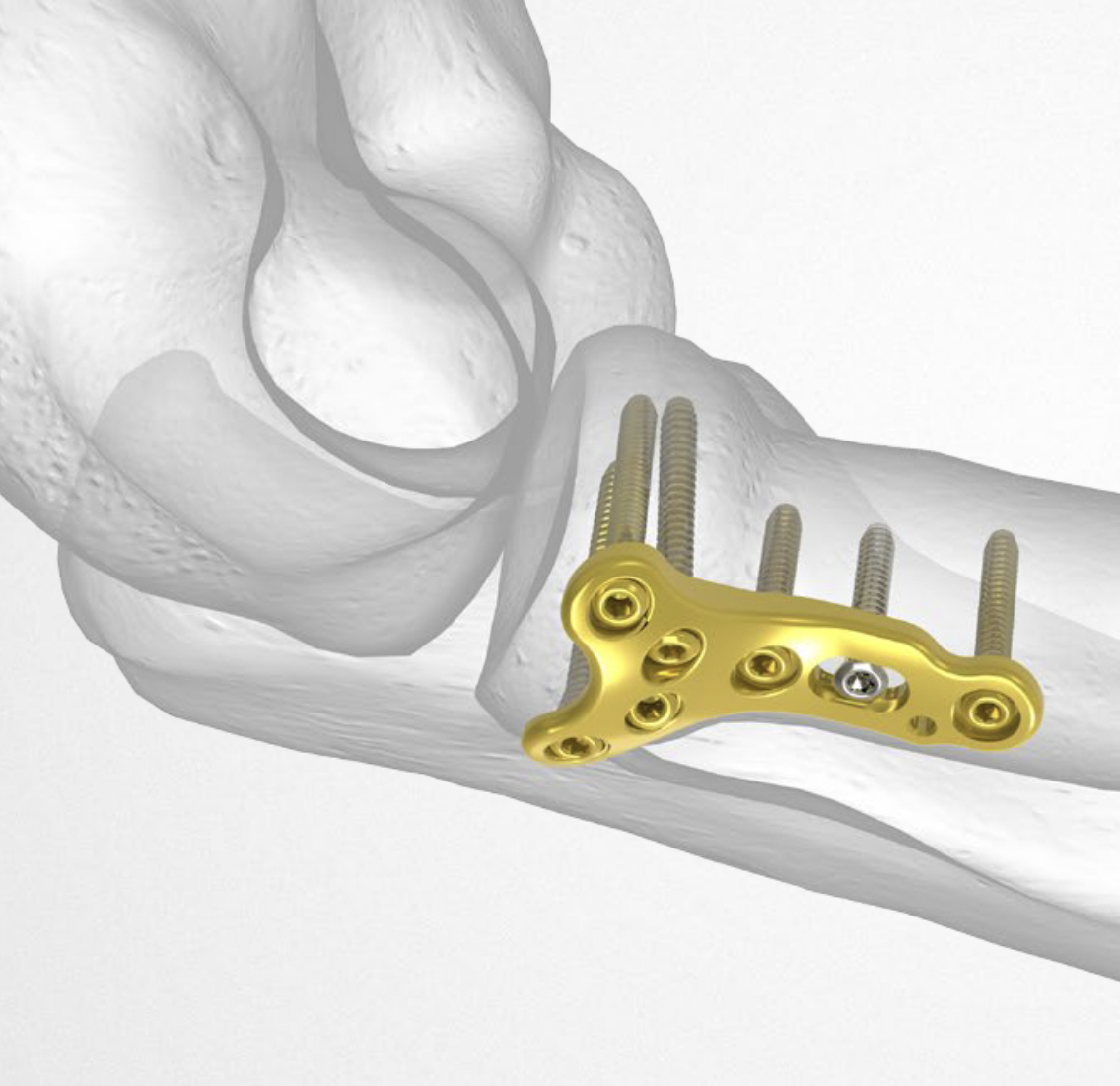
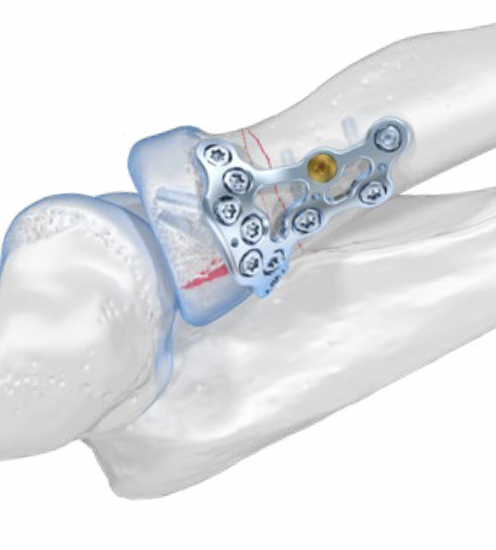
Acumed and Medartis Radial Head / Neck plates
Lateral approach
- identify safe zone (90 degrees between radial styloid) and Lister's tubercle)
- lag articular surface first if required
- pre-contoured low profile plates
- distal limit is bicipital tuberosity
- check ROM intra-operatively
- plates often bulky and may limit ROM
- close annular ligament
Radial Head Arthroplasty




