


Options
Percutaneous K wires
Volar locking plate
External fixation
Bridging plate
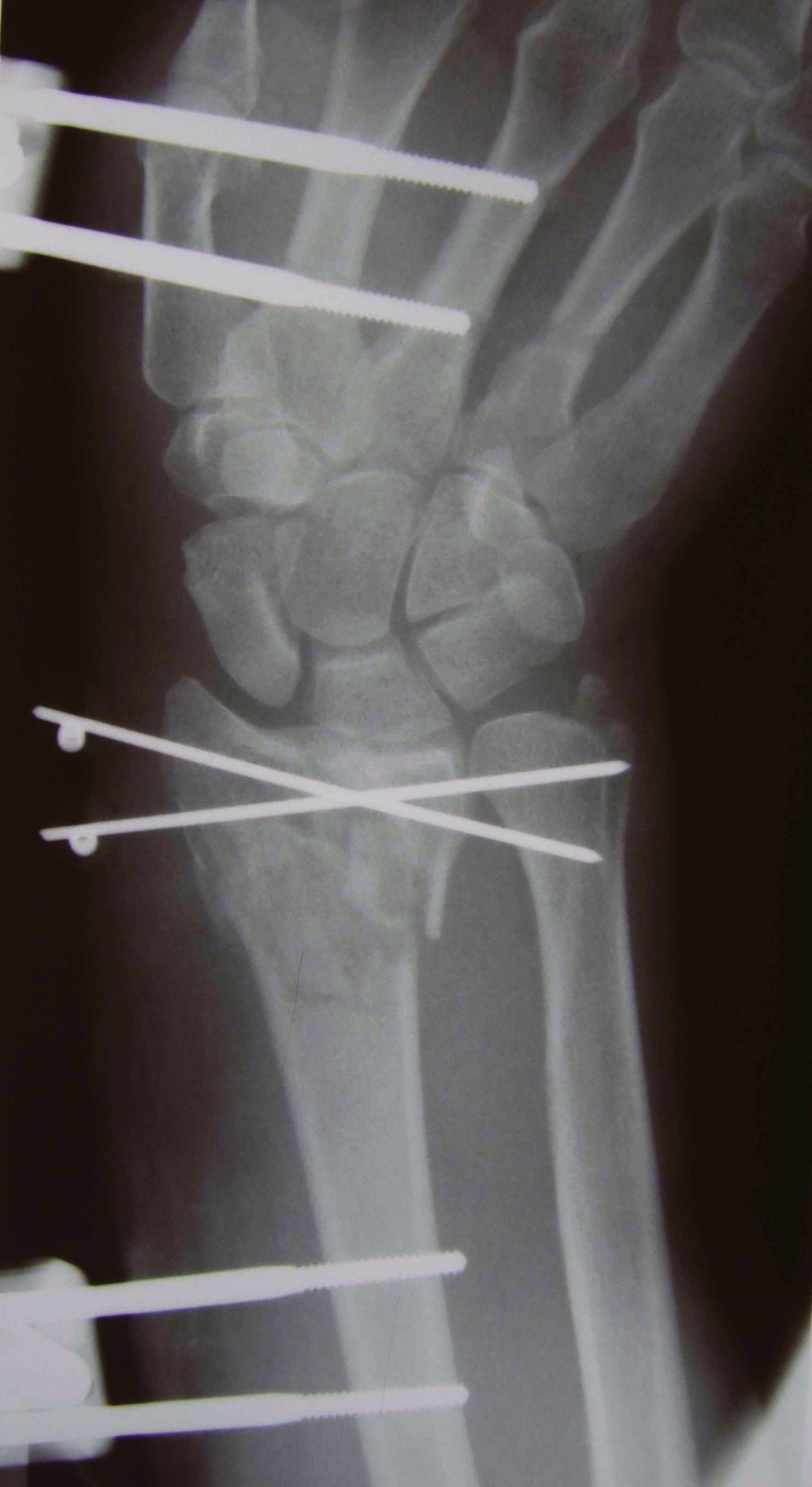
Percutaneous K Wire


Issues
Increased pin site infections
No early immobilization
Technique
Youtube K wire distal radius fracture video
Reduce fracture under anesthesia and fluoroscopy
Radial K wire
- through radial styloid
- can make small incision / blunt dissect to protect branches SRN
- cross fracture site and engage other cortex
- 1.6 or 2 mm K wire
Dorsal K wire Kapandji technique
- percutaneous by hand into fracture site
- tilt distally to reduce dorsal displacement of distal fragment
- drive into proximal radius and engage volar cortex
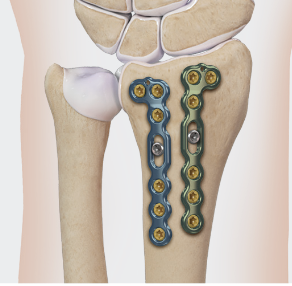
ORIF with locking plates



Advantages
Accurate restoration of intra-articular anatomy
Stable fixation with early mobilisation
Fragment specific plates
| Volar locking plates | Volar rim plates | Radial styloid plates |
|---|---|---|
|
Locking screws act as fixed angle devices Variable angle screws |
For very distal fracture fragments
|
Supplementary radial column fixation |
|
 |
 |
| Dorsal fragment specific plates | Dorsal rim buttress plate | Volar lunate plates |
|---|---|---|
|
|
Arthrex dorsal rim plate | Arthrex volar lunate plates |
 |
 |
 |
Volar locking plate technique
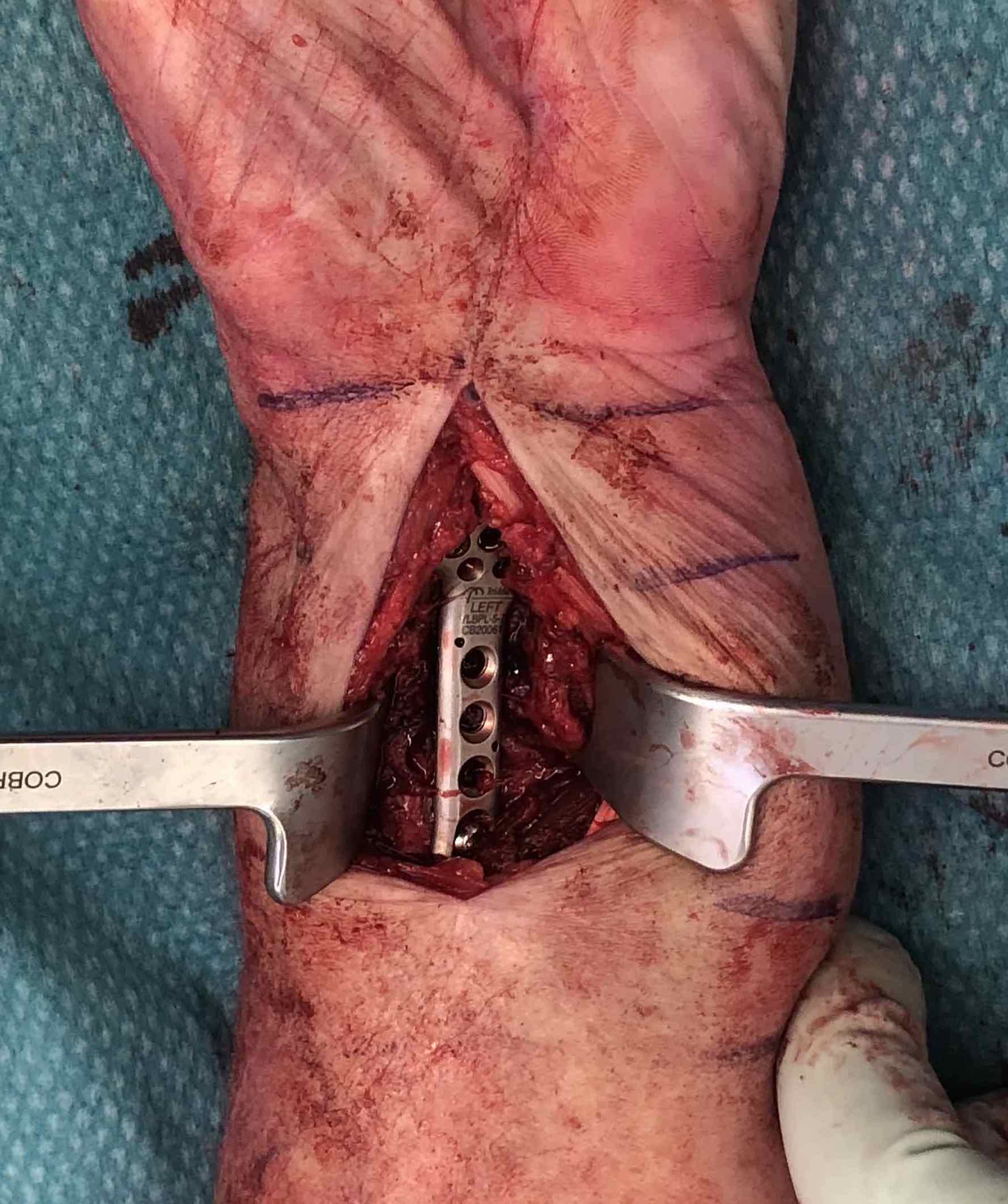


AO surgery modified Henry to distal forearm
Vumedi volar locking plate distal radius
Bed of FCR approach
- incision over FCR and mobilize ulnarly
- divide fascia in bed of FCR and retract radial artery laterally
- L shaped released of pronator quadratus
- cannot make volar capsulotomy - divides radiocarpal ligaments and causes instability
- elevate 1st extensor compartment (APL / EPB)
- release brachioradialis from radial styloid
Reduce fragments and temporarily stabilize with K wires
- apply volar plate with screw fixation in scaphoid and lunate fragments
- ensure not beyond watershed line to avoid flexor tendon irritation / rupture
- engage dorsal cortex but not too long to prevent EPL rupture
- on lateral, raise hand 30o to view joint
- +/- radial styloid plate if required
Dorsal plates technique
Advantage - can open and expose the radiocarpal joint
AO surgery dorsal approach to distal radius
Vumedi dorsal plating distal radius video 1
Vumedi dorsal plating distal radius video 2
Vumedi dorsal plating distal radius video 3
Dorsal approach over Lister's tubercle
- expose extensor retinaculum
- 3/4 approach
- divide extensor retinaculum over 3rd extensor retinaculum / EPL
- EPL radial / EDC ulna
- can make a transverse dorsal arthrotomy to expose joint without causing instability
- perform ORIF with plates
- close extensor retinaculum over plate and under extensor tendons
Results
Immobilization
Quadlbauer et al Clin Rehab 2022
- RCT of 5 weeks cast v removable splint and early mobilization
- 116 patients with distal radius fracture treated with volar locking plate
- improved ROM and grip strength at 1 year with early immobilization group
Pronator quadratus repair
Turley et al Acta Orthop Trauma 2023
- systematic review of 5 RCTs and 270 patients
- no difference in outcomes with pronator quadratus repair
Arthroscopic assisted
Vumedi arthroscopic assisted distal radius ORIF video
Shihab et al J Hand Surg Am 2022
- systematic review of arthroscopic assist v fluoroscopic assist
- 6 studies and 280 patients
- reduced articular step off with arthroscopic assist
- longer OR times with arthroscopic assist
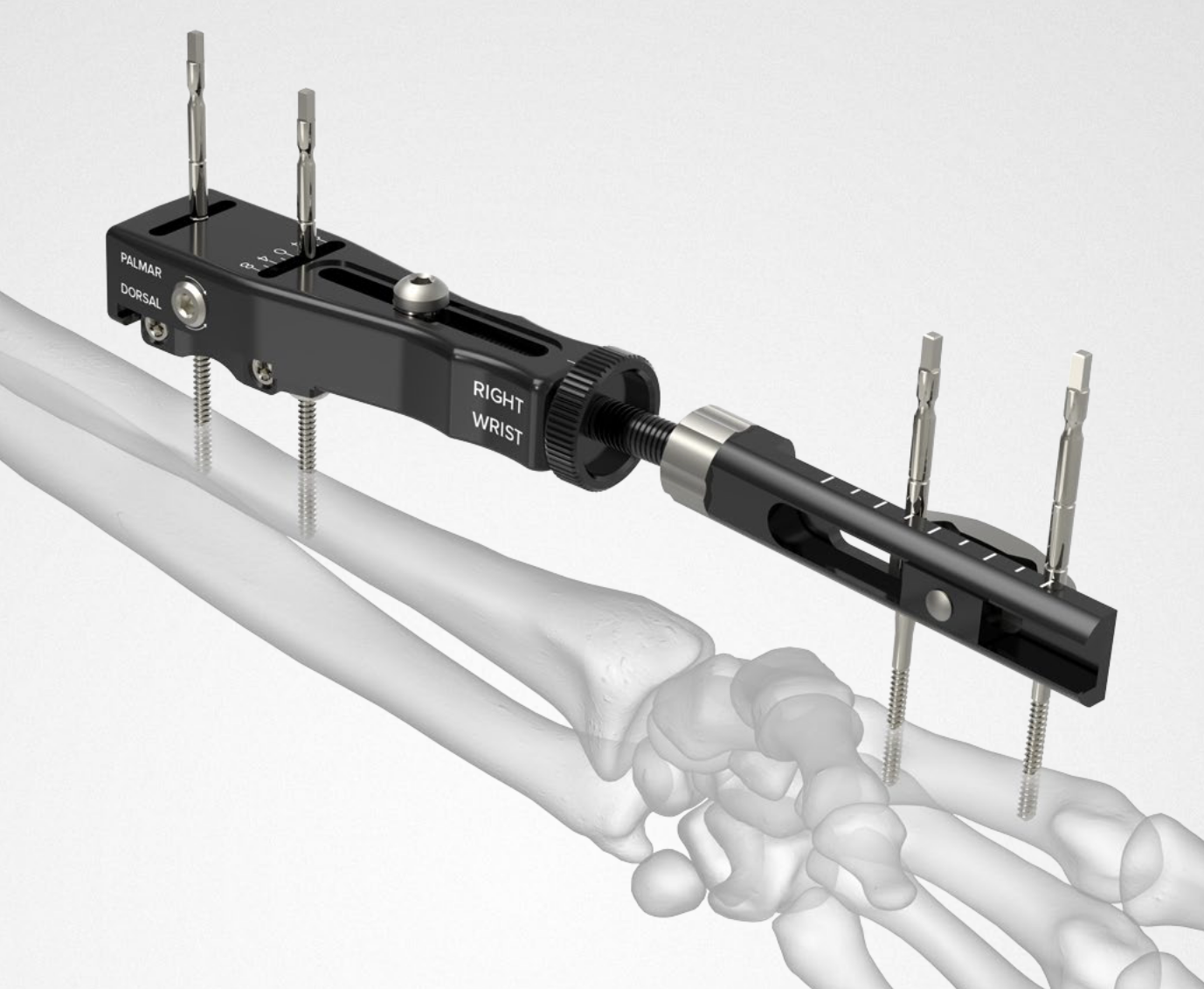
External Fixation + / - Supplemental K wires

Indications
Compound fractures
Severe unreconstructable injuries
Very osteoporotic bone
Technique
AO surgery wrist external fixation
Vumedi wrist external fixation video
Dorsal distal radius
- 2 x half pins 4mm
- proximally between EDC and ECRB / ECRL
- bare area of radius
Metacarpal
- 2 x half pins index or second metacarpal 3 mm
- distal and proximal metaphysis
- insert at 30 degrees to prevent transfixing extensor tendon
- flex MCP to 90 degrees with when placing distal pin to avoid extensor hood
Dorsal distraction plating



Indication
Internal radiocarpal distraction
- unreconstructable distal radius fractures
- early weight bearing in poly trauma patients
- osteoporotic bone
Advantage - no pin site infection from external fixation
Disadvantage - need to remove plate at 3 - 4 months once fracture united
Technique


AO surgery foundation extended dorsal approach wrist
AO surgery foundation dorsal distraction plate
Arthrex dorsal spanning plate 2 incision video
Extended dorsal approach
- protect sensory radial nerve
- open 3rd extensor compartment / retract EPL radially
- mobilized 4th extensor compartment / retract EDC ulnarly
- bare area of radius proximally between EDC and ECRB / ECRL
Fixation to 2nd or 3rd metacarpal first
- 2nd metacarpal: under 2nd extensor compartment
- 3rd metacarpal: under 4th extensor compartment
- reduce / distract joint
- +/- additional radius fixation
Results
- systematic review of dorsal distraction plating
- 50% of wrist flexion extension compared to contralateral limb
- grip strength 80%
Specific fracture patterns
Volar Barton's


Definition
Intra-articular fractures of the dorsal articular margin of the distal radius
Unstable and allow volar subluxation of the carpus
Management
Volar locking plate
Volar buttress plate without distal screws




Dorsal / Reverse Barton's


Definition
Fractures of the dorsal articular margin of the distal radius
Dorsal radiocarpal subluxation if the volar ligament / capsule are disrupted
Management
Dorsal buttress plates
Vumedi dorsal plating distal radius video 1
Radial styloid fractures / Chauffeur's Fracture
Associations
Perilunate fracture / dislocations
Radiocarpal dislocation
Scaphoid fractures
Options
K wires / screw fixation / radial styloid plate / volar locking plate
Approach
- volar approach
- dorsal-radial approach
Dorso-radial approach / direct approach to radial styloid
AO foundation dorso-radial approach
Between 1st and 2nd extensor compartments
- protect sensory branches radial nerve
- release brachioradialis tendon
- release 1st compartment and mobilize 2nd



Volar rim fractures
Definition
Very distal fractures
Need distal plates
Low profile plates to protect flexor tendons

Technique
Plate sits distal to watershed line
- variable angle screws
- sit in subchondral bone
- can cause flexor tendon irritation and may need removal



Outcomes
Lari et al Eur J Orthop Surg Traumatol 2023
- systematic review of surgical treatment of volar rim fractures
- 26 studies and 600 patients
- implant removal 22%
- flexor tendon irritation 6%