Definition
Unacceptable position of radius post fracture
1. Radial Shortening > 4mm at DRUJ

2. Radial Inclination < 15°


3. Radial Tilt
- > 15° Dorsal
- > 20° Volar

4. Articular incongruity > 2mm

5. Positive ulna variance > 4mm

Biomechanics
Dorsal Tilting
1. Increases dorsal load
- maintain midcarpal alignment
2. DISI / CIND
- midcarpal instability
- get DISI pattern without interosseous ligament disruption
- may be increased in patients with ligamentous laxity
Radial shortening
1. Alter kinematics of DRUJ
2. Ulnocarpal abutment
Clinical Presentation
DDx Pain
- synovitis
- RC OA
- ulnocarpal abutment
- DISI
- TFCC tear
- RSD
Functional Loss of ROM
- DF loss > PF
- supination loss > pronation
- weak grip
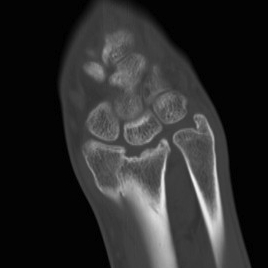
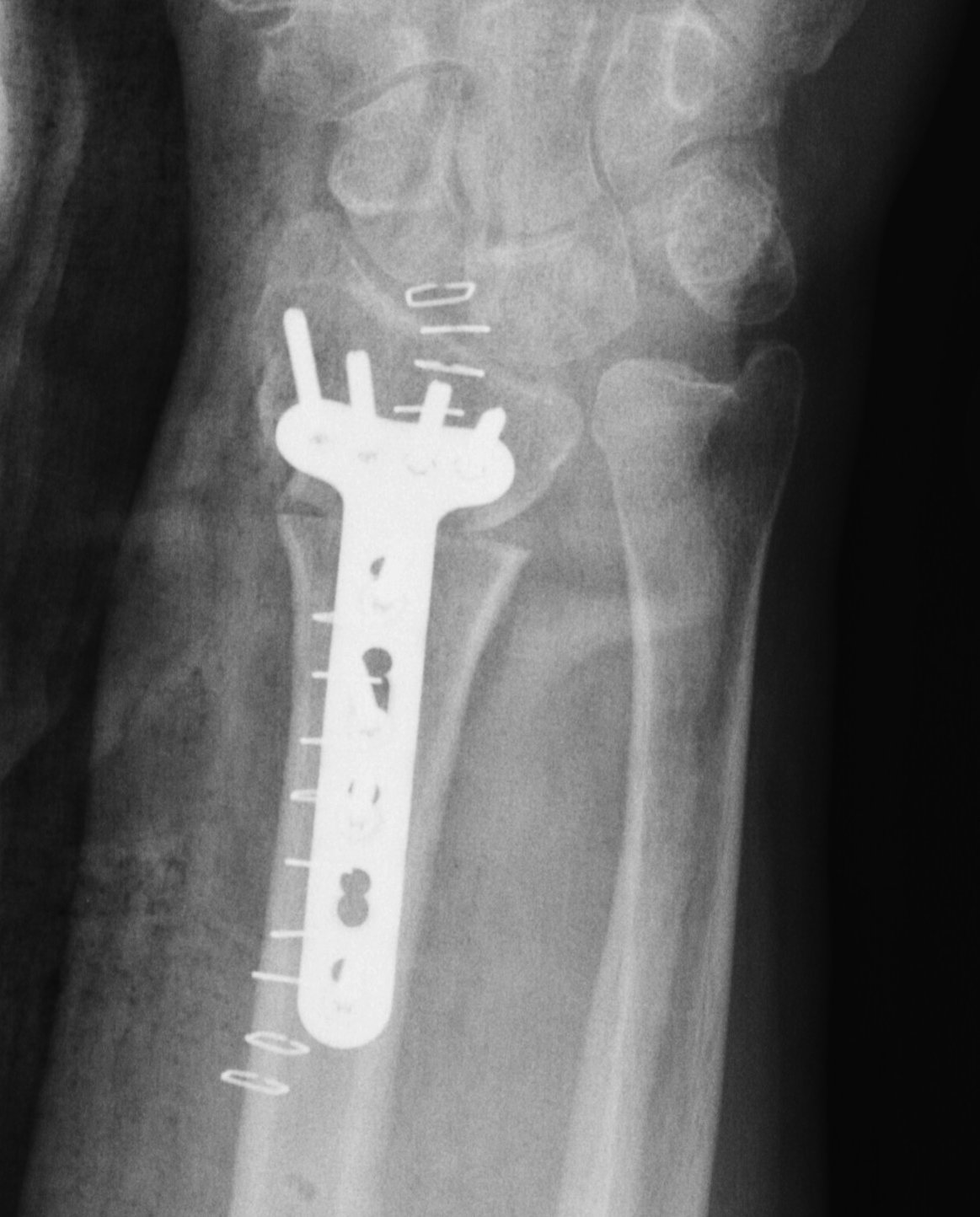
Investigation
PA film in neutral
- wrist neutral
- elbow & shoulder at 90°
5 Measurements
1. Radial inclination
2. Radial length
3. Ulnar Variance
4. Radial Tilt
5. Radial Shift
- radial Styloid from longitudinal axis
- compare to contralateral side
NHx Painless malunion
No evidence for development OA
Operative Management
Indications
Pain
Disability
Contraindications
OA in RCJ / carpus
Osteoporosis
CRPS
Timing
Early > late results
- Jupiter 1996
- < 2/12 since fracture best
However, period of non operative treatment is often desirable
Surgical Options
1. Ulna shortening
2. Radial osteotomy
3. Radial osteotomy + ulna shortening
4. Radial osteotomy + ulna ablation
5. Intra-articular ostetomy
6. Soft tissue releases
Ulnar Shortening
Indications
- short radius, positive ulna variance
- acceptable alignment distal radius
- acceptable DRUJ articular surface
Distal Radial Osteotomy
Indications
- positive ulna variance / shortening
- dorsal tilt
- DRUJ reducible by radial osteotomy
- acceptable DRUJ articular surface
Options
- dorsal opening wedge
- volar opening wedge
- volar closing wege
Dorsal Opening wedge osteotomy


Advantage
- lengthens the distal radius
- may be easier to correct in coronal and sagittal plane
- this makes it the most popular
Disadvantage
- dorsal approach / dorsal plate (extensor tendon issues)
- usually requires bone graft
- increased instability
- increased risk of non union
Template
- xray normal wrist
- calculate correction / size of bone graft
Dorsal opening wedge
- 3rd dorsal compartment
- expose distal radius
- can use half pins to control distal fragment
- check osteotomy site with II (metaphyseal, site of deformity)
- protect structures with homan retractors
- osteotomy with microsagittal saw
- correct radial articular surface in sagittal & coronal planes
- trapezoidal bi-cortical iliac crest autograft / synthetic graft
- dorsal locking plate
Volar opening wedge
Advantage
- volar approach
- apply volar plate to gain correction
Disadvantage
- require dorsal approach to bone graft
Technique
- bed of FCR approach
- protect radial with homans, osteotomy
- apply volar plate
- then either leave gap dorsally or
- second dorsal approach to insert bone graft
Closing wedge osteotomy
Advantages
- volar approach / plate better tolerated
- nil bone graft, direct bone to bone contact
Disadvantage
- can shorten radius / may need to perform ulna shortening as well
Distal Radial Osteotomy & Ulnar Shortening
Indications
- unacceptable radial alignment
- DRUJ not reduced by radius osteotomy
- acceptable DRUJ articular surface
Distal Radial Osteotomy & Ulnar Ablation
Indications
- unacceptable radial alignment
- DRUJ irreducible by radial osteotomy
- unacceptable DRUJ articular surface
Options
- Bower's hemiresection
- Darrach's
- Suave-Kapandji
Intra-articular Osteotomy
Issues
A. Scaphoid facet malunion
- intra-articular osteotomy
- radial styloidectomy
- proximal row carpectomy
B. Lunate facet malunion
- osteotomy
- radio-lunate fusion
C. Global wrist involvement
- early intra-articular osteotomy
- total wrist fusion
D. Anterior / Posterior rim malunion
- simple bone resection
Soft Tissues Releases
Options
DRUJ volar capsulotomy
- restores supination
DRUJ dorsal capsulotomy
- restores pronation
+/- Pronator Quadratus release