

Indications
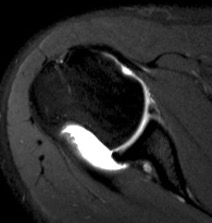
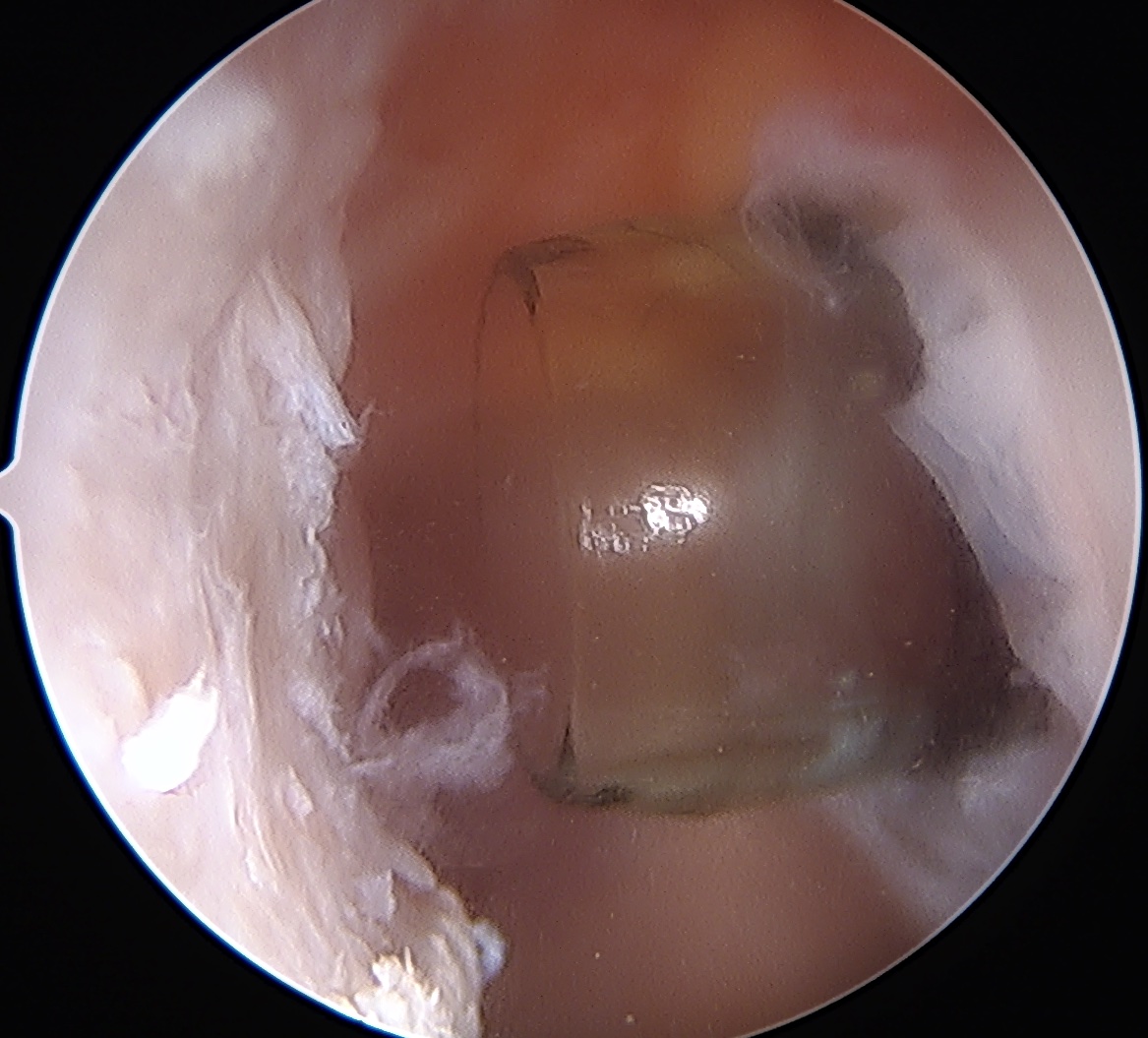
Engaging / Large Hill Sachs lesion
Concept
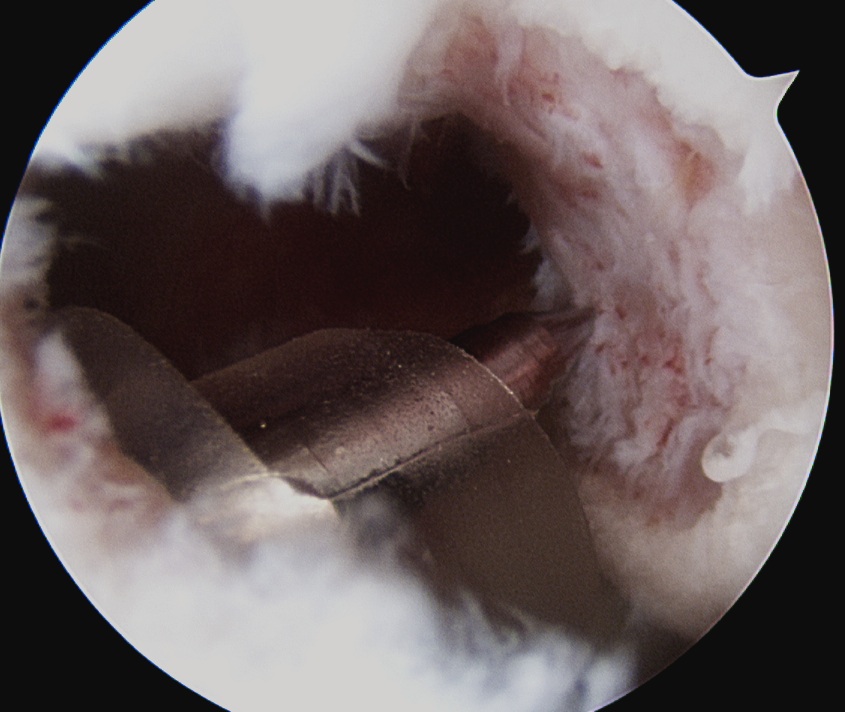
Filling Hill Sachs defect with infraspinatus / posterior capsule
Results
Villareal-Espinosa et al KSSTA 2024
- systematic review of Bankart repair v Bankart + Remplissage
- reduced recurrent instability with Bankart + Remplissage with no difference in ROM
- RCT of 100 patients with <15% glenoid bone loss
- arthroscopic Bankart v Bankart + Remplissage
- Bankart only: recurrent instability 18%
- Bankart + Remplissage: recurrent instability 4%
- medium term follow up of RCT of 100 patients with <15% glenoid bone loss
- arthroscopic Bankart v Bankart + Remplissage
- Bankart only: recurrent instability 30%
- Bankart + Remplissage: recurrent instability 10%
Technique
Timing
- typically before labral repair
- sublux the head anteriorly
Technique
- view from anterior portal
- posterior cannula over Hill Sachs lesion
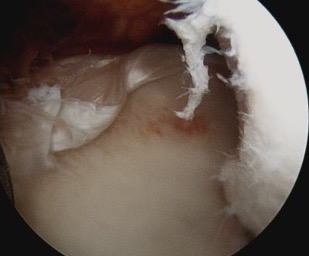
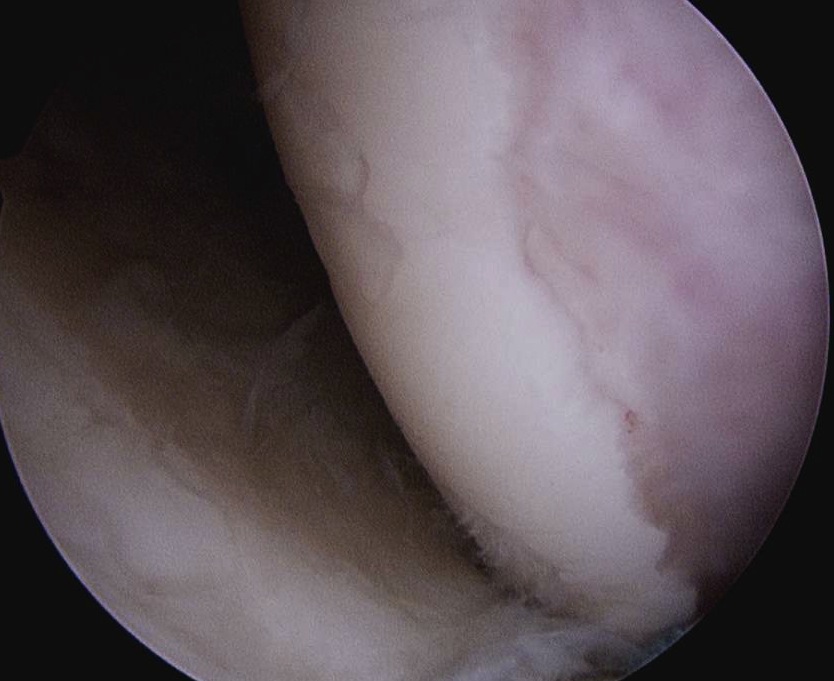
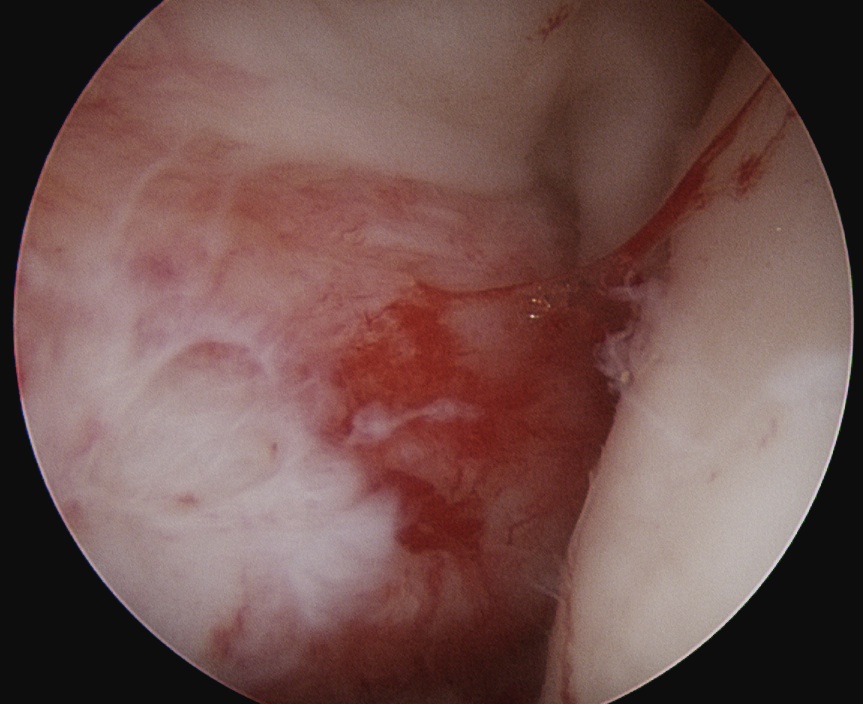
- debride base of Hill Sachs to bleeding bone
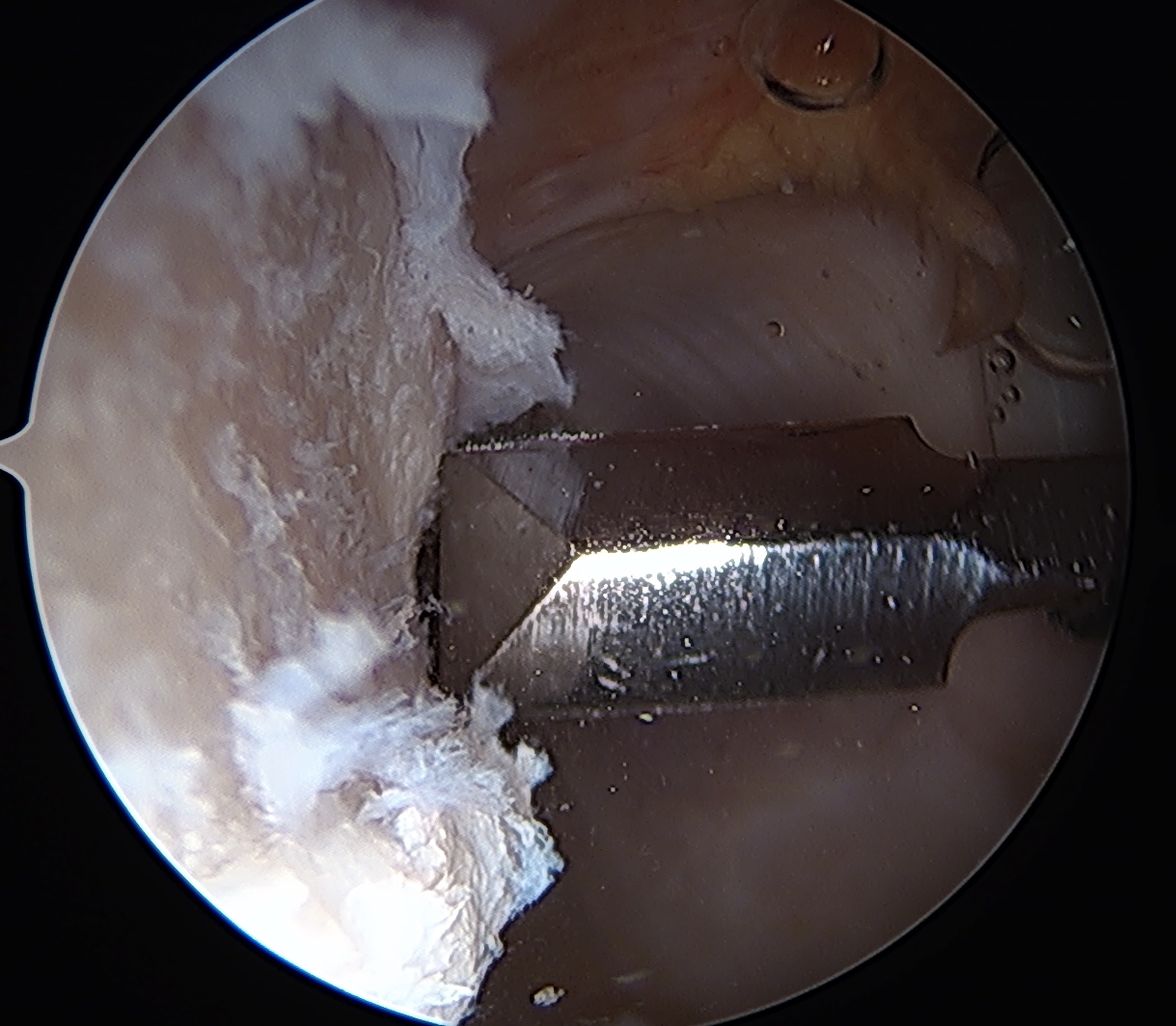
- insert anchors at medial aspect of defect
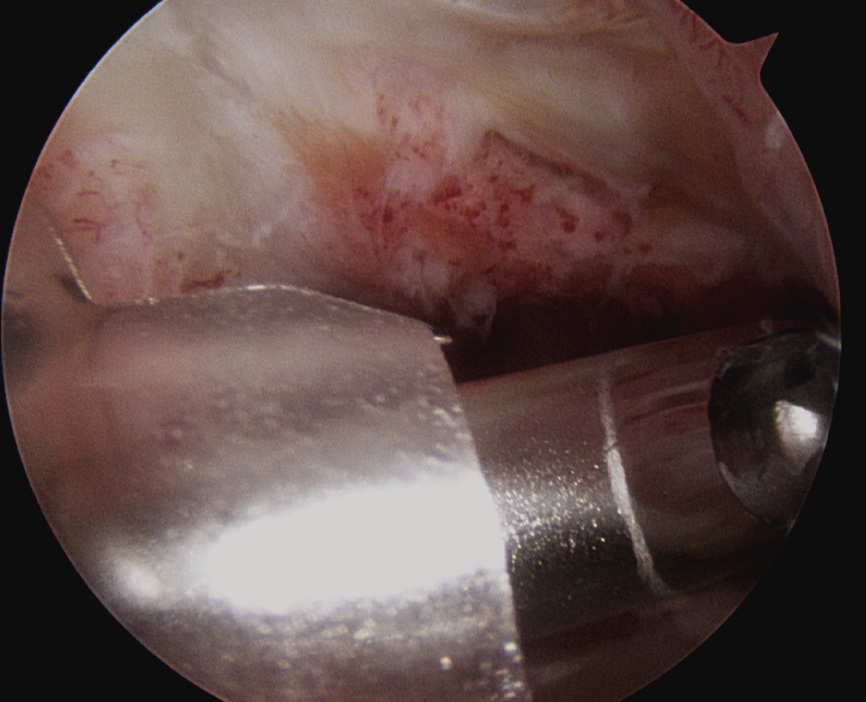
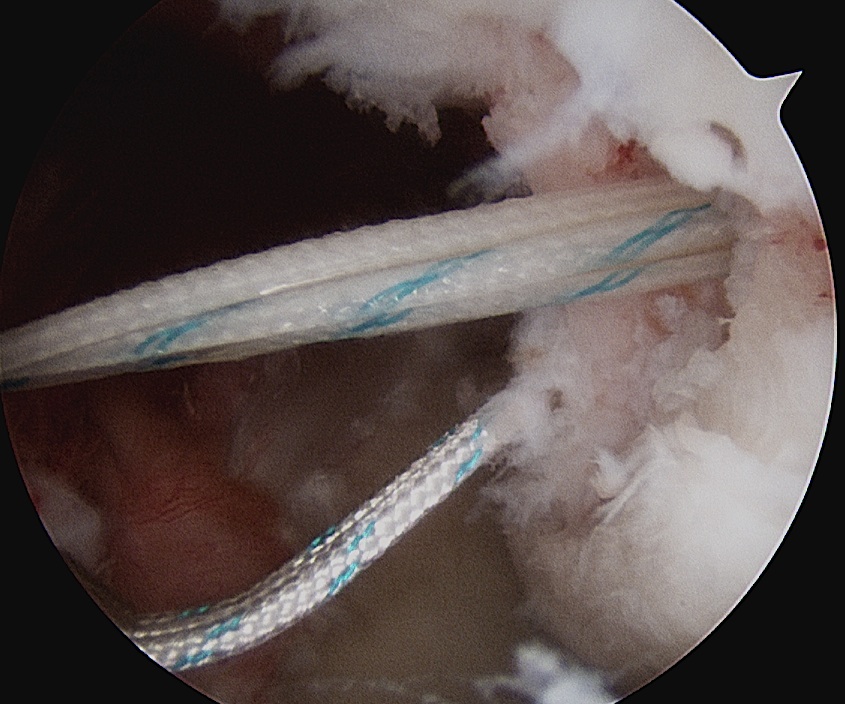
- suture passer / birds beak to take bite of capsule
- tie down into defect
- can tie blind or put camera into subacromial space
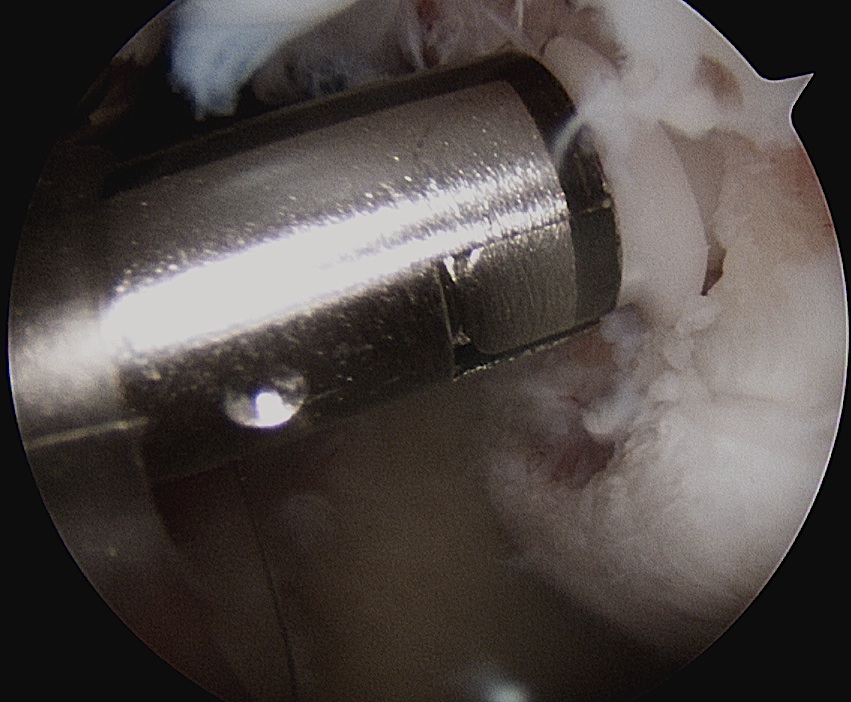
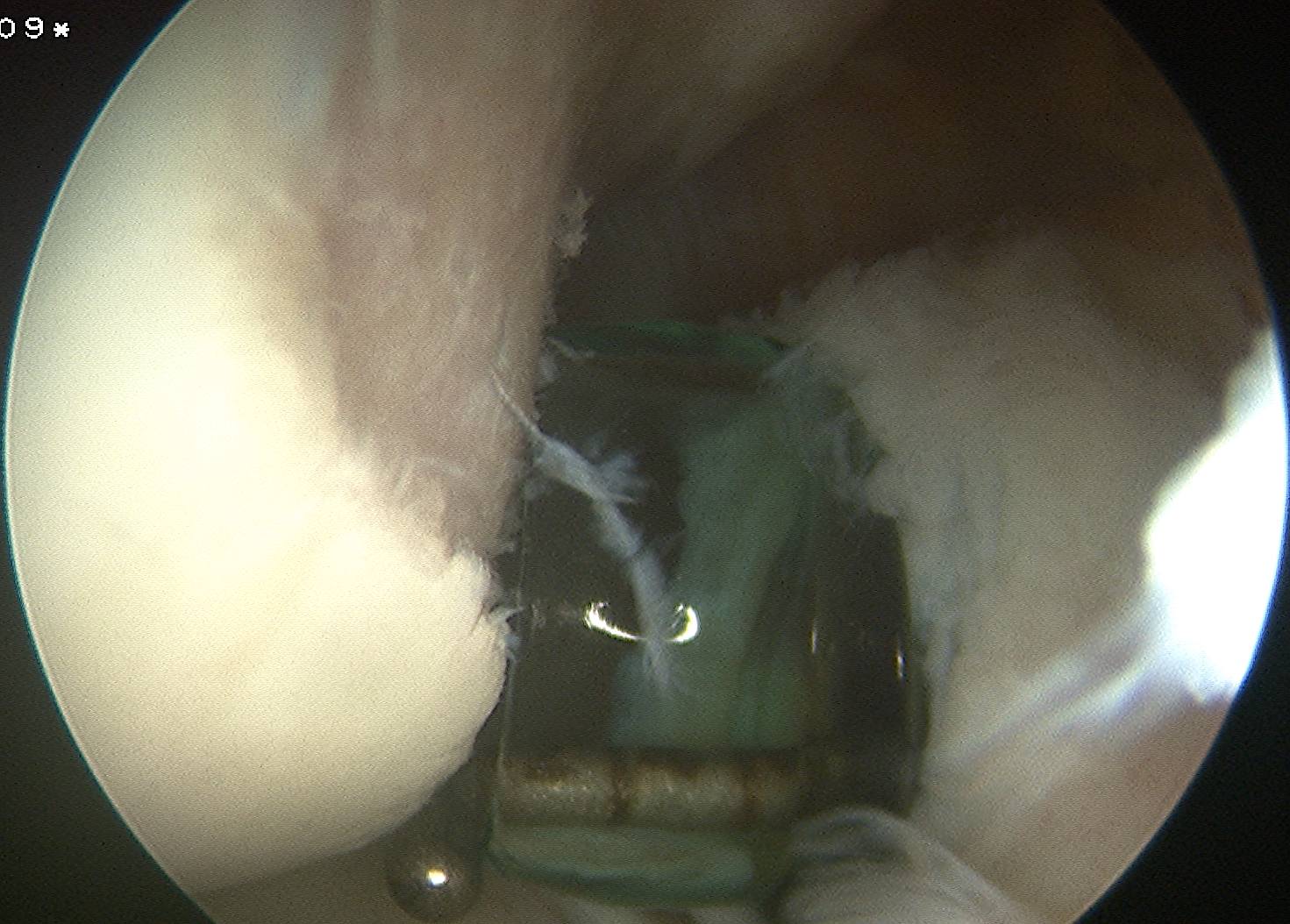
Anchor insertion into Hill Sachs lesion
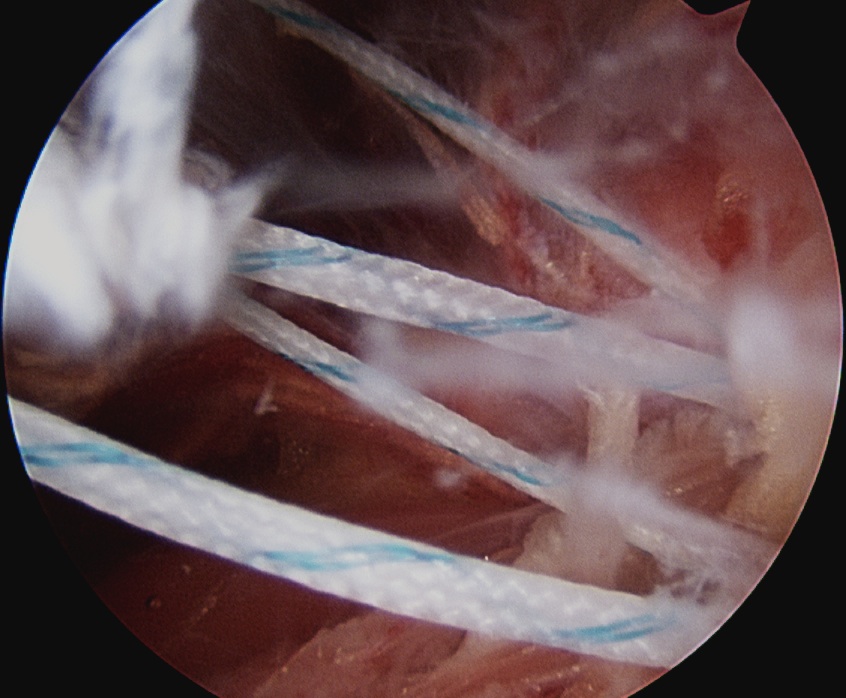
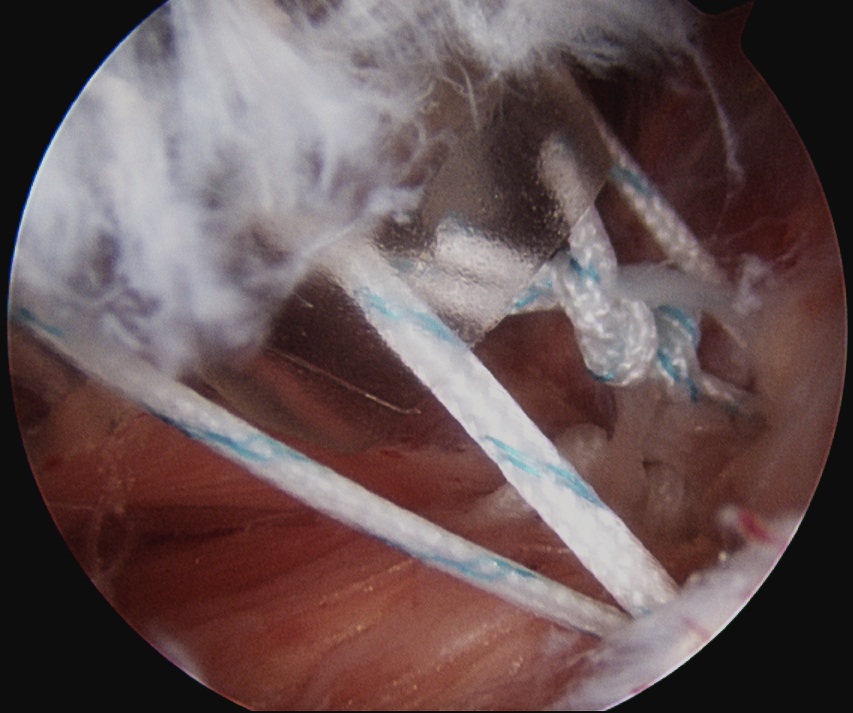
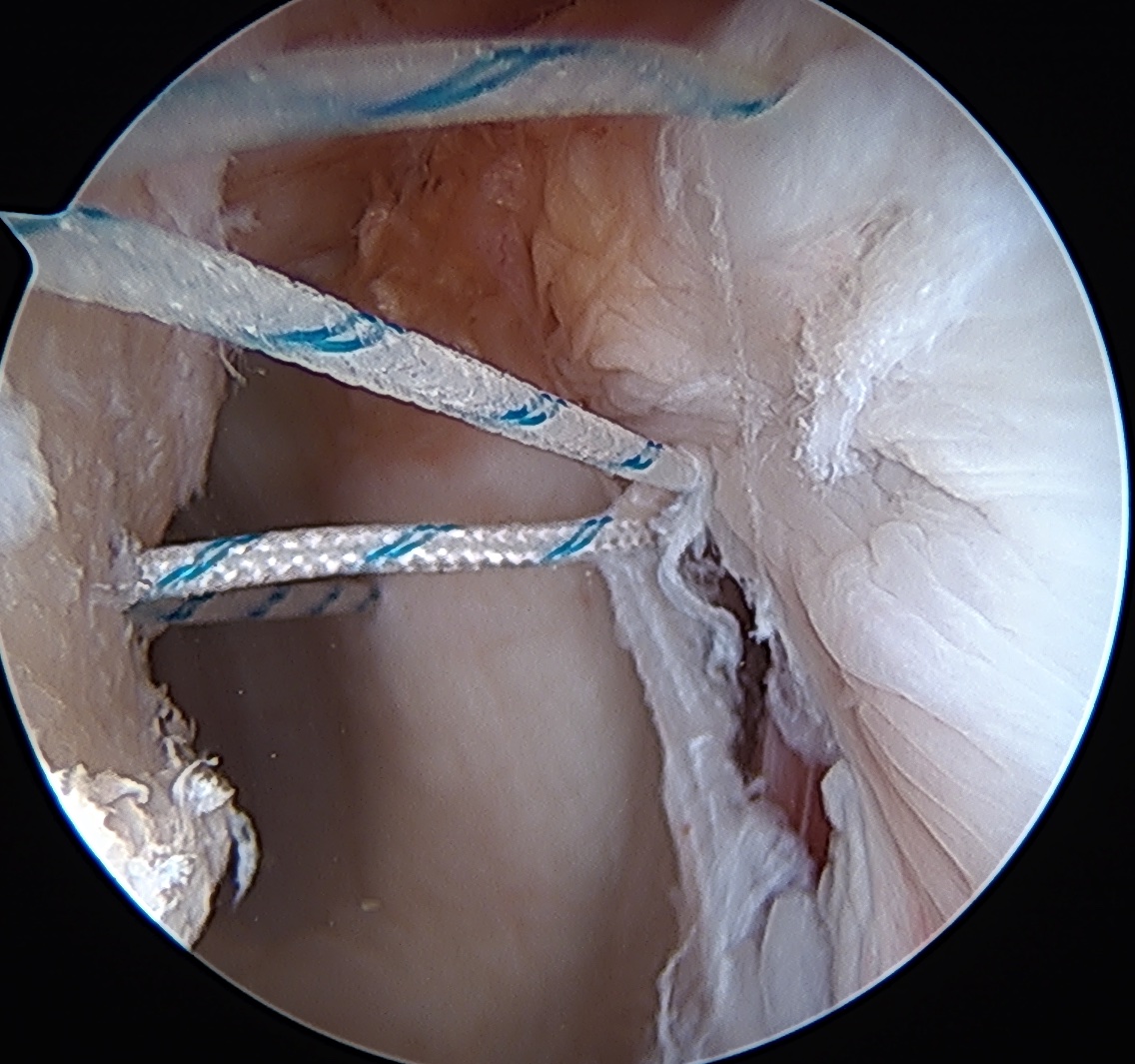
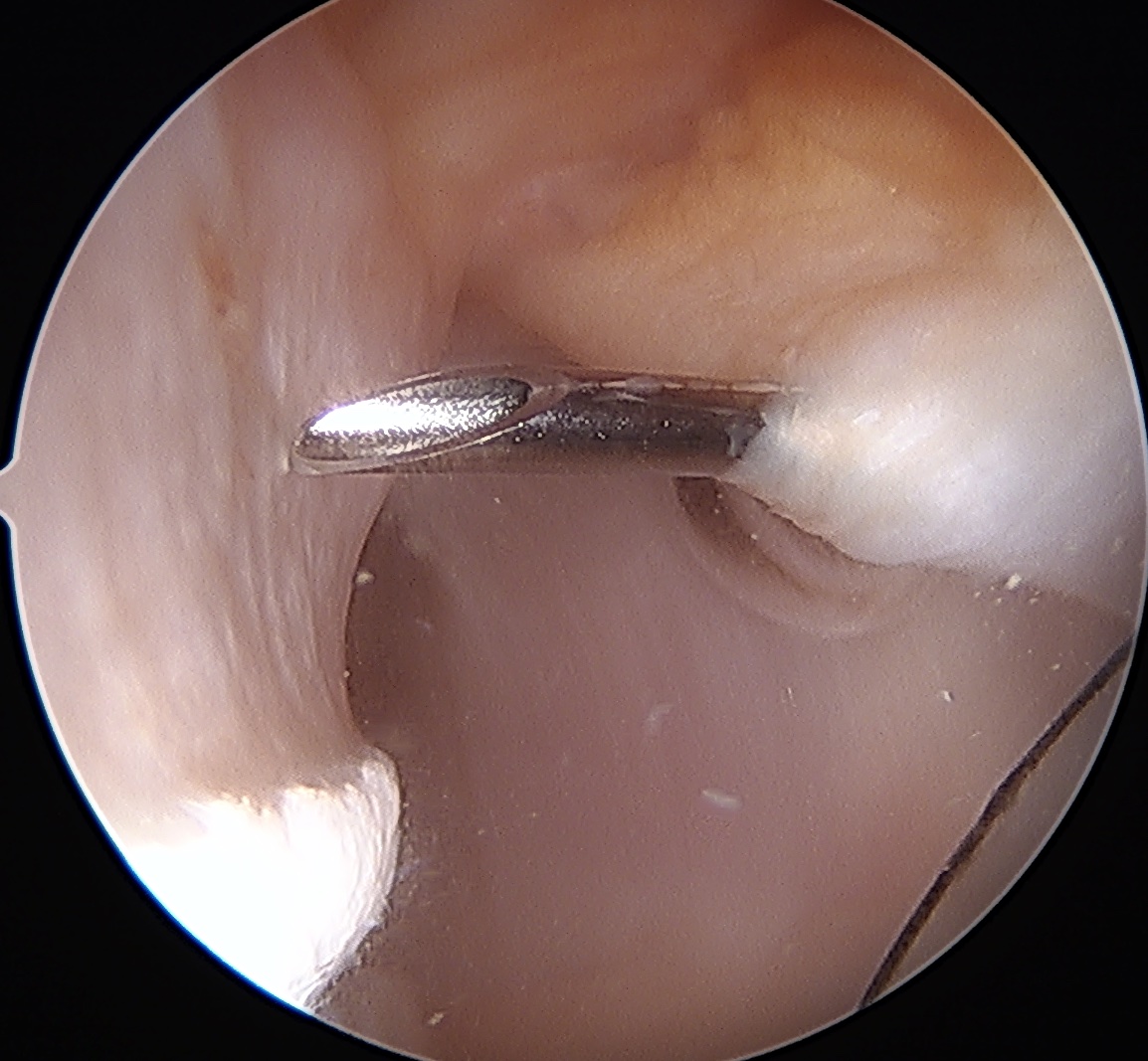
Tying knots under direct vision in the subdeltoid space using double pulley technique
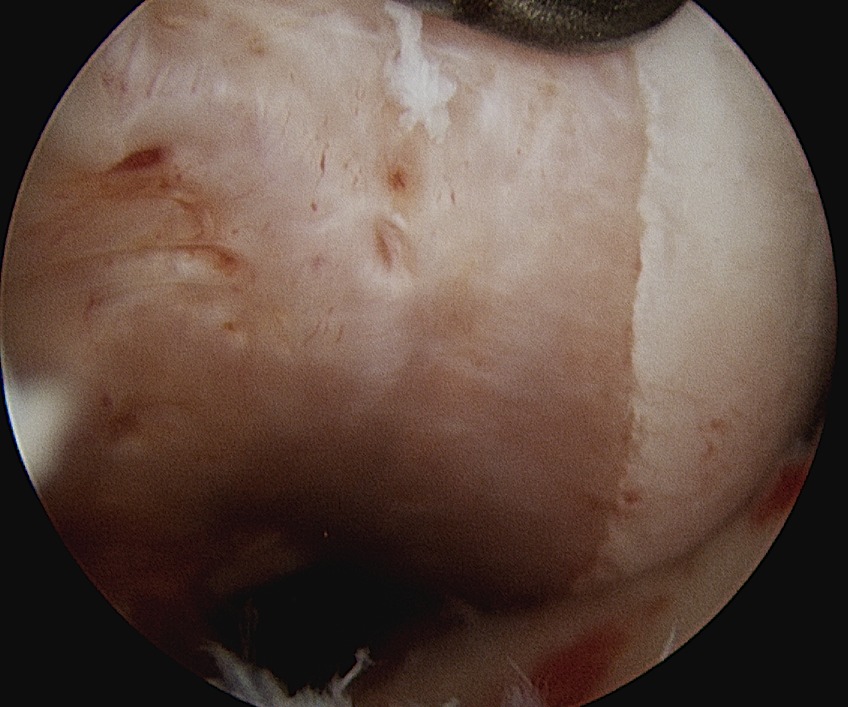
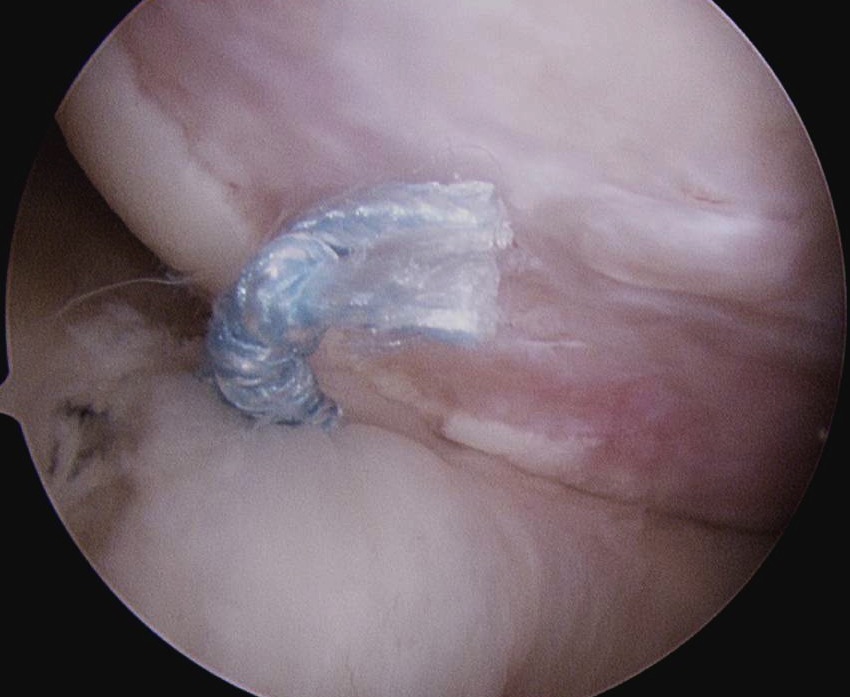
End result