Anatomy
Action - internal rotation
Origin - coastal border of scapula
Insertion
- superior 2/3 tendon inserts into LT
- inferior 1/3 inserts into proximal humerus
Pathology
Isolated subscapularis tears
Anterosuperior cuff tears - supraspinatus + subscapularis
Medial subluxation of the biceps - subscapularis stabilizes long head of biceps in the groove
Yoon et al Biomedial Res Int 2018
- 100 patients with subscapularis tears on MRI
- half had medial biceps subluxation at arthroscopy
- 45/46 patients with medial biceps subluxation also had subscapularis tears
www.boneschool.com/medial-subluxation-biceps
Examination
| Subscapularis | |
|---|---|
|
Gerber lift-off test - internally rotate hand to back pocket - can lift hand away - need sufficient internal rotation to perform test |
Belly press test - fists on belly - elbows forward to eliminate deltoid - resist force lifting fists away from belly |
 |
 |
MRI
Patterns
- full thickness minimally retracted tears
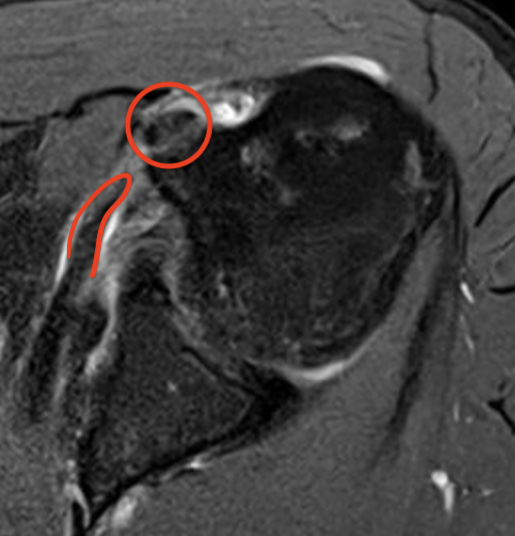
- full thickness retracted tears (comma sign)

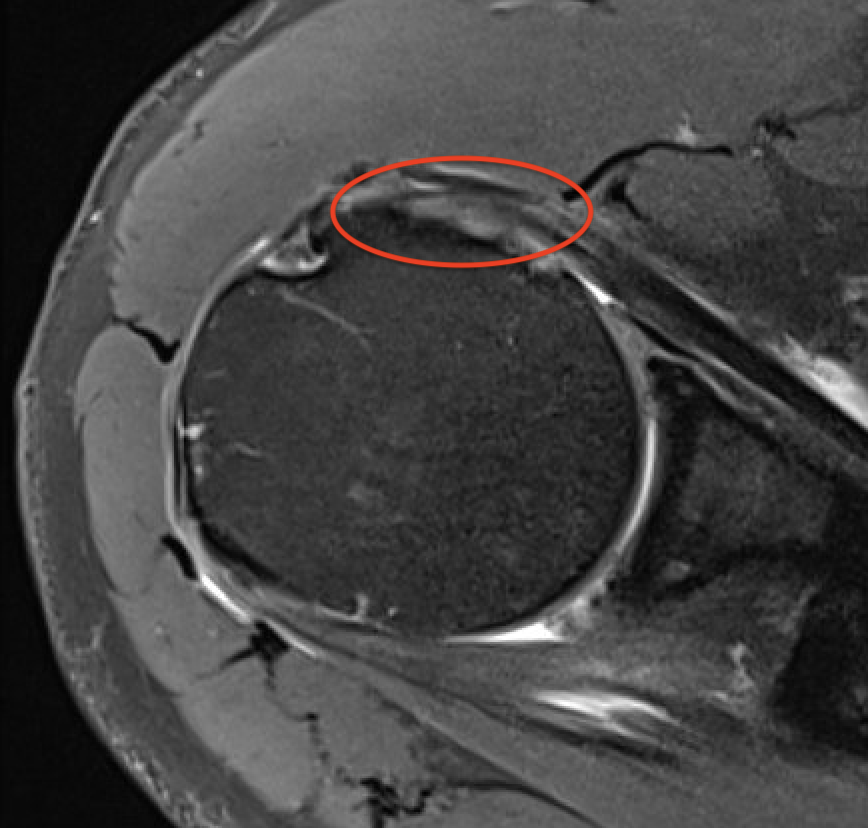
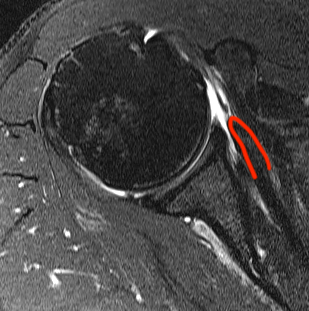
Perched long head of biceps with tear of upper border of subscapularis
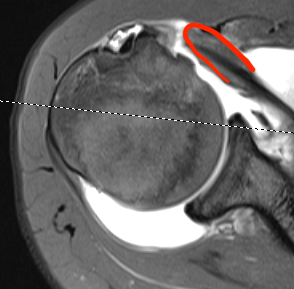
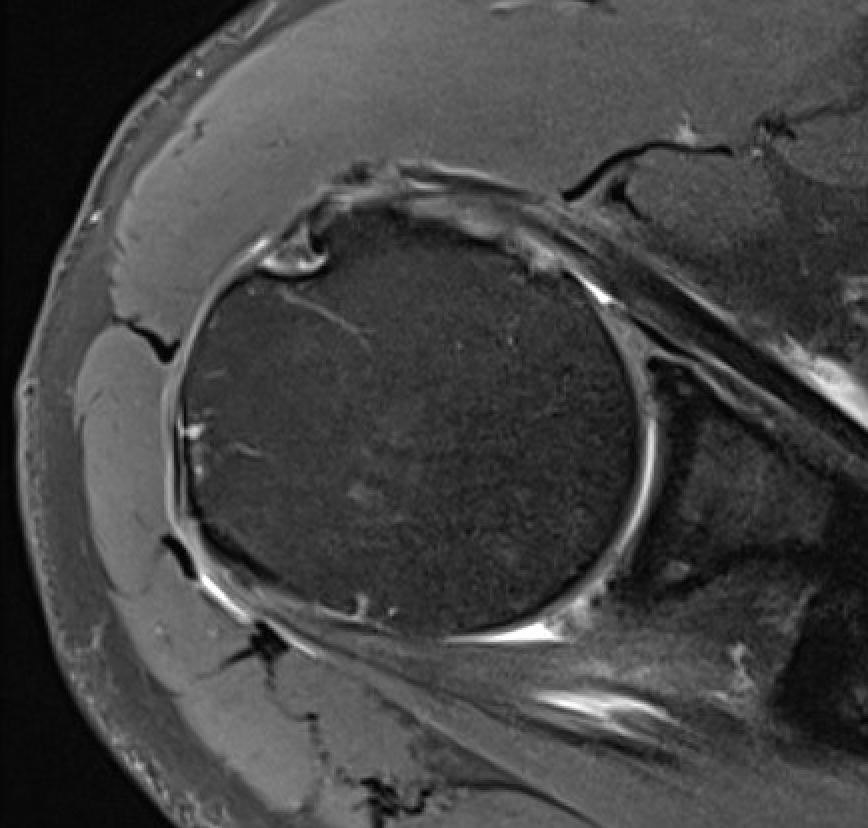
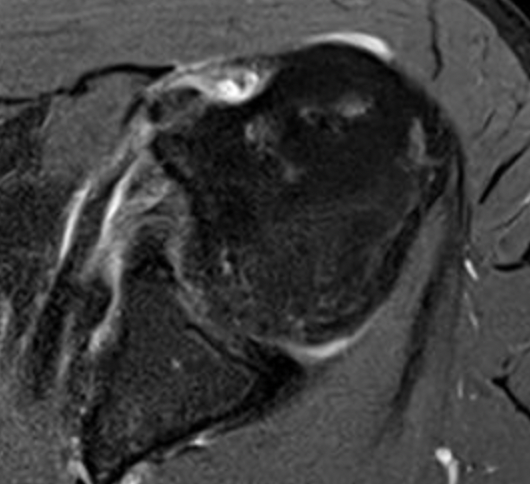
Full thickness minimally retracted subscapularis tear
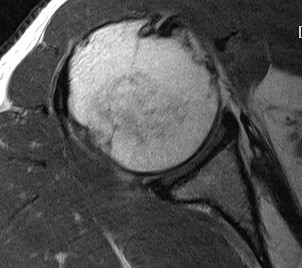
Full thickness retracted subscapularis tear
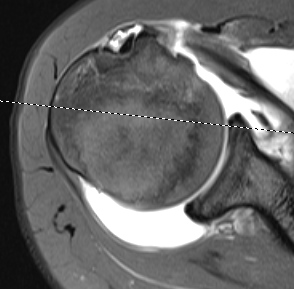
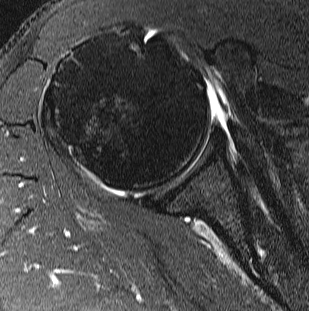
Full thickness retracted subscapularis tear with medial dislocation of long head of biceps tendon
Arthroscopy
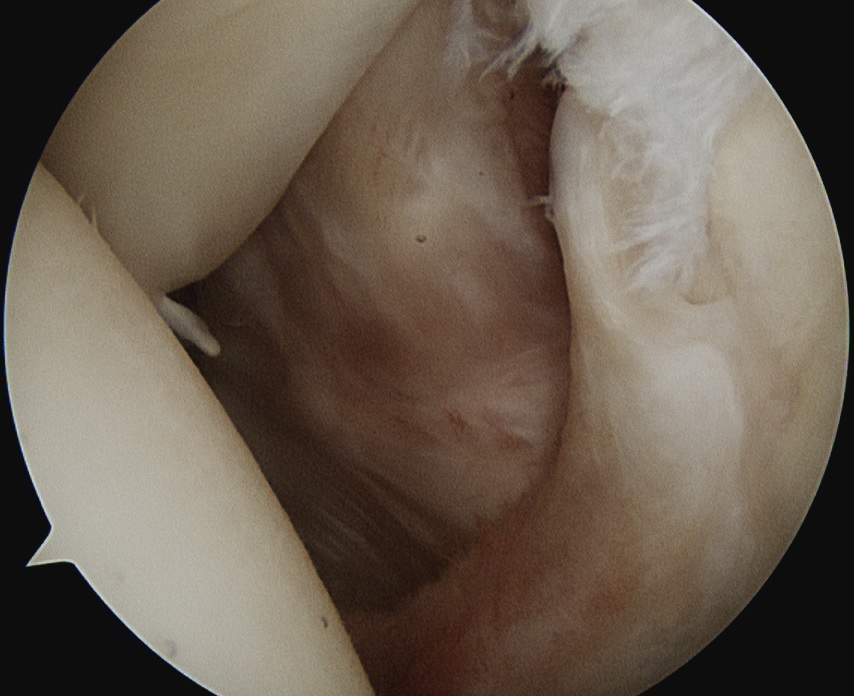
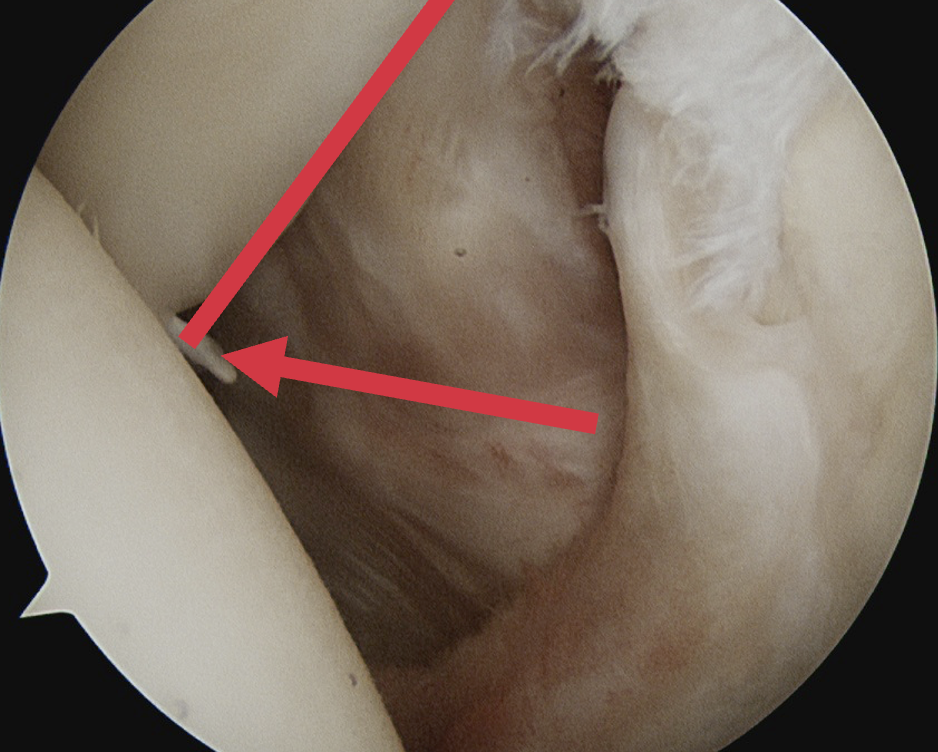
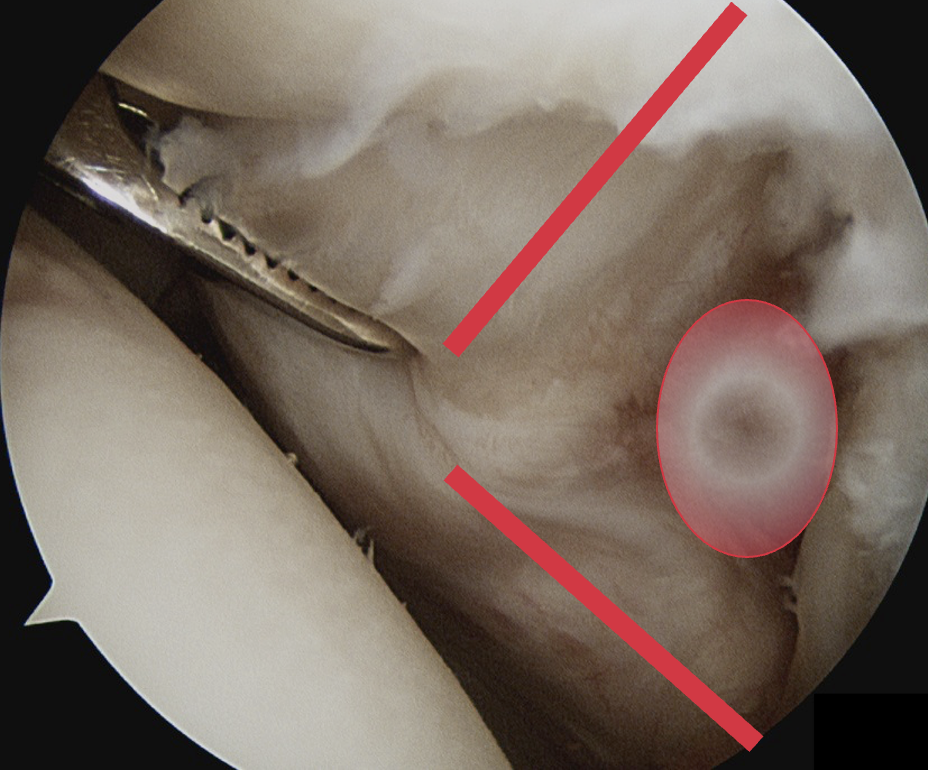
Hidden lesion
- assess subscapularis insertion thoroughly
- beware medial subluxation of the biceps
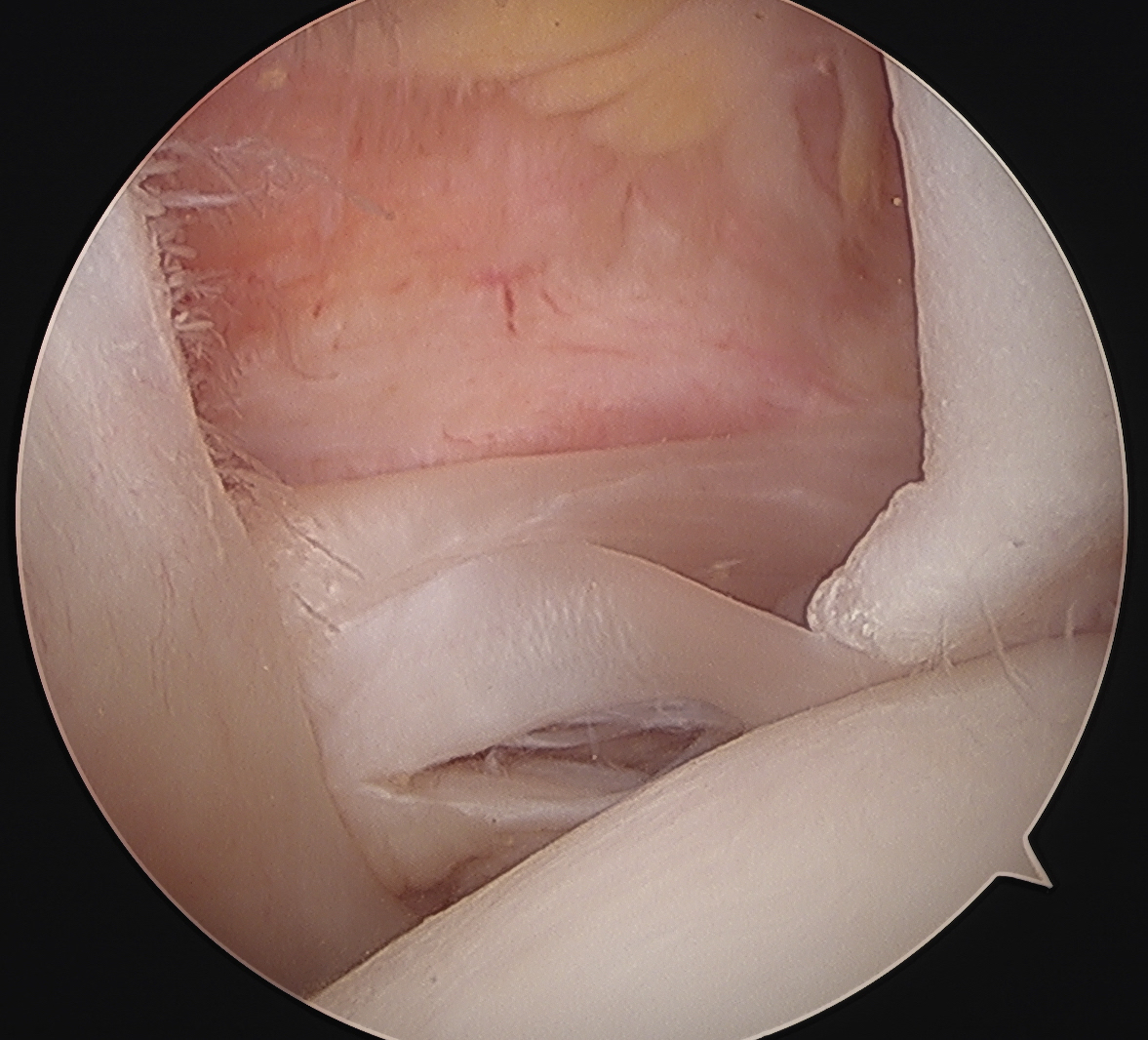
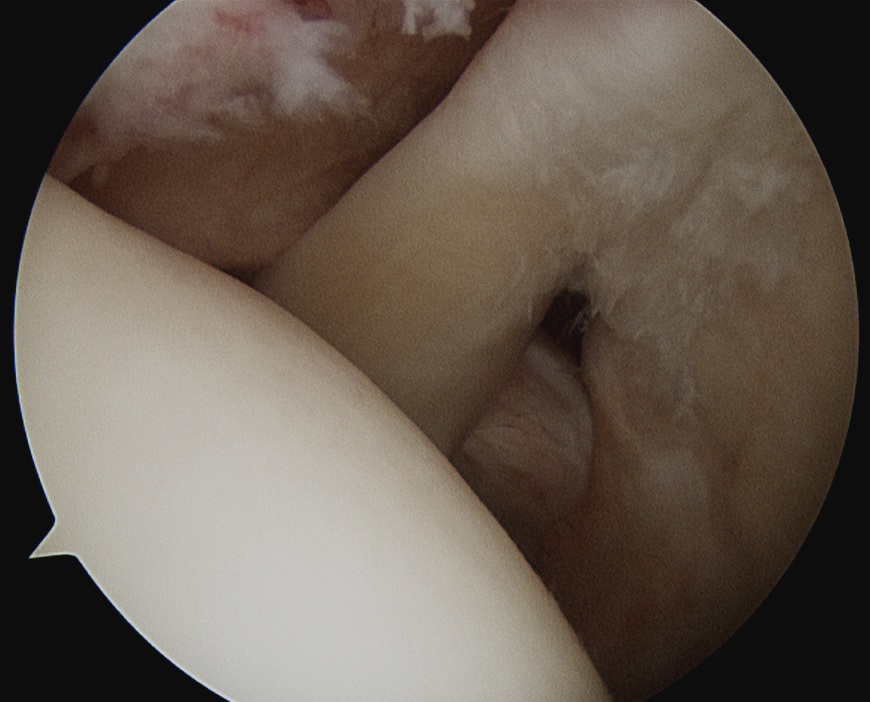
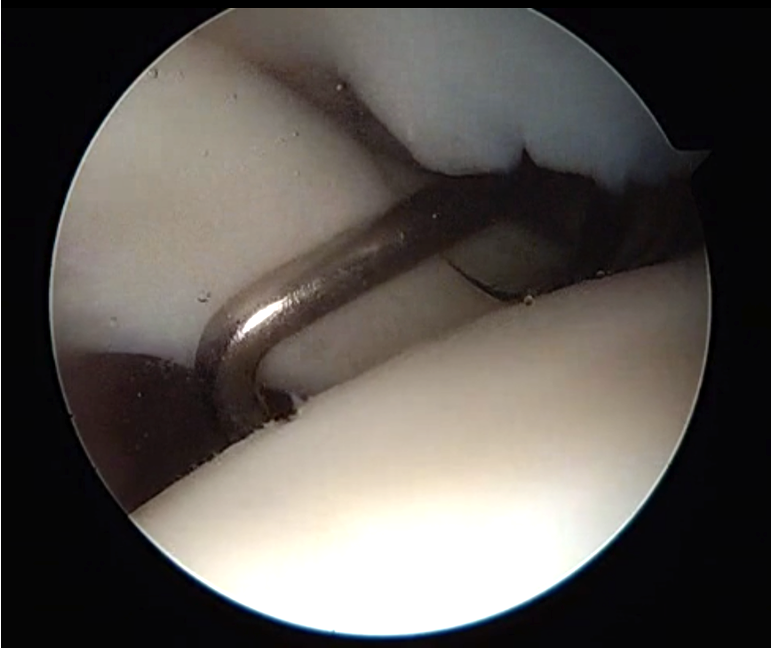
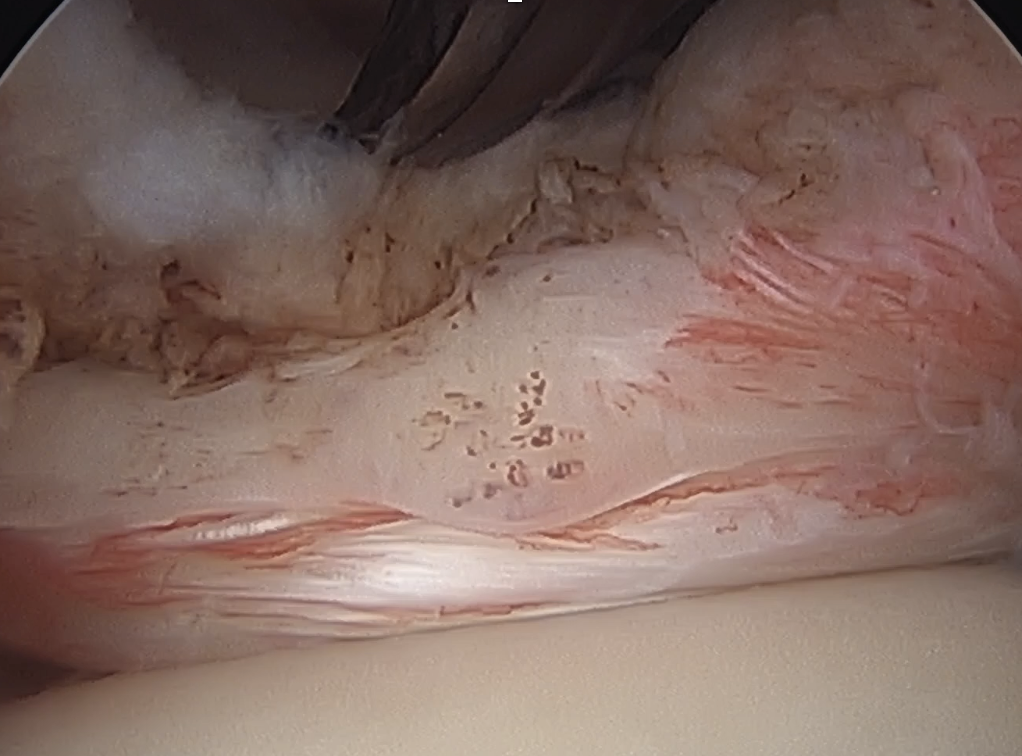
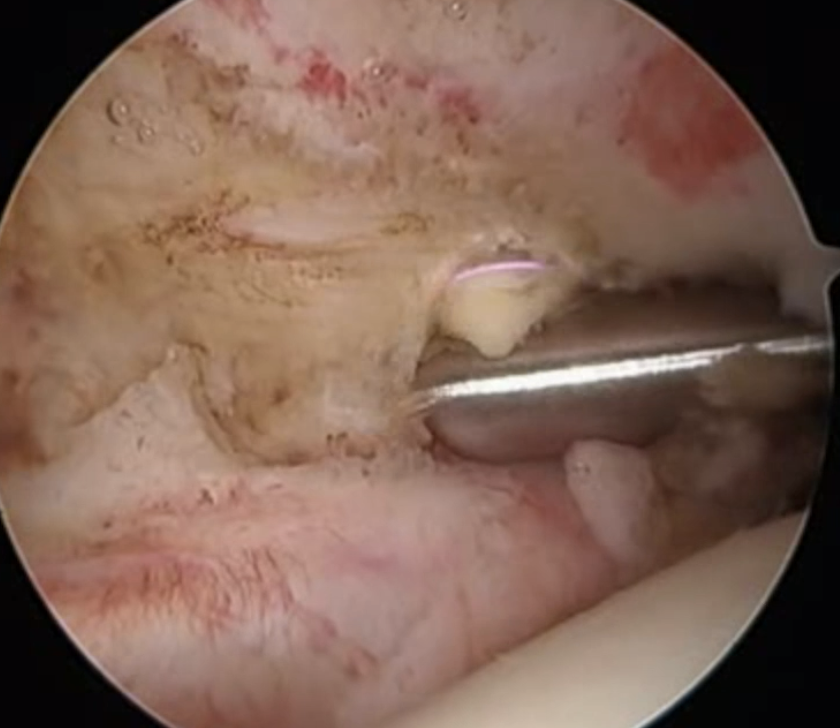
Medially dislocated biceps tendon with upper border subscapularis tear
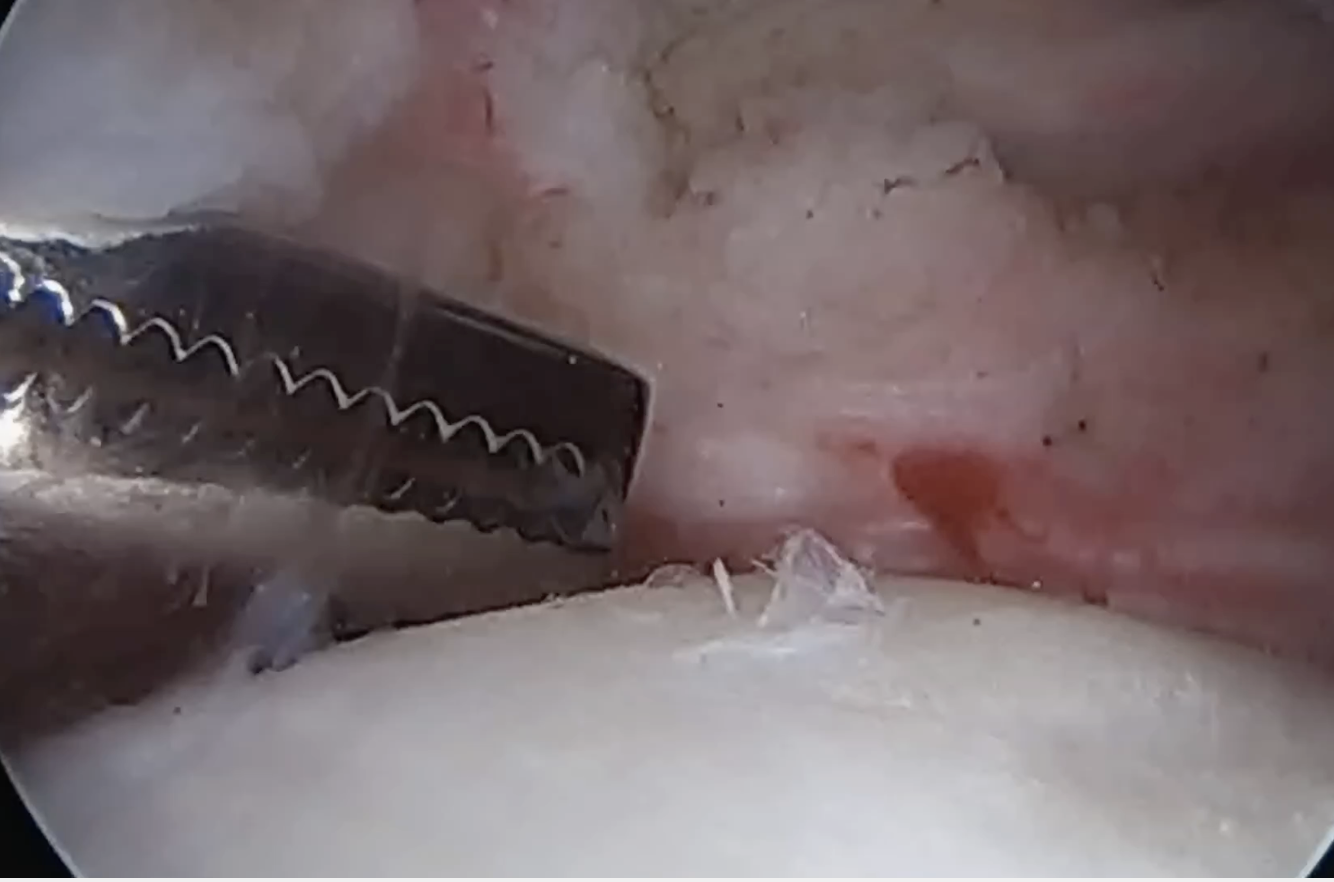

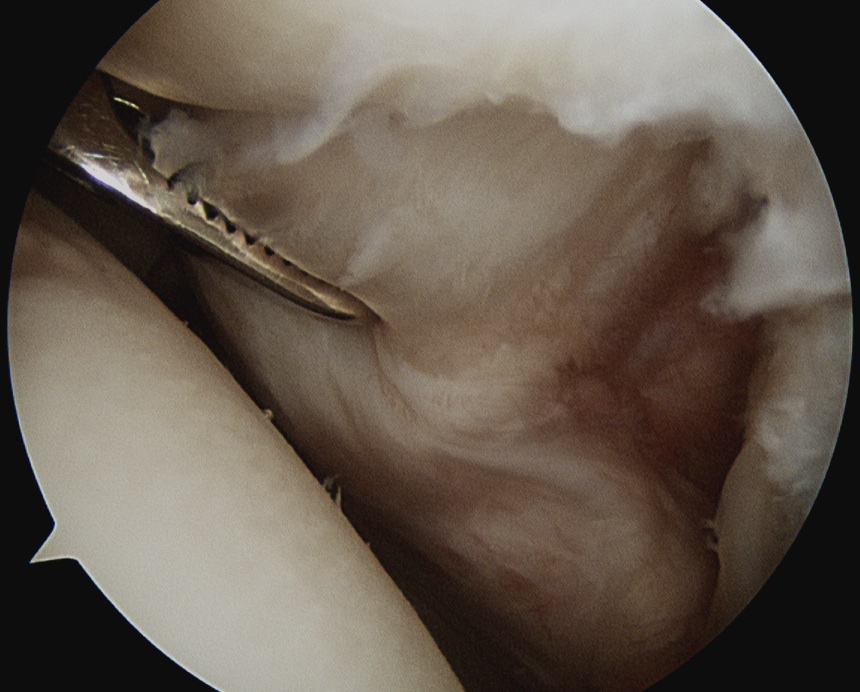
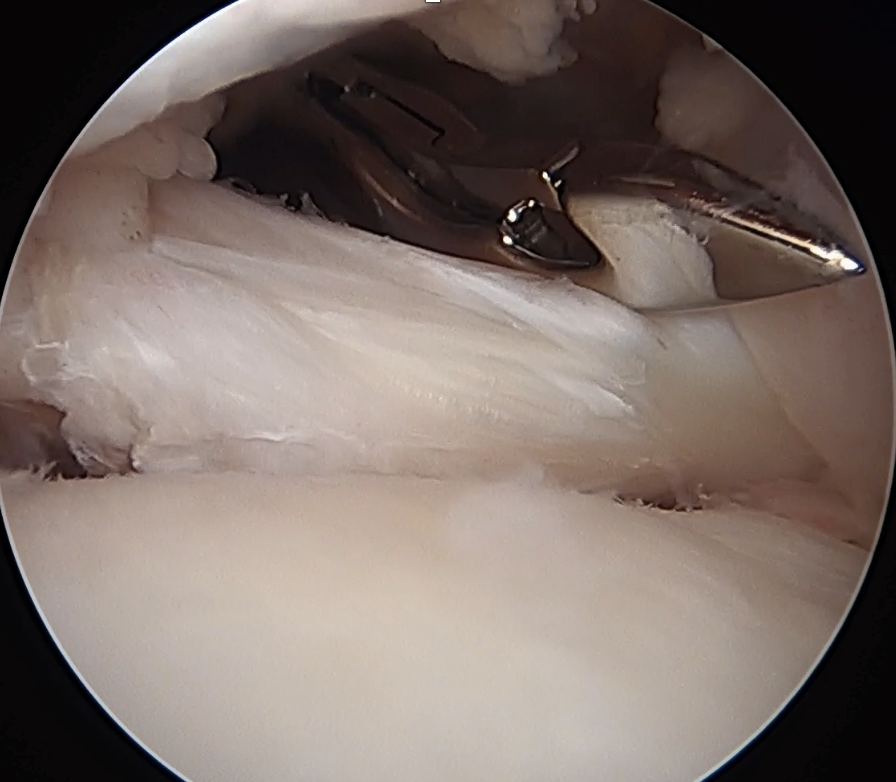
Full thickness tear of subscapularis off insertion revealed with grasper
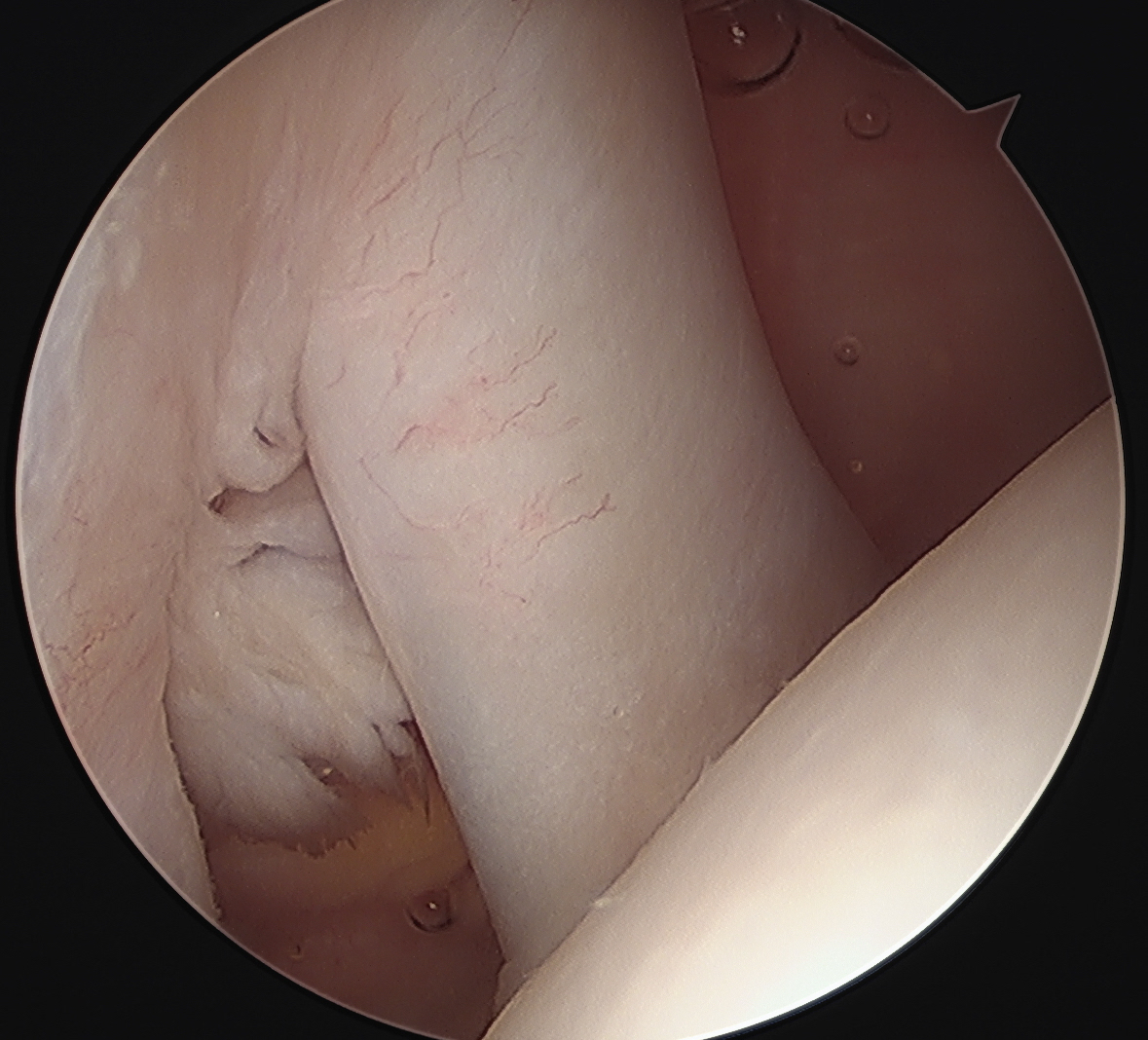
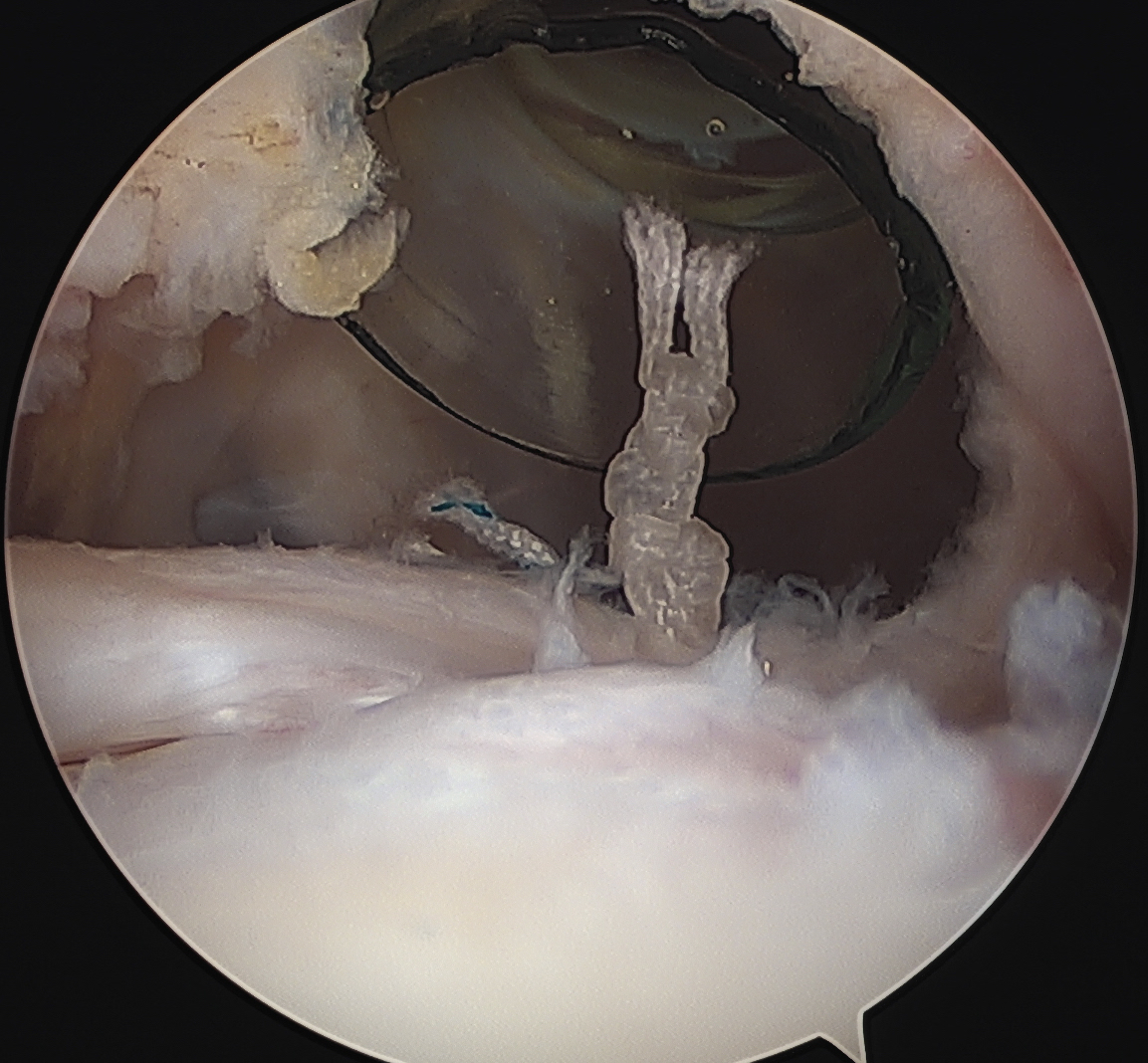
Comma Sign
Comma sign
- medially retracted subscapularis tear
- exposes the superior insertion of superior glenohumeral ligament / coracohumeral ligament
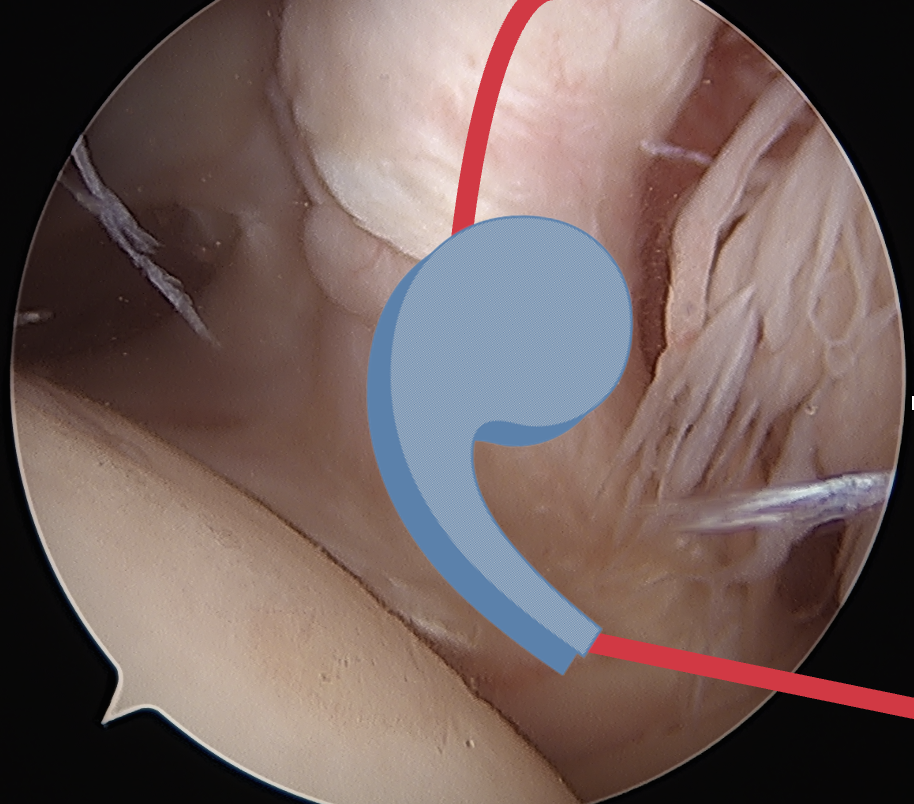
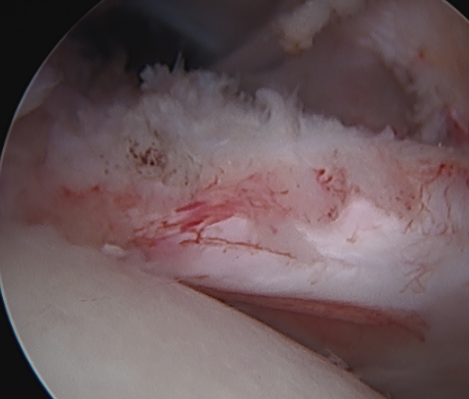
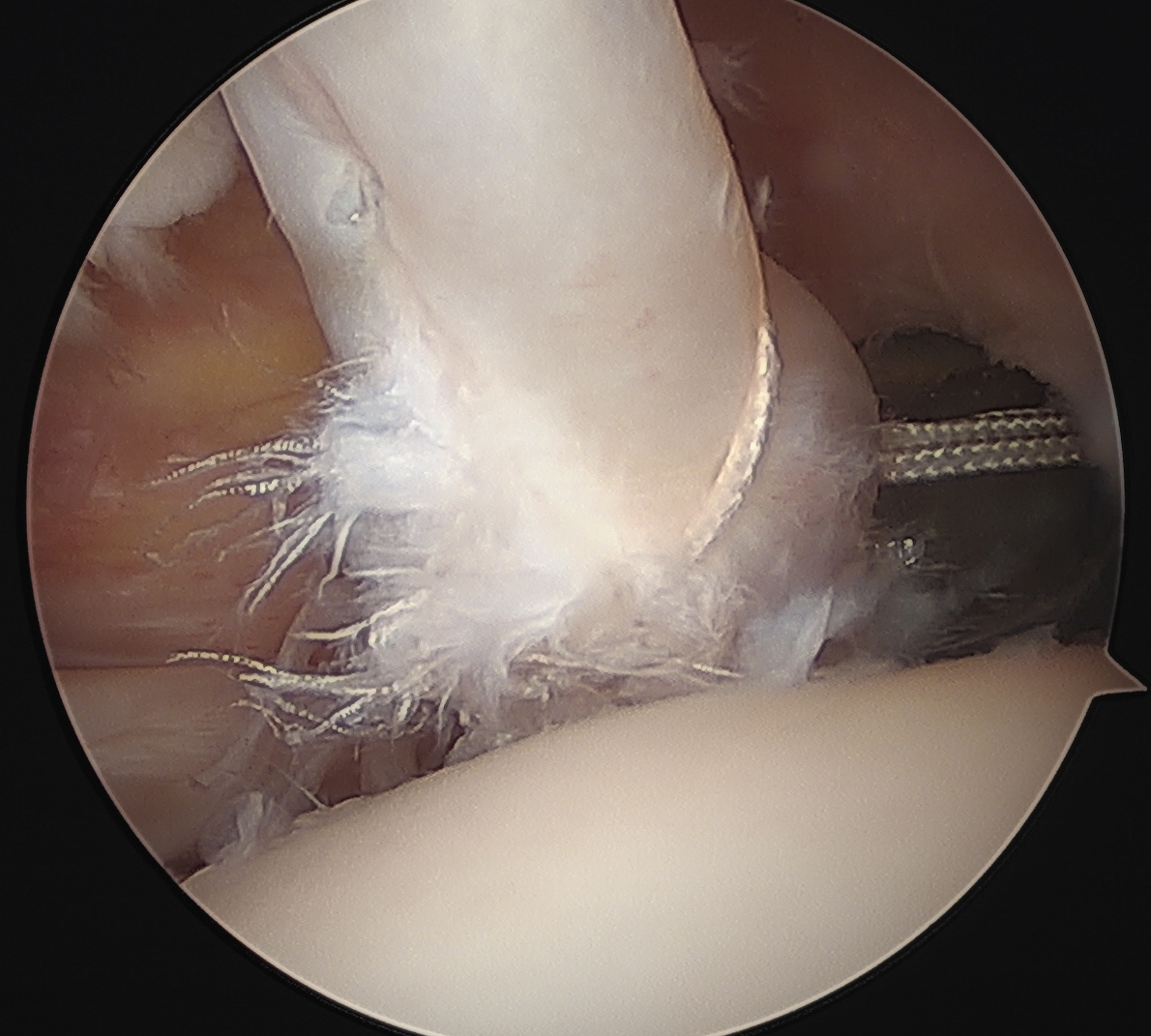
Full thickness retracted subscapularis tear with comma sign
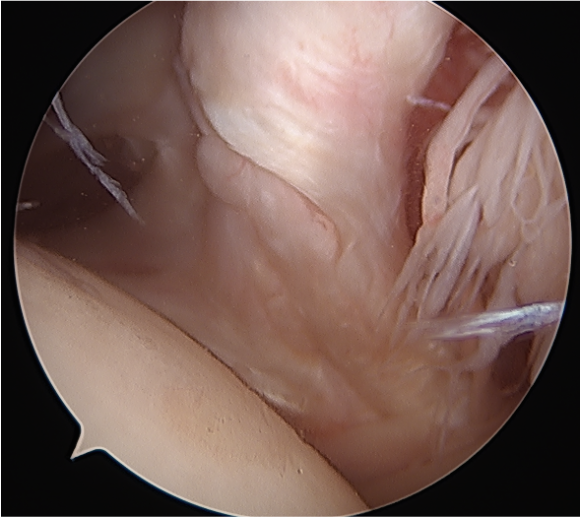
Full thickness completely retracted subscapularis, loss of rotator interval and comma sign
Full thickness completely retracted subscapularis, loss of rotator interval and comma sign
Operative Management
Options
Open repair versus arthroscopic
Arthroscopic repair - glenohumeral joint versus subacromial space
Results
Isolated subscapularis tears
Kamijo et al Arthros Sports Med 2022
- arthroscopic repair of 48 isolated subscapularis tears
- retear rates: small tears 6%, large tears 64%
Arthroscopic repair through glenohumeral joint
Vumedi arthroscopic subscapularis repair video
1. Minimally retracted subscapularis tear
- anterior rotator cuff portal for footprint debridement and anchor insertion
- anterolateral portal / portal of Wilmington for biceps / suture passage
- tag biceps for later tenodesis
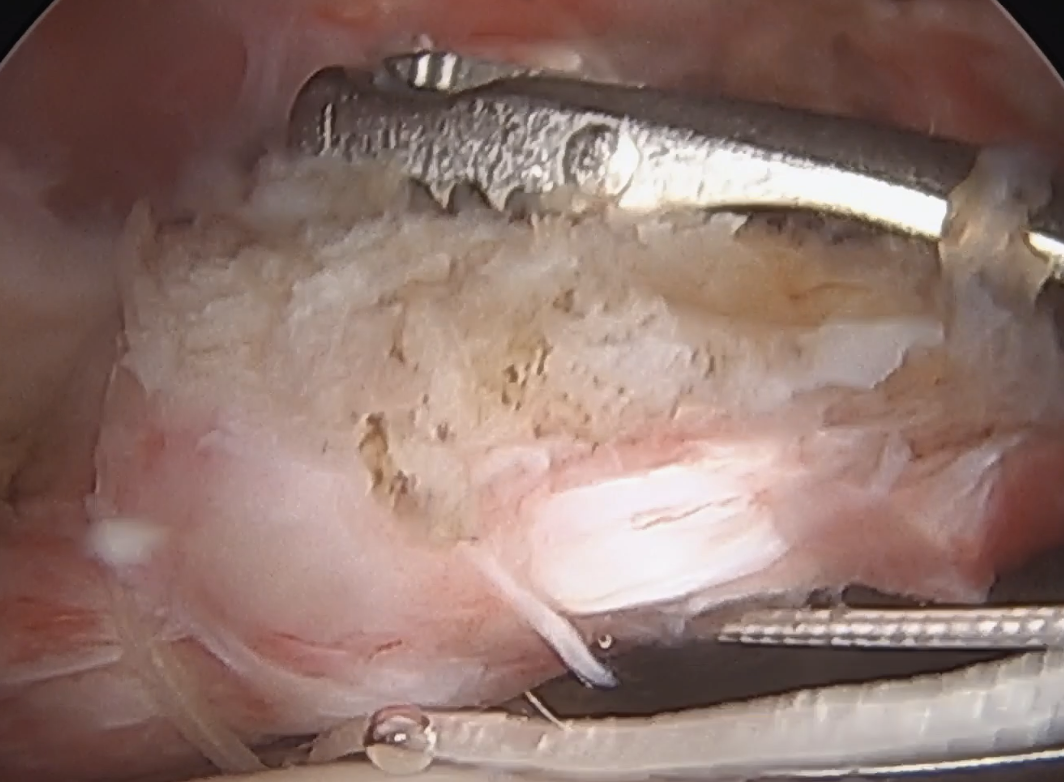
- debride footprint on lesser tuberosity
- insert anchor through anterior portal
- pass sutures from anterolateral portal with birdsbeak or from lateral portal with suture passer
- tie from anterior portal
- +/- lateral row / double row repair

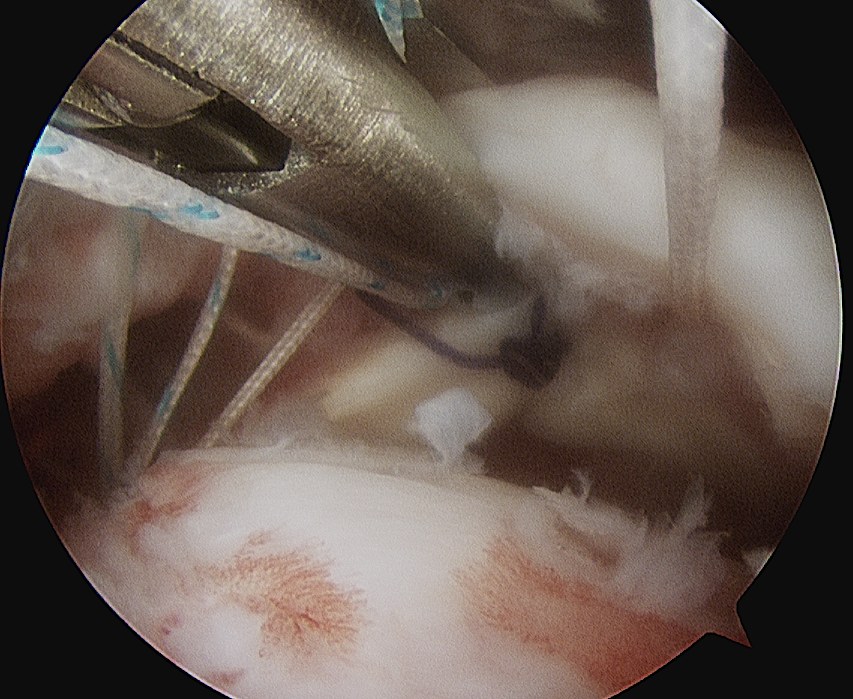
Anterolateral portal of Wilminton at anterolateral border of the acromion used to tag and release biceps
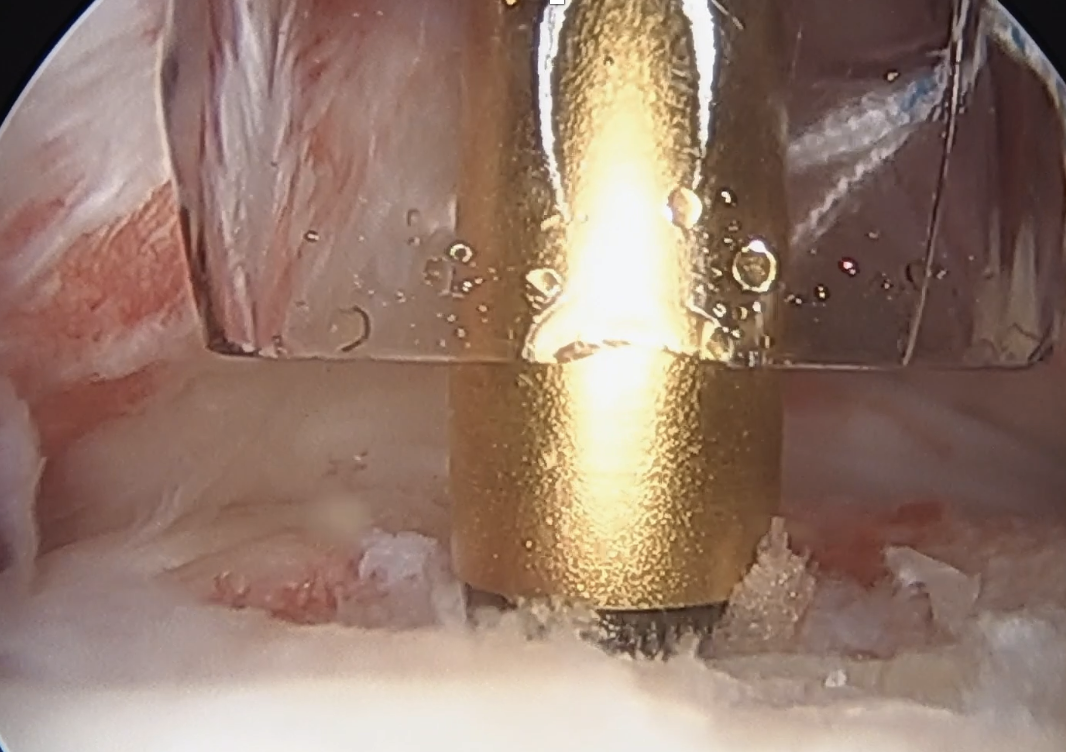
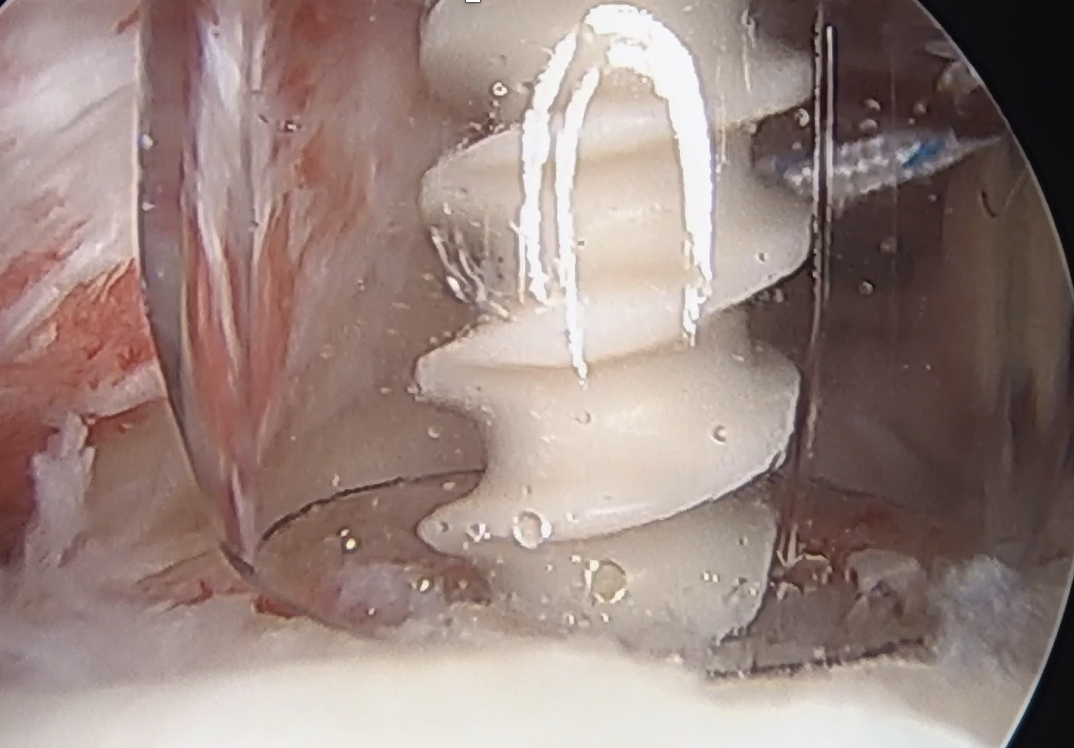
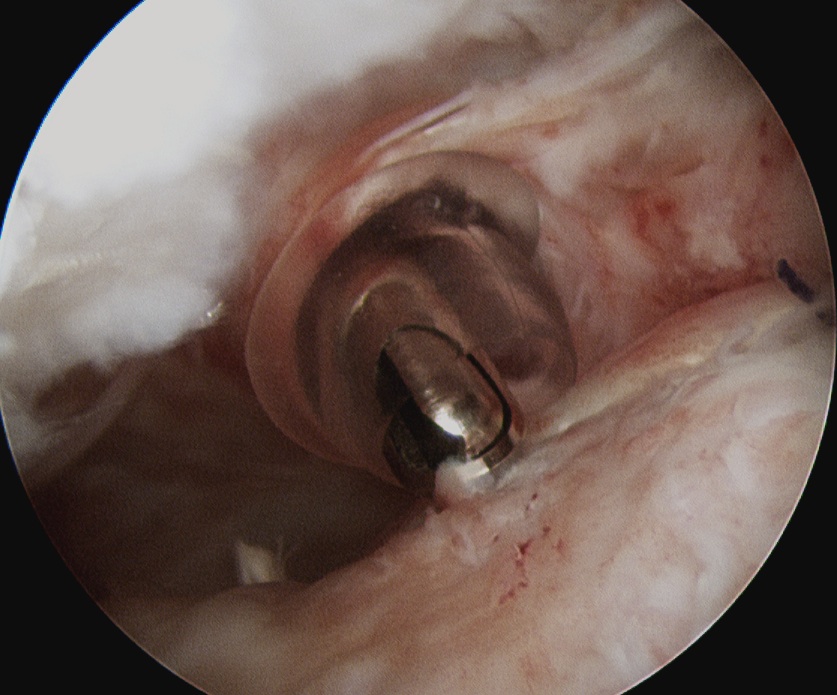
Insert anchor through anterior portal into subscapularis footprint
Suture passage through anterior portal or anterolateral portal and tie sutures through anterior portal
2. Retracted tendon tear
- tag and release biceps tendon
- lateral traction sutures in subscapularis
- extensive tendon release with cautery and recreate rotator interval
- repair as above
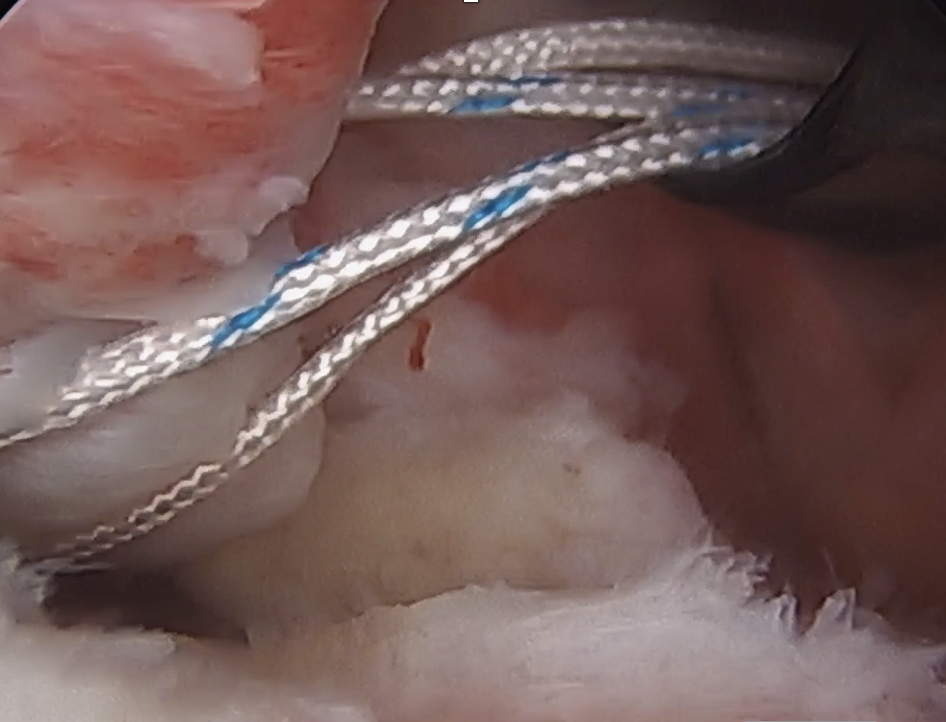
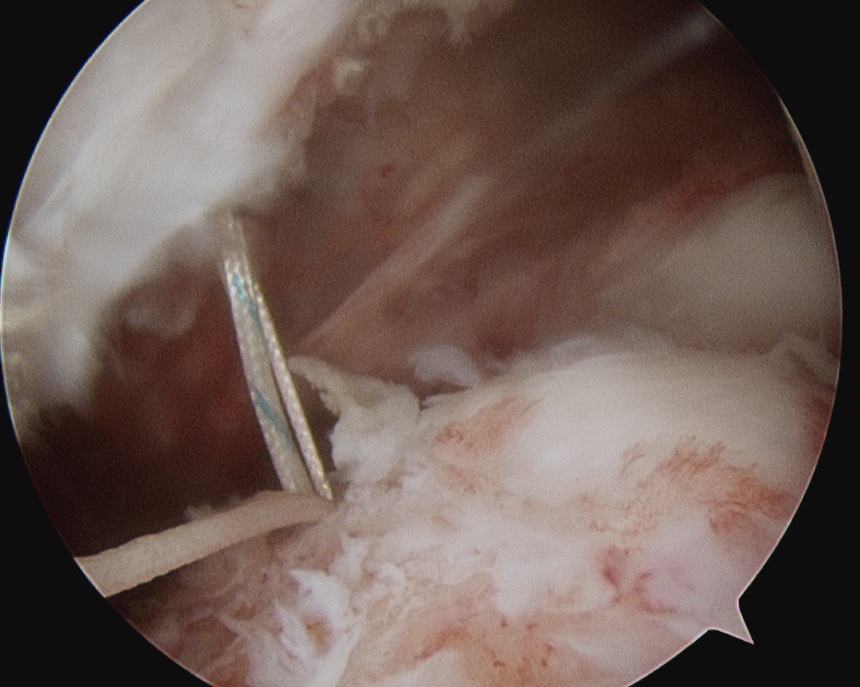
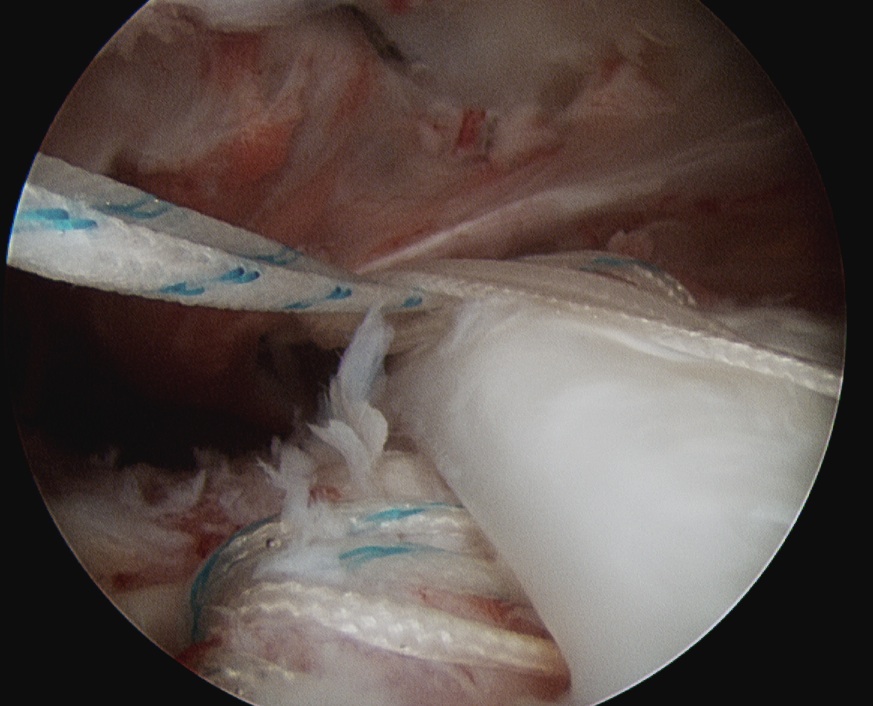
Lateral traction sutures placed in subscapularis, then cautery used to remove scar tissue and recreate rotator interval
Arthroscopic repair through subacromial space
Technique
- move camera to lateral portal for subscapularis visualization
- can use 70 degree scope
- anterior portal for debridement of footprint and insertion of anchor
- anterolateral portal for suture passage through subscapularis tendon
Open subscapularis repair
Technique
Deltopectoral approach
- preserve axillary nerve inferiorly
- mobilise SSC
- subscapular nerves on anterior surface medial to glenoid rim
- tenodesis LHB
- suture anchor repair to lesser tuberosity
Irreparable subscapularis tears
Options
Elderly - rTSA
Young patients
- Pectoralis major transfer
- Latissimus dorsi tendon transfer (LDTT)
- anterior capsular reconstruction
Technique
Video J Sports Med pectoralis major transfer
Arthroscopy techniques LDTT for subscapularis deficiency
Open technique of LDTT for subscapularis deficiency
Results
- systematic review of LDTT v pectoralis major transfer for irreparable subscapularis
- 12 studies and 260 patients
- suggest better outcomes for LDTT