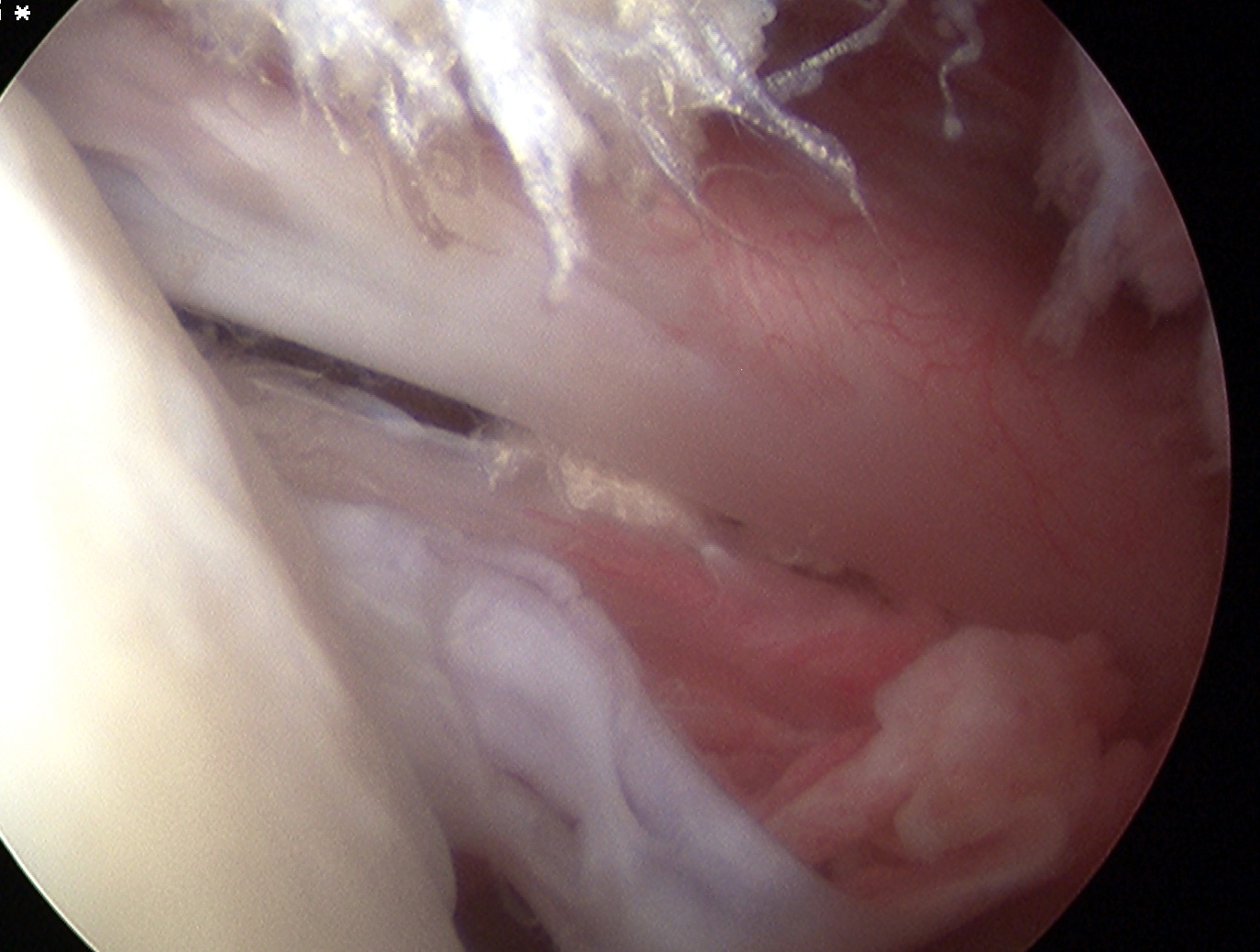
HAGL
Definition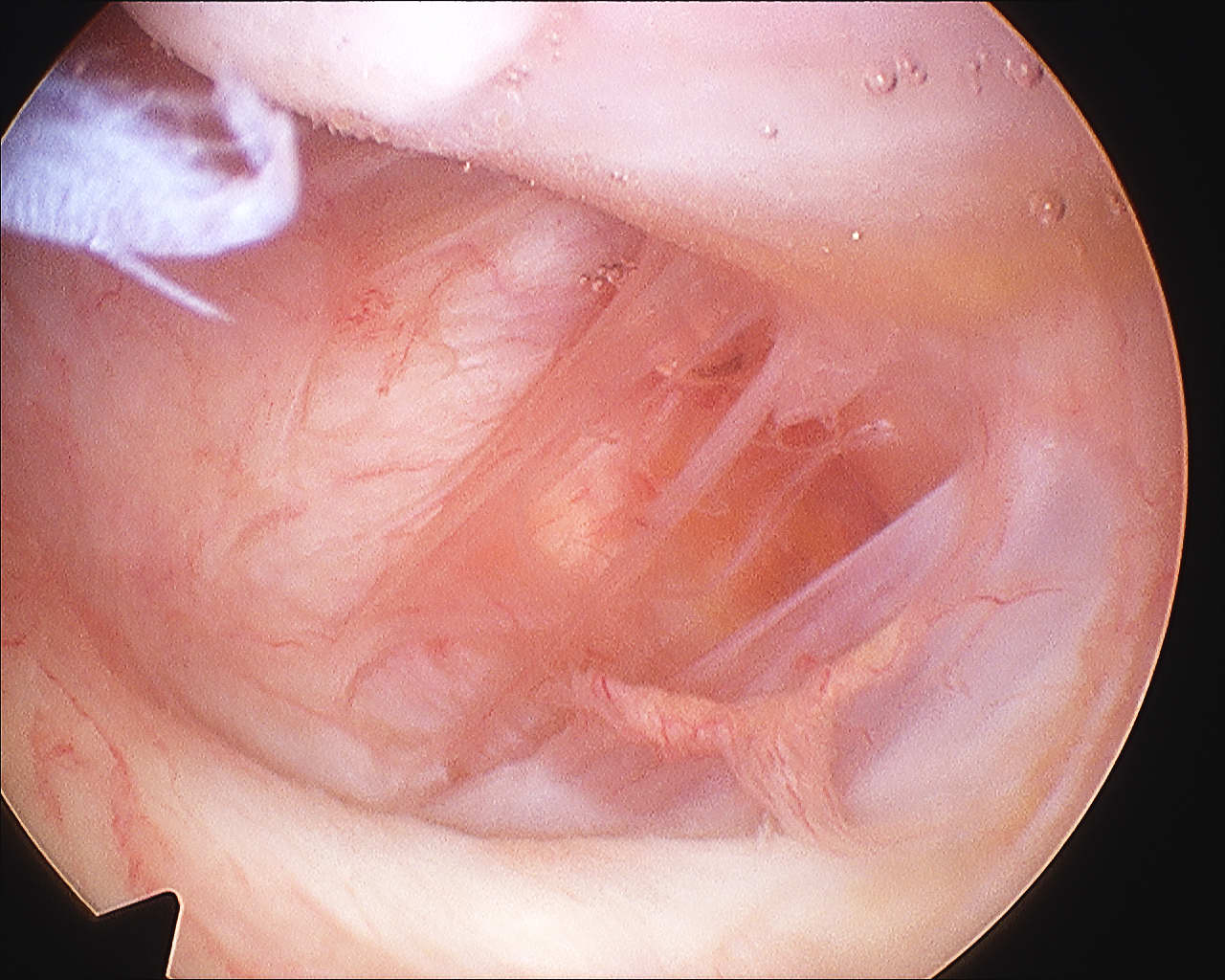
Humeral Avulsion of Glenohumeral Ligament
Incidence
Bokor et al JBJS Br 1999
- 514 cases surgical treatment traumatic instability
- incidence 7.5%
- 25% associated SSC tear
- likelihood of HAGL if no Bankart or MDI 27%
Humeral Avulsion of Glenohumeral Ligament
Bokor et al JBJS Br 1999
- 514 cases surgical treatment traumatic instability
- incidence 7.5%
- 25% associated SSC tear
- likelihood of HAGL if no Bankart or MDI 27%

Size
2 x as strong as ACL
About the same length as ACL 38 mm
Cross sectional area 150% of ACL
13 mm diameter (thicker)
2 Bundles
1. Anterolateral
- most important
- double the size of the posteromedial
- tight in flexion
- try to reconstruct this bundle
Most common
- fascia lata on greater trochanter
- iliopsoas on lesser trochanter
1. Intra-articular structures
- labrum
- ligamentum Teres
- loose bodies
- synovial chondromatosis
- osteochondoma
2. Extra-articular structures
- fascia lata on greater trochanter (common)
Stage 0
Natural history mixed
- depends on size of lesion and diagnosis
- treat if becomes asymptomatic
- may benefit from bisphosphonates
Stage 1 / Normal X-ray, abnormal MRI
Forage: 80% G/E
Bisphosphonates
Stage 2 / Abnormal X-ray with cysts and sclerosis
A: As for Stage I
Pain & Stiffness
- often more pain than FT tears
Bursal side tears more painful than articular
Articular side more common
May see in young patient overhead throwing
Painful arc
Impingement signs
No weakness
- function good
Largest and most powerful rotator cuff
- arises coastal border of scapula
- superior 2/3 tendon inserts into LT
- inferior 1/3 inserts into proximal humerus
Action
- IR (with T major, P major, Lat Dorsi)
- part of force couplet depressing humeral head
Full thickness tear (FTT)
- variable amount retraction from insertion
Partial thickness tear (PTT)
- incomplete
- bursal or articular sided
Mid-substance calcification of the rotator cuff
- part of a metaplasia secondary to hypoxia


2 groups of patients
- stabilise patient with beanbag or lateral rests
- apply skin traction to forearm
- place traction pole at foot of table opposite surgeon
- suspend arm with 10 lb weight
- abduction 60°
- forward flexion of 20°
- tilt top shoulder posteriorly 30° so that glenoid is parallel wwith bed
- mark bony landmark
- prep & free drape
1. Removal Loose body
2. Excison of osteophytes
- coronoid
- olecranon
- aiming to improve ROM / prevent impingement