Definition
Full thickness tear (FTT) - complete tendon tear / avulsion from foot print
Partial thickness tear (PTT) - partial thickness tendon tears / bursal or articular sided
Epidemiology
95% atraumatic / degenerative
Incidence
- systematic review of incidence RC pathology
- 30 - 49: 13%
- 50 - 59: 19%
- 60 - 69: 30%
- 70 - 79: 41%
- > 80: 62%
Bilateral
- patients > 65 with painful full thickness cuff tear
- 50% chance of unilateral asymptomatic cuff tear
Natural history of rotator cuff tears
- 118 full thickness rotator cuff tears
- 61% enlarged over a 3 year period
- systematic review of progression
- partial tears: 27% at 2 years
- full thickness tears: 55% at 2 years
Anatomy
Blood Supply
Proximal from muscle belly / Distal from bone
Vessels more abundant on bursal side than articular side
Foot print
Supraspinatus: mean 13 mm anterior to posterior
Infraspinatus: 32 mm curving superiorly
Pathology
- MRI of 245 patients with RC tears
- mean size 11 x 11 mm
- most located 10 mm posterior to long head of biceps
History
Pain and weakness
Examination
Muscle wasting of supraspinatus and infraspinatus


Rotator cuff strength
| Supraspinatus | Infraspinatus |
|---|---|
|
Patient's arm forward flexed 90° Thumb down |
Resist external rotation |
 |
 |
| Subscapularis | |
|---|---|
|
Gerber lift-off test - internally rotate hand to back pocket - can lift hand away - need sufficient internal rotation to perform test |
Belly press test - fists on belly - elbows forward to eliminate deltoid - resist force lifting fists away from belly |
 |
 |
Pseudoparalysis / Shoulder hiking

Xray
Look for: acromial morphology / high riding humeral head / rotator cuff arthropathy

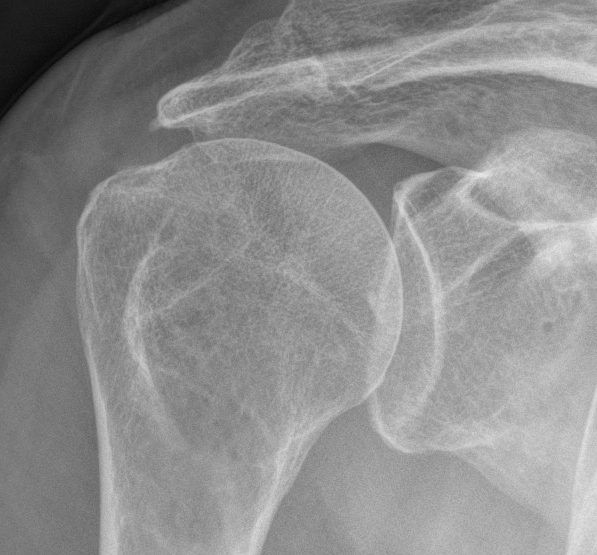

Acromial spur / superior migration humeral head / rotator cuff arthropathy
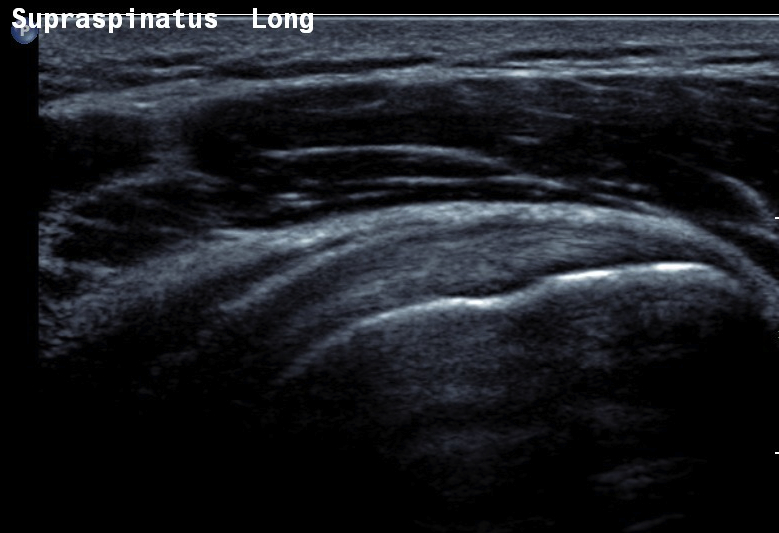
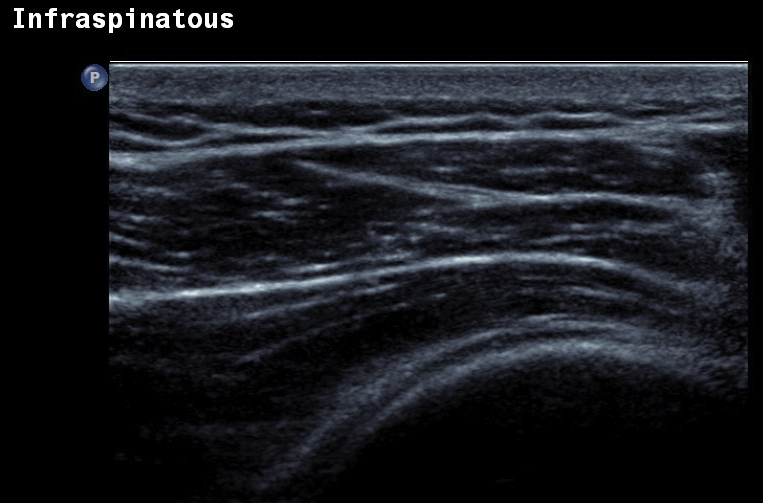
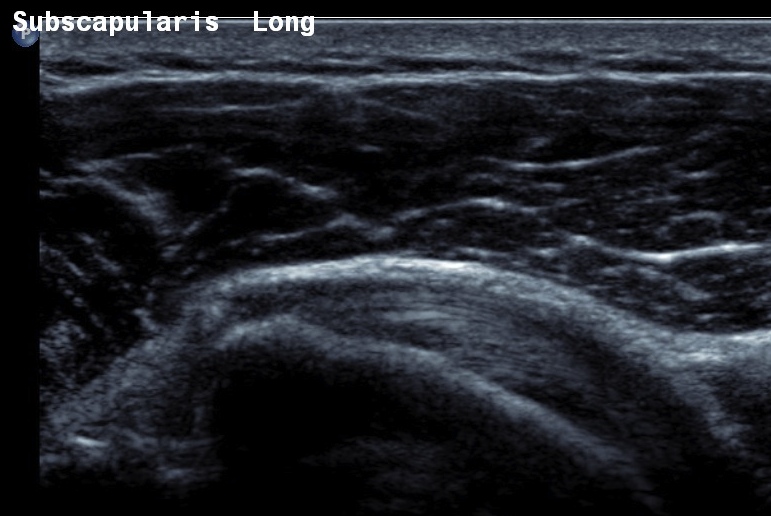
Ultrasound
Normal
- systematic review of US rotator cuff tears
- US more accurate for supraspinatus and biceps than subscapularis
- US more accurate for full thickness tears than partial thickness tears
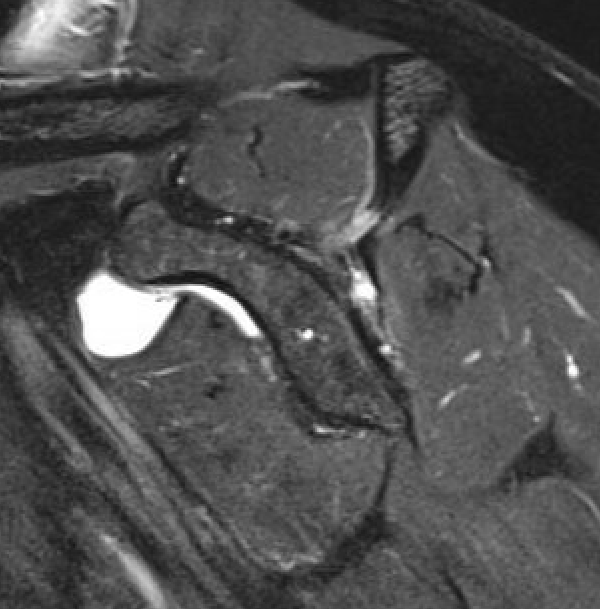
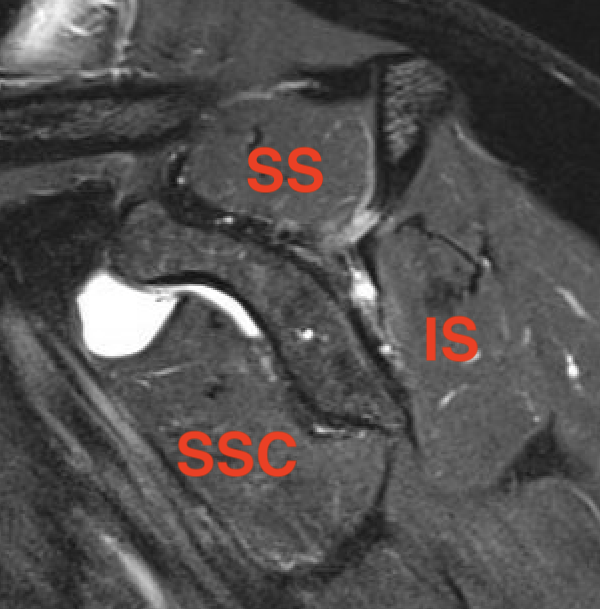
MRI
Look for
- supraspinatus / infraspinatus / subscapularis / long head of biceps pathology
- partial verus full thickness
- size of tear in coronal and sagittal planes
- retraction
- atrophy / fatty infiltration

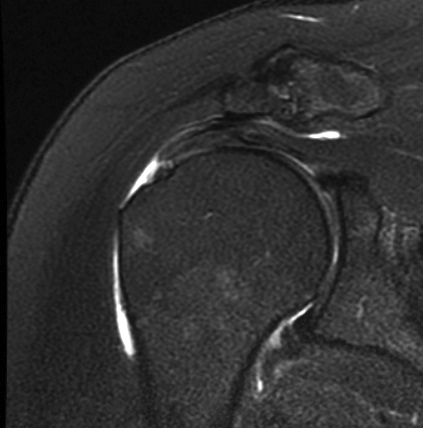
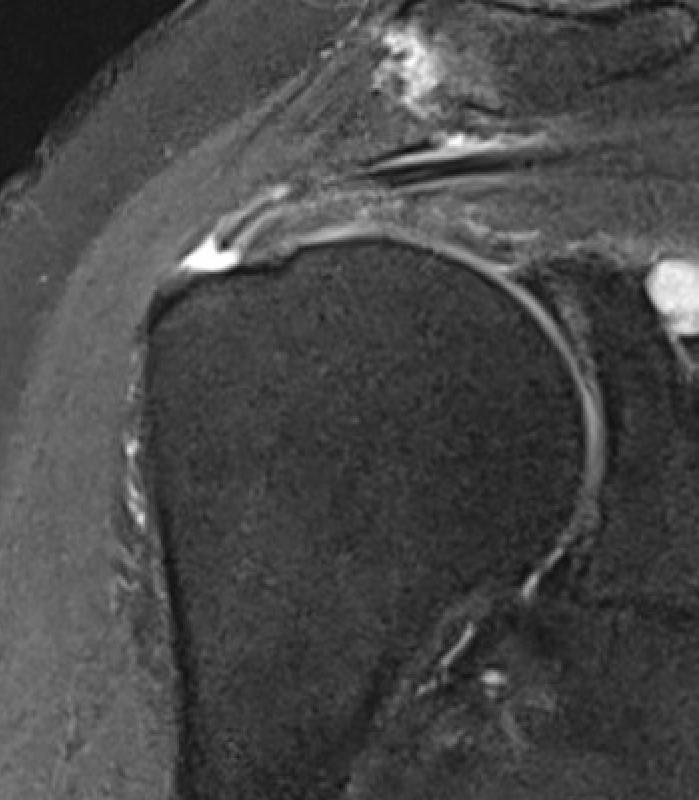
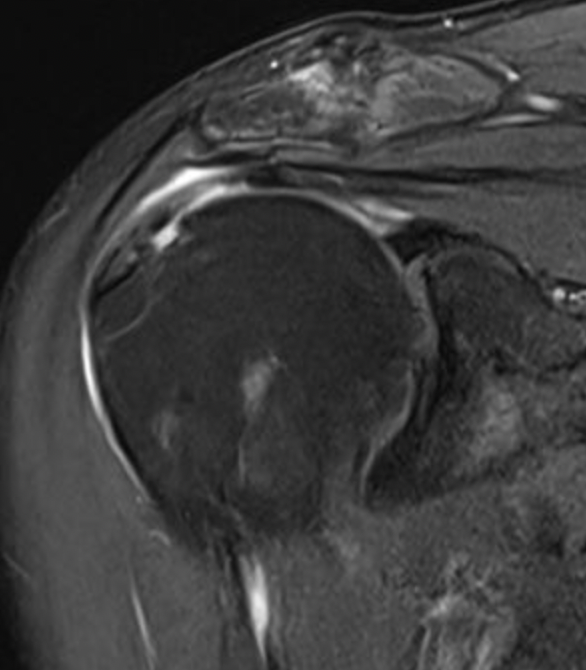
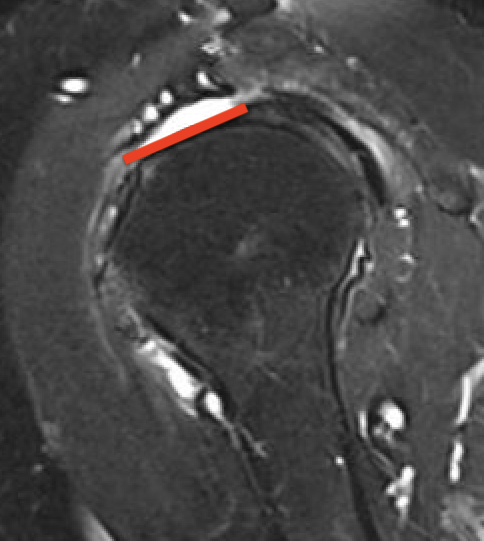
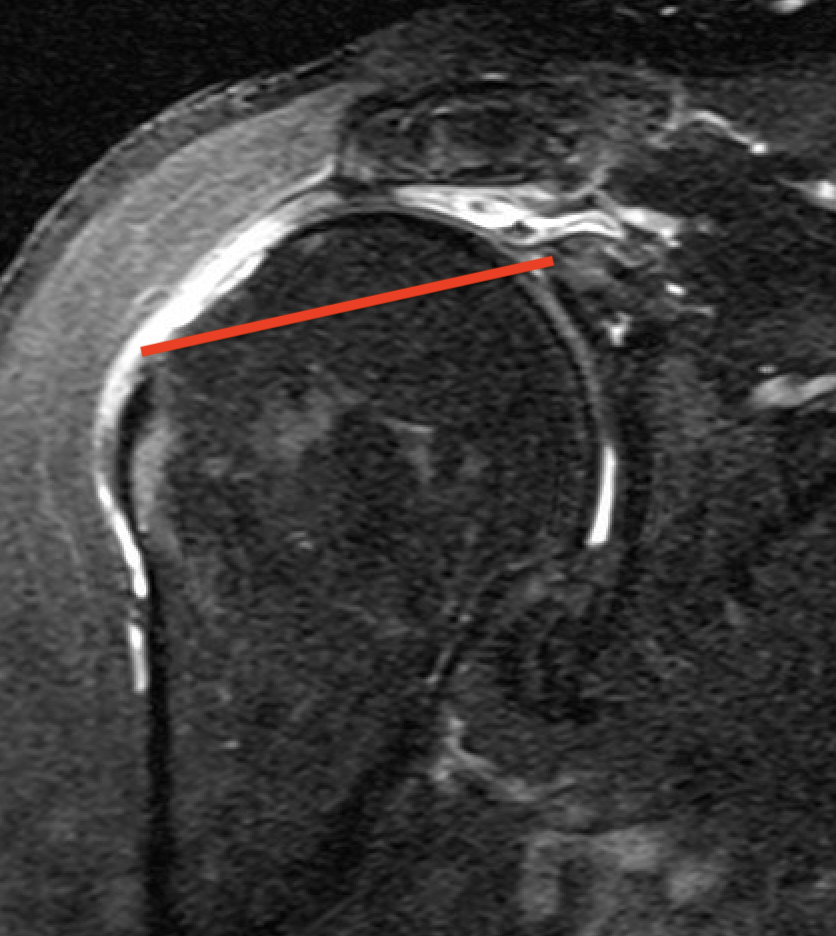
Full thickness rotator cuff tears
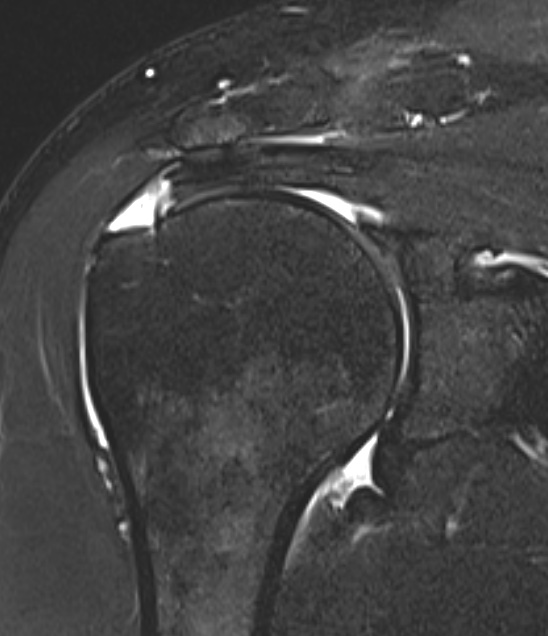
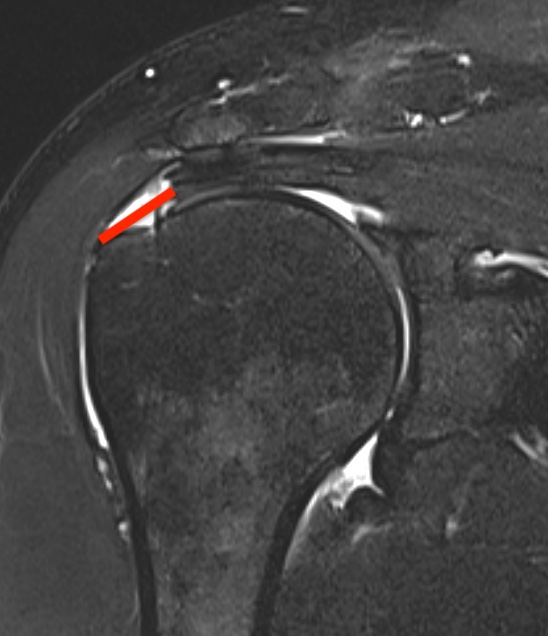
Partial bursal sided tear Partial articular sided tears
Subscapularis tears
Classification
| Size | Tendons | Topography | Patte Retraction on coronal MRI |
|---|---|---|---|
|
Small < 1 cm Moderate 1-3 cm Large 3-5 cm Massive > 5 cm |
Supraspinatus Infraspinatus Subscapularis |
Superior - supraspinatus Anterosuperior - supraspinatus / subscapularis Posterosuperior - supraspinatus / infraspinatus |
I: To footprint II: Articular surface / midhumeral head III: To or beyond glenoid |
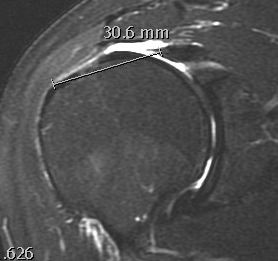
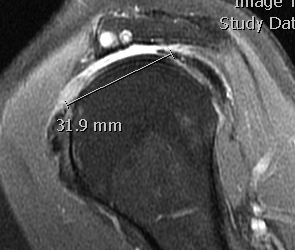
Measure tear in the coronal and sagittal plane
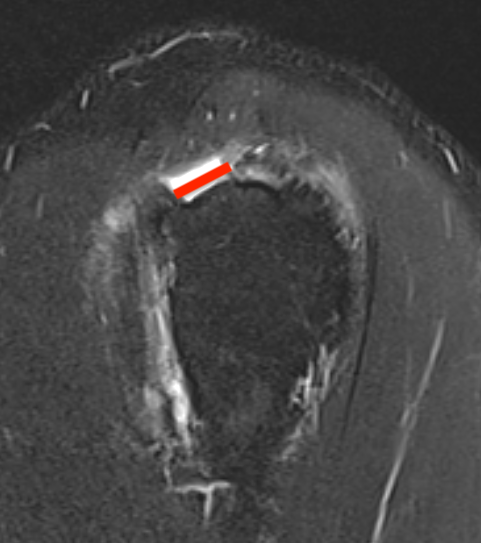
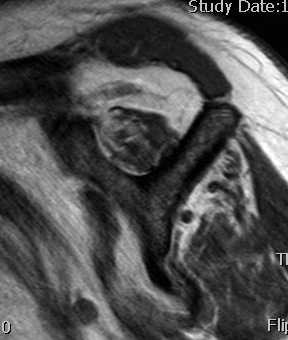
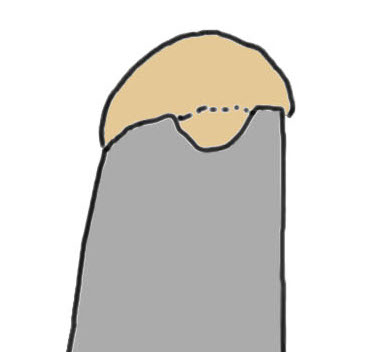
Small full thickness rotator cuff tear of supraspinatus - retracted to footprint
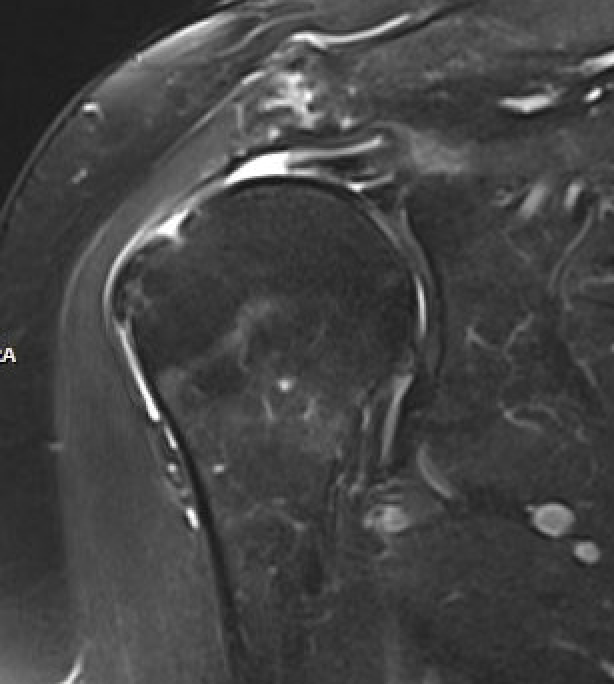
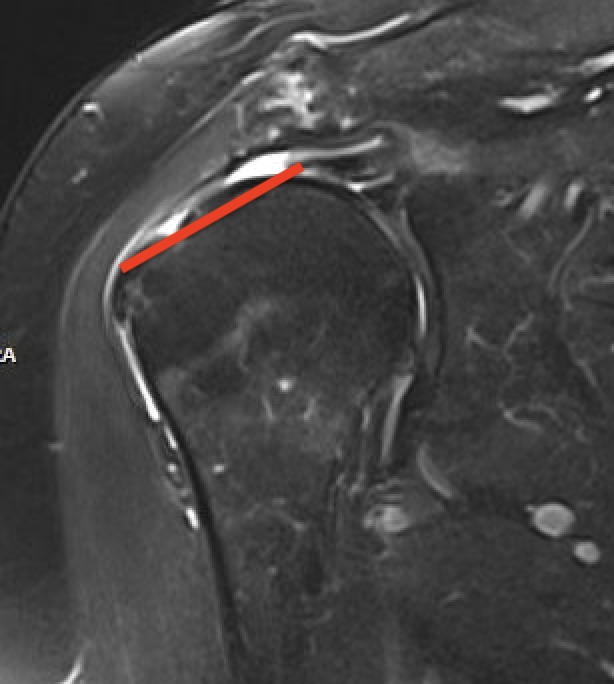
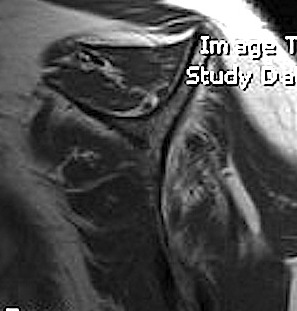
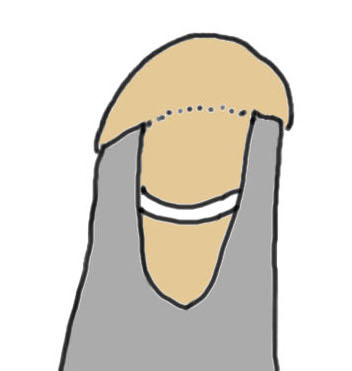
Large full thickness tear of supraspinatus and infraspinatus tendon - retracted to midhumeral head

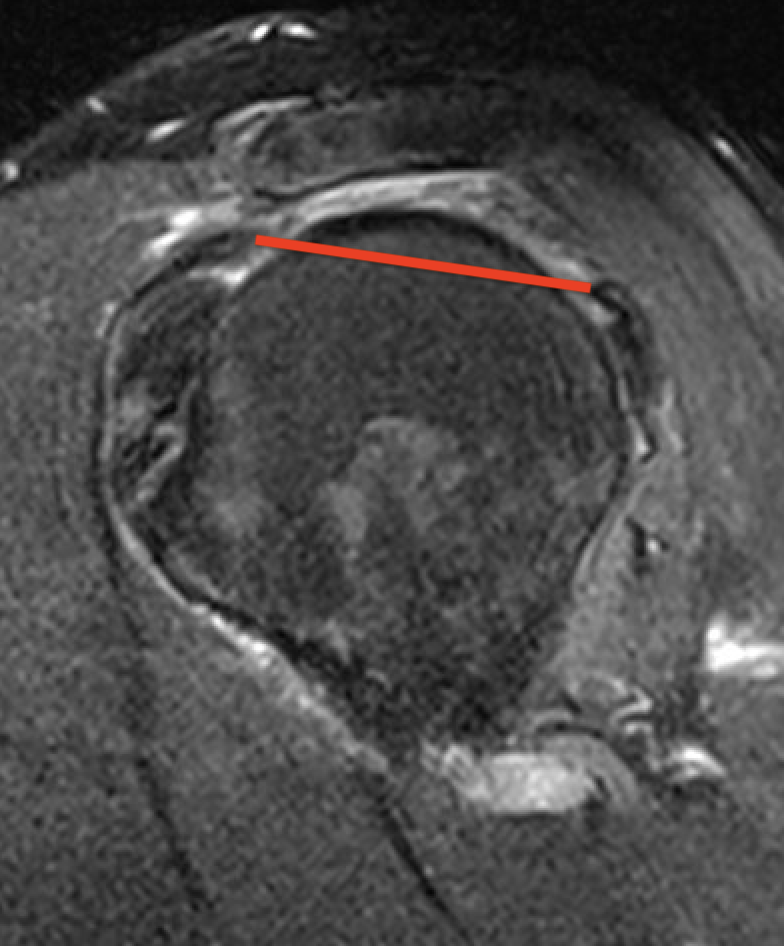
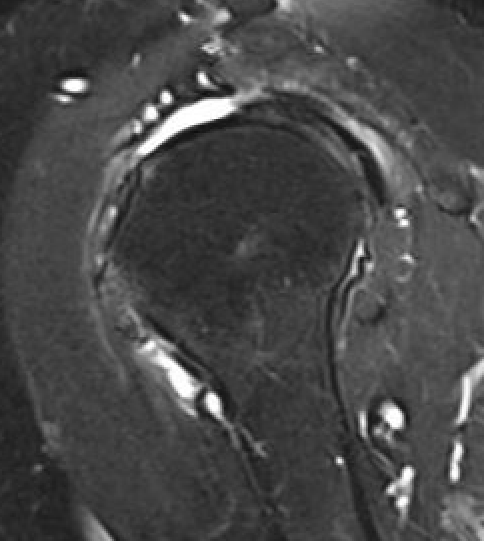
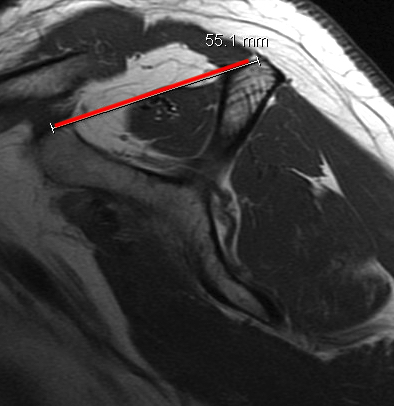
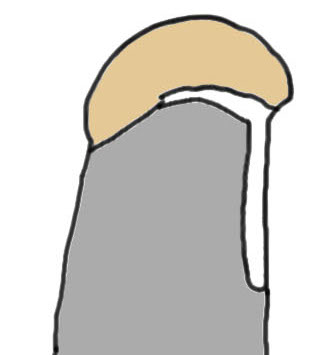
Massive rotator cuff tear of the supraspinatus and infraspinatus tendon - retracted to glenoid
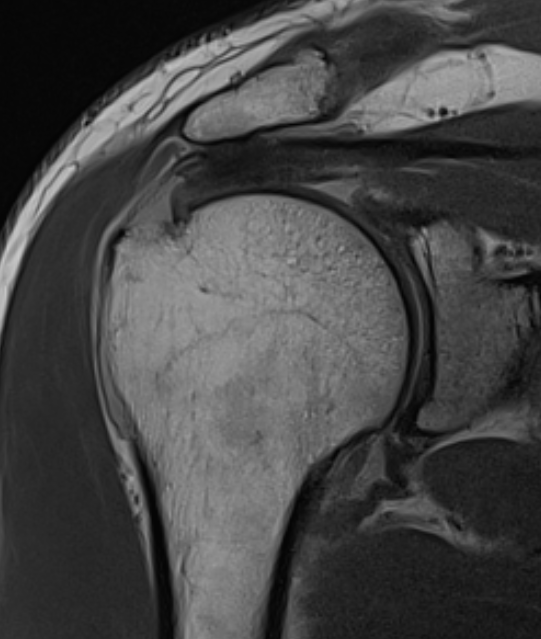
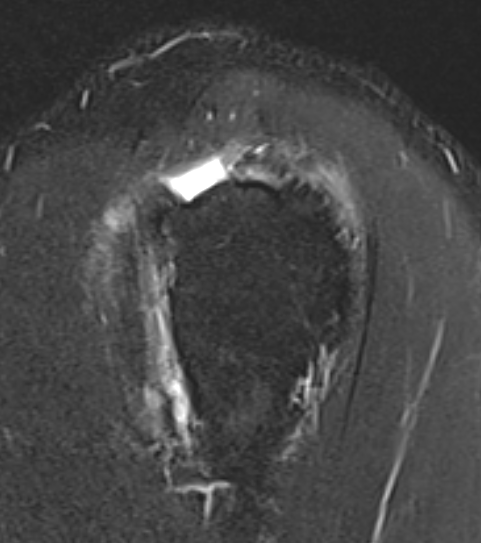
Goutallier classification
Amount of fatty degeneration in rotator cuff muscle belly on a T1 sagittal MRI
- systematic review of Goutallier grade and retear rates
- retear rates after surgical repair increase as the Goutallier stage increases
Stage 0: normal muscle
| Stage 1 | Stage 2 |
|---|---|
|
Some fatty streaks MRI shows some fatty streaks in supraspinatus |
More muscle than fat MRI shows grade 2 in supraspinatus |
 |
 |
| Stage 3 | Stage 4 |
|---|---|
|
Equal fat and muscle MRI demonstrates grade 3 supraspinatus and infraspinatus |
More fat than muscle MRI demonstrates grade 4 infraspinatus |
 |
 |
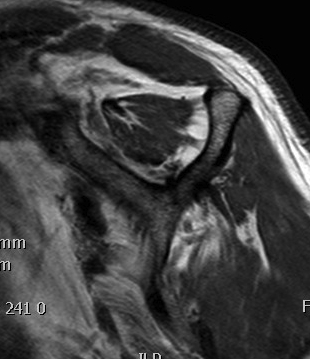
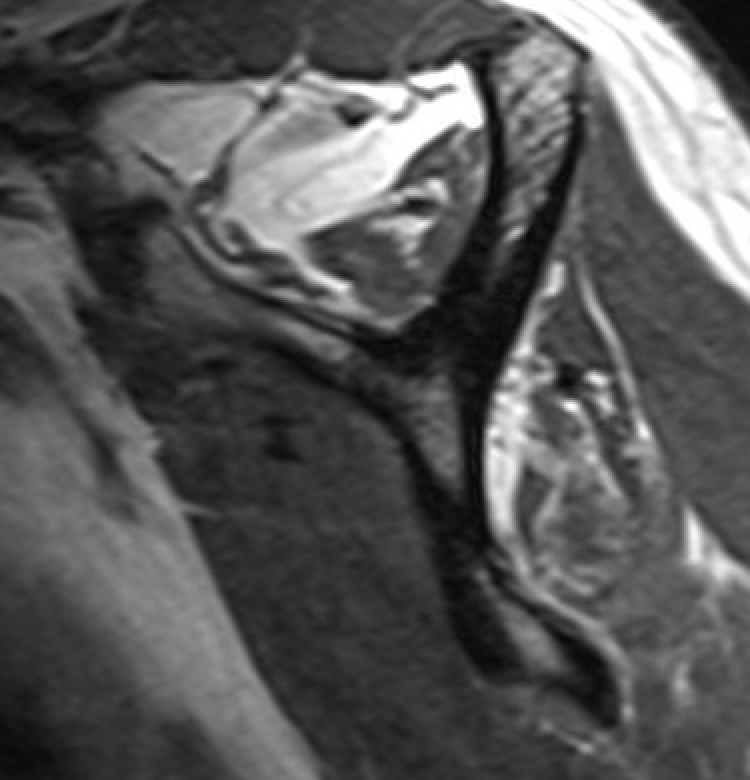
Supraspinatus atrophy
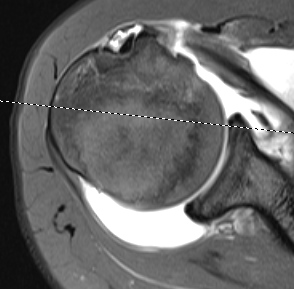
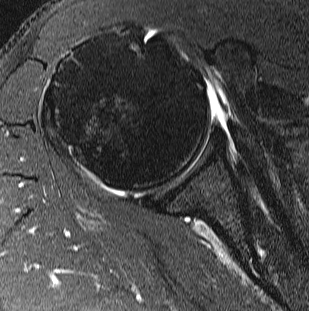
Tangent sign
- sagittal MRI
- line connecting superior coracoid and superior border scapular spine
- if supraspinatus muscle is below line, there is significant atrophy
- positive tangent sign / significant atrophy associated with larger tears / irrepairable tears
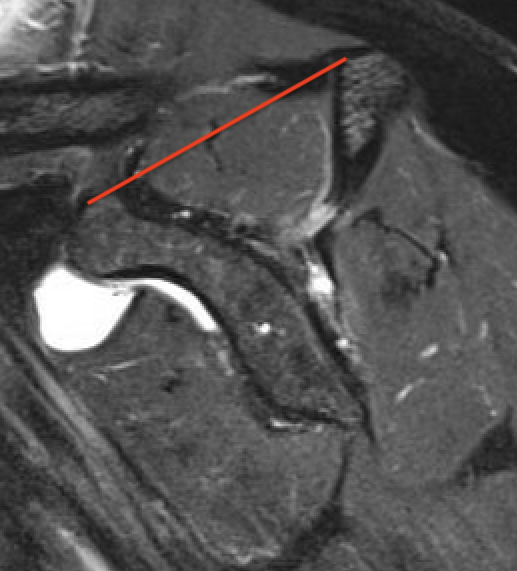
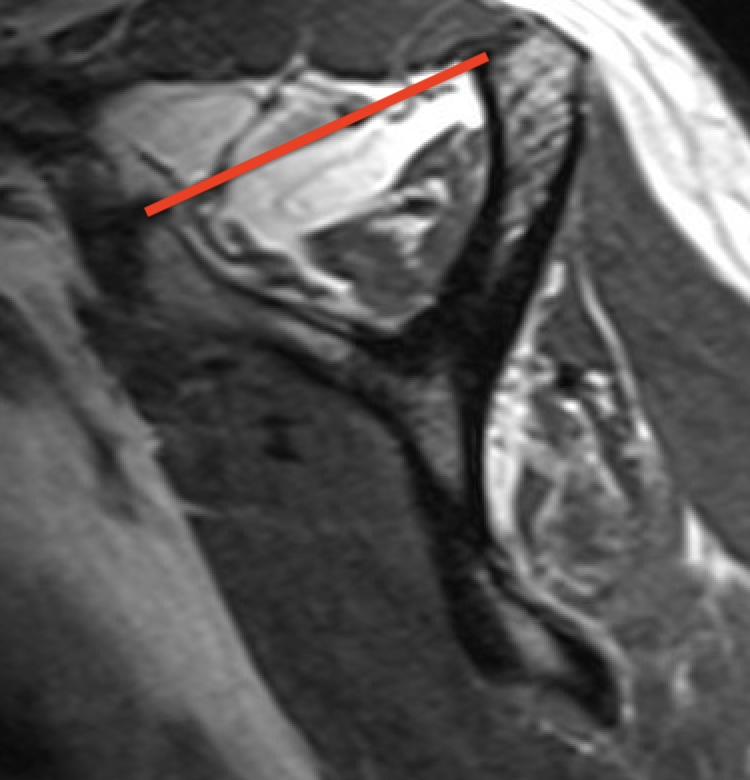
Negative tangent / no atrophy Positive tangent / significant supraspinatus atrophy
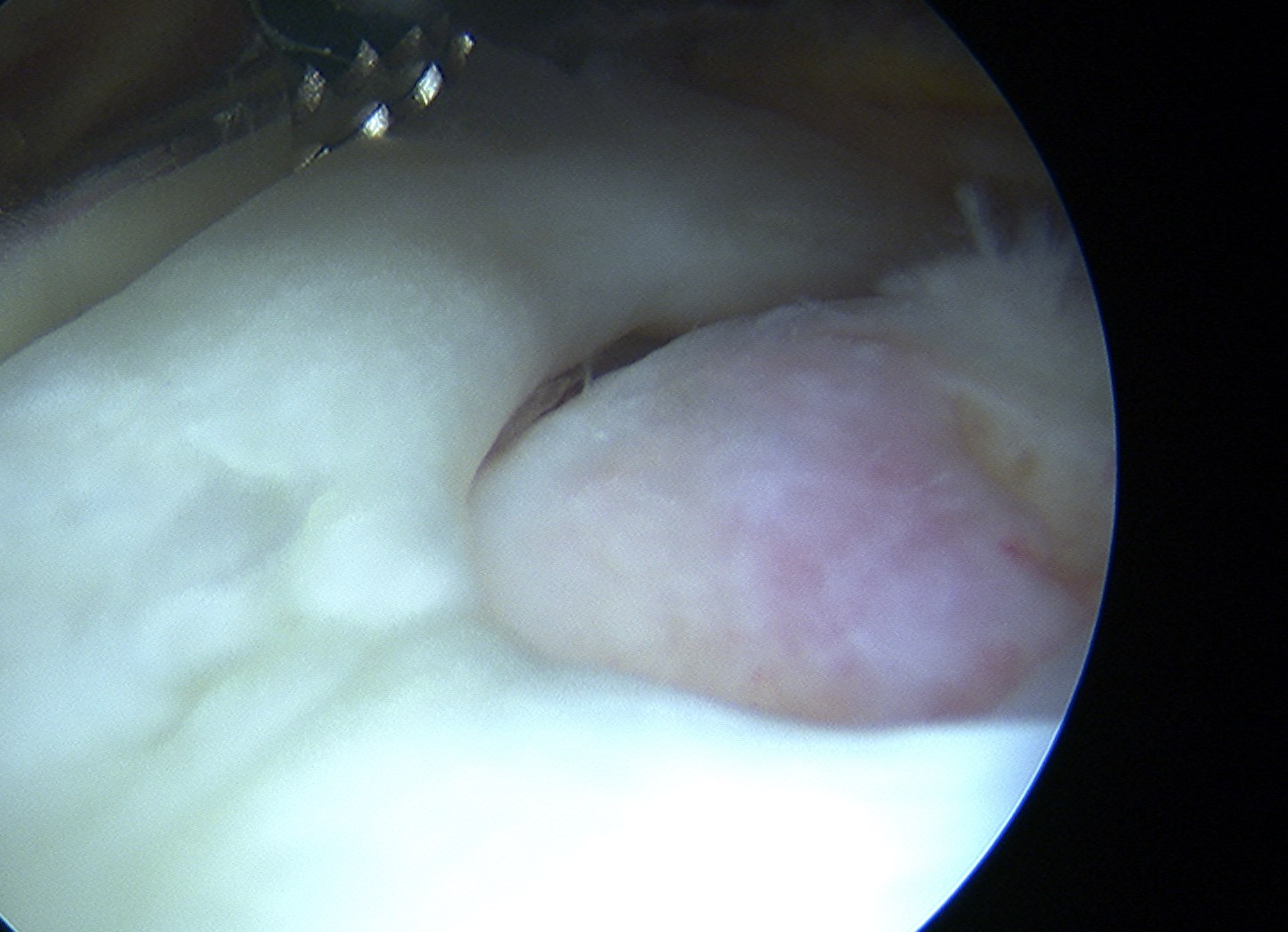
Arthroscopy
Tear patterns of supraspinatus and infraspinatus
| Crescent shaped | U shaped | L Shaped |
|---|---|---|
|
Small to medium tears Repair to footprint |
Large tears Need margin convergence then repair to footprint |
Antero-superior or postero-superior tears Need to mobilize cuff anterior or posterior |
 |
 |
 |
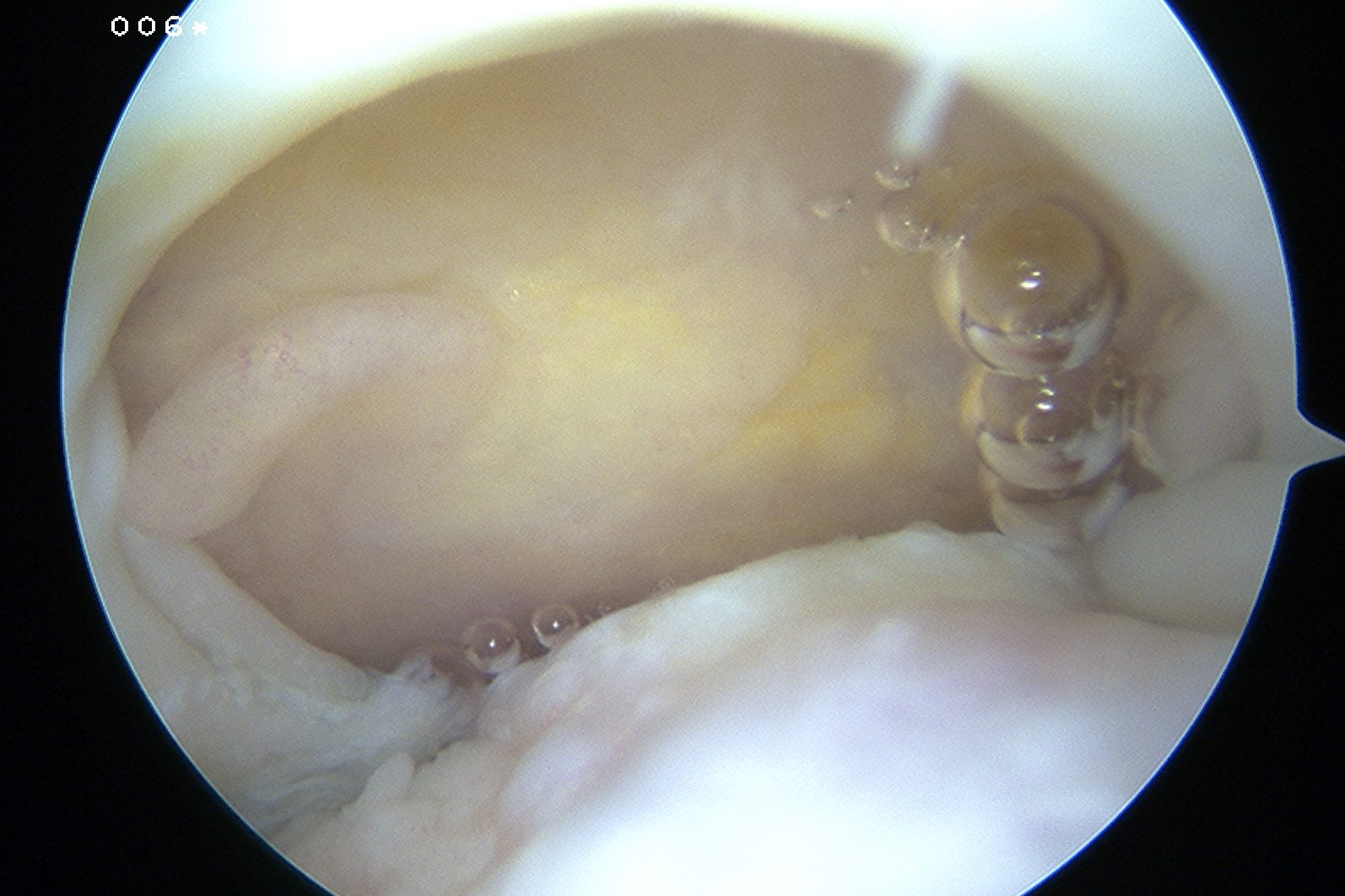
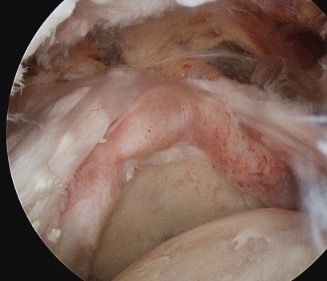
Crescent, U shaped and massive rotator cuff tears
Non operative management
Physiotherapy
- prospective cohort study of 450 patients with symptomatic full-thickness atraumatic cuff tears
- 6-12 weeks of physiotherapy
- only 27% elected for surgery (most in first 6 months)
- low expectation of physiotherapy, workers comp., and high functional demand predicted later surgery
Injections
Jiang et al J Orthop Surg Res 2023
- systematic review of cortisone v HA v PRP for rotator cuff tears
- 12 RCTs and 1000 patients
- short term pain relief with HA
- longer term pain relief and functional improvement with PRP
Operative versus nonoperative management
- meta-analysis of 6 RCT comparing operative v nonoperative management
- no difference in functional scores at 12 months
- better VAS with surgery at 12 months
- 5 year follow up of RCT
- 150 patients with 1 cm tear > 55
- no difference in functional outcome