
Definition
Femoro-acetabular impingement (FAI)
- abnormal contact between the femoral head neck junction and the acetabular rim
- causes pain secondary to labral and chondral lesions
Types
Cam
Pincer
Mixed - CAM and Pincer
Cam impingement
- abnormal femoral head morphology at head neck junction
- loss of sphericity
- typically anterolateral
Pincer impingement
a. Global
- overcoverage of femoral head
- profunda, protrusio
- acetabular retroversion / relative anterior rim overcoverage
b. focal
- os acetabuli
- focal acetabular lesion

Mixed
- combination of pincer and Cam impingement

Epidemiology
- MRI of bilateral hips in 200 asymptomatic people
- 14% had Cam deformity in at least one hip
- 80% men, 20% women
Gao et al J Orthop Surg Res 2021
- MRI of 125 hips in 70 asymptomatic patients
- 53% of hips had a labral tear
Etiology
Developmental / sports
- increased incidence of Cam in hockey / basketball / football / soccer
- suggests changes to femoral epiphysis with certain athletic pursuits
Pediatric hip disease / SUFE
Acetabular retroversion
- posteriorly orientated acetabular opening
- relative prominence of anterior rim
Coxa profunda (deep socket) / Protrusio
History
Groin pain
- with activity
- with flexion
C shaped pain
- patient uses hand to grip anterior and posterior hip
Examination
FADIR (Flexion-adduction Internal Rotation)
FABER (Flexion-abduction External Rotation)
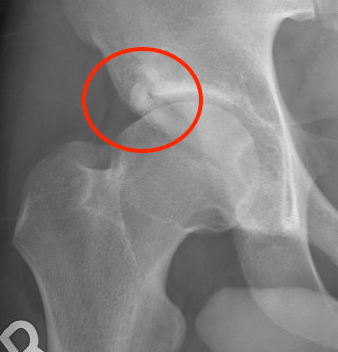
X-ray
True AP
Coccyx and symphysis pubis within 1-2cm of each other
- exclude osteoarthritis
- pincer
- dysplasia
- retroversion / crossover sign
- os acetabuli / ossification labrum
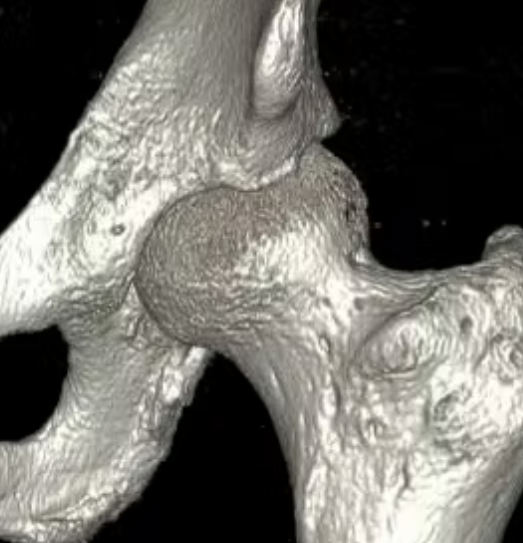
- bony prominence junction anterolateral head and neck - Cam


Bilateral pincer


Ossified labrum

Os acetabuli
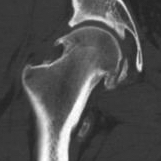
45 and 90 degree Dunn view
Look for Cam morphology


Small Cam on Dunn view Large anterior Cam on Dunn view
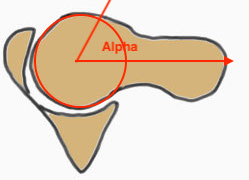
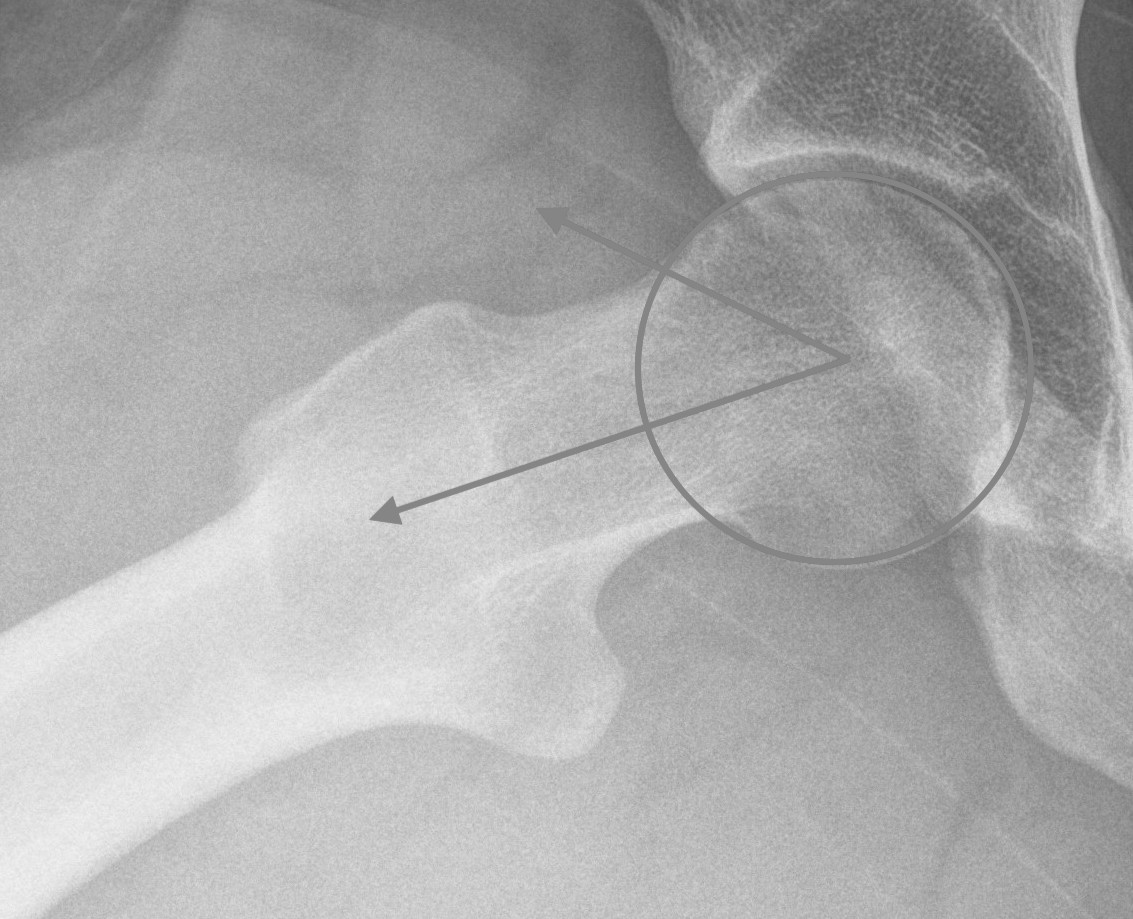
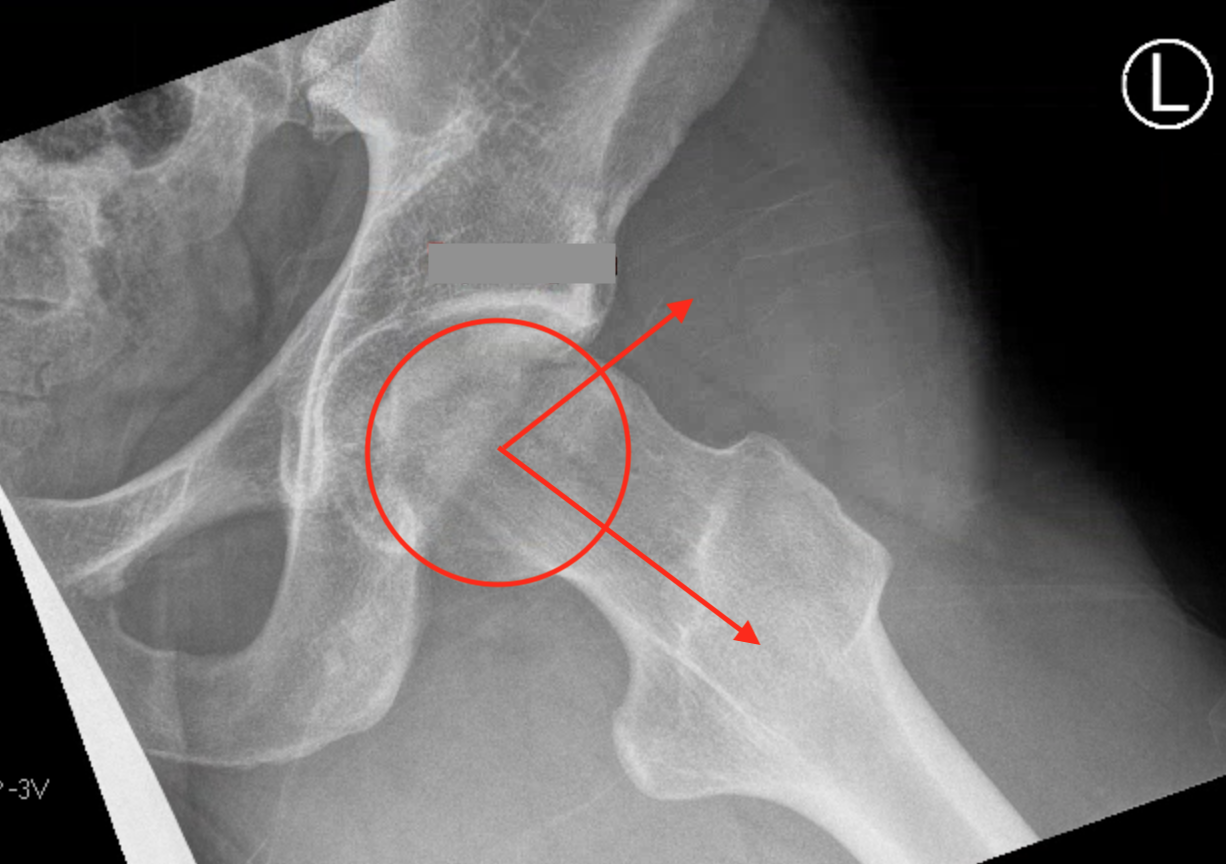
Alpha angle
Measurement
- centered in the center of the femoral head (best fit circle)
- formed by two lines
- one line center of the femoral neck axis
- a line where the femoral head leaves a best-fit circle
- higher alpha angle with Cam lesion
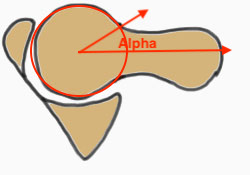
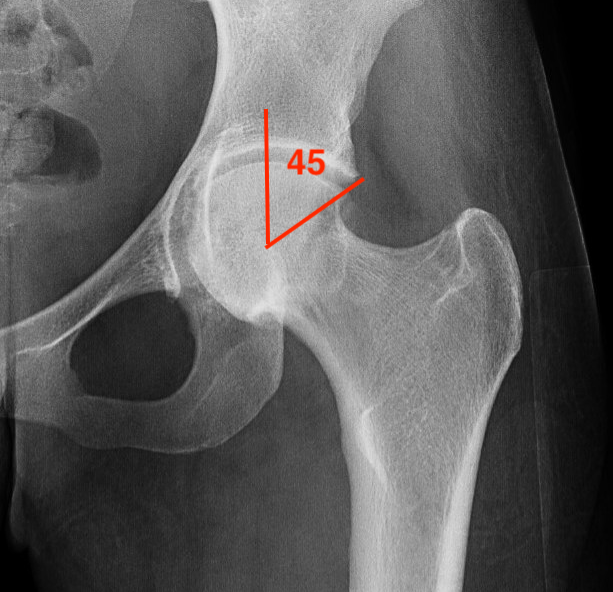
Alpha < 55 degrees Alpha > 55 degrees
Barrientos et al J Hip Preserv Surg 2016
- 38 patients with Cam versus 108 control
- CT scans
- mean 48+/-5 degrees in controls
- mean 67+/-12 degrees in patients with symptomatic Cam
Kowalczuk et al Sports Med Arthrosc Rev 2015
- systematic review
- Cam lesions with elevated alpha angles predispose to development of OA
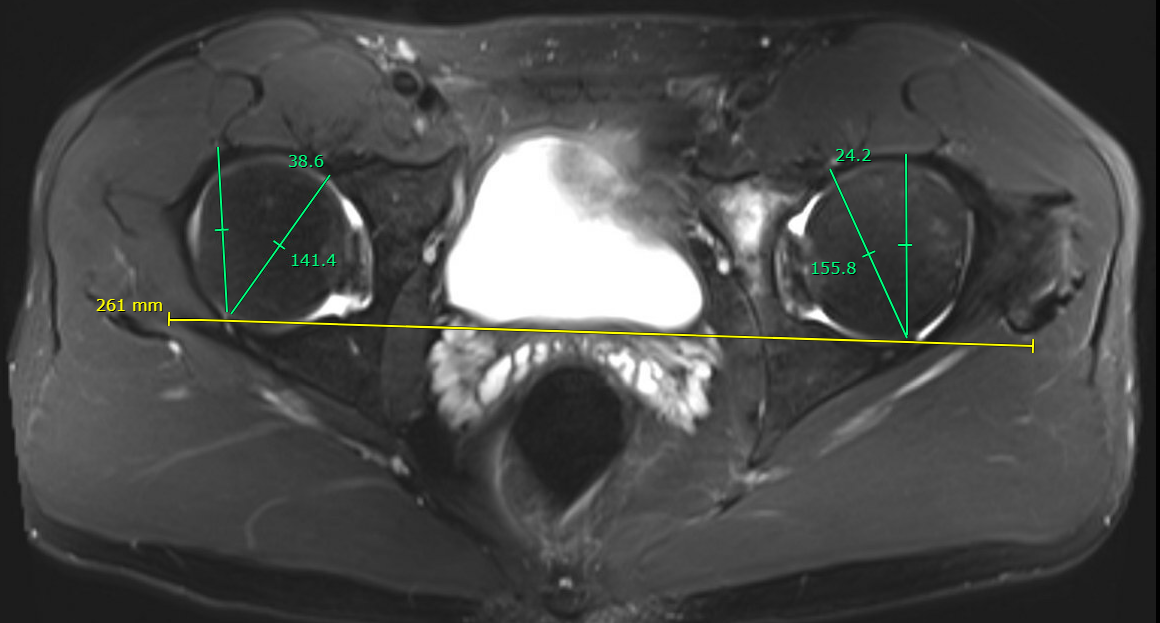
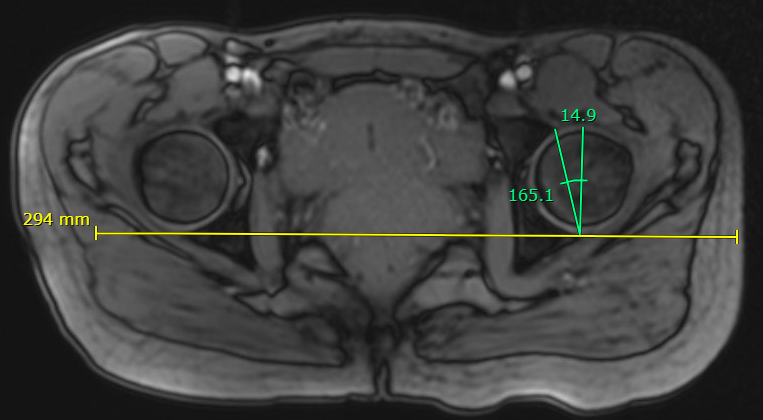
Lateral centre edge angle (LCEA)
Measurement
- vertical line drawn from the center of the femoral head
- line from the center of the femoral head to the lateral acetabular rim
- normal 20 - 40 degrees
- dysplasia < 20 degrees
- profunda > 40 degrees

Increased LCEA in profunda
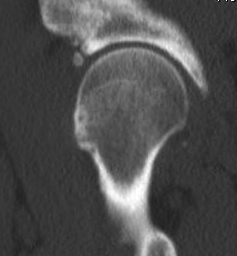
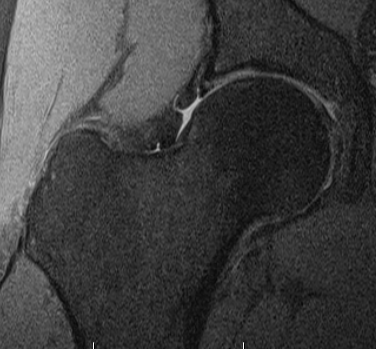
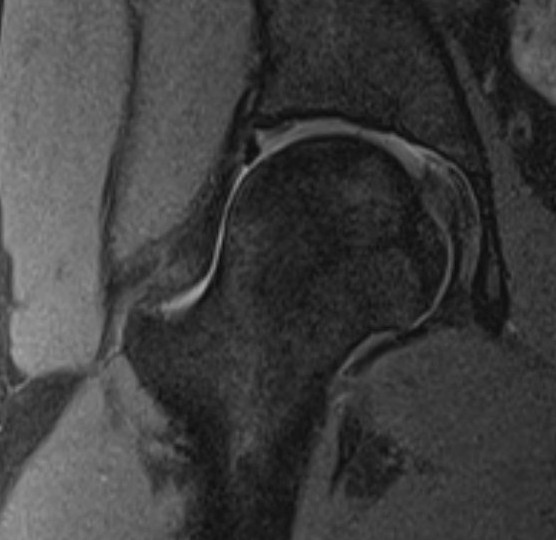
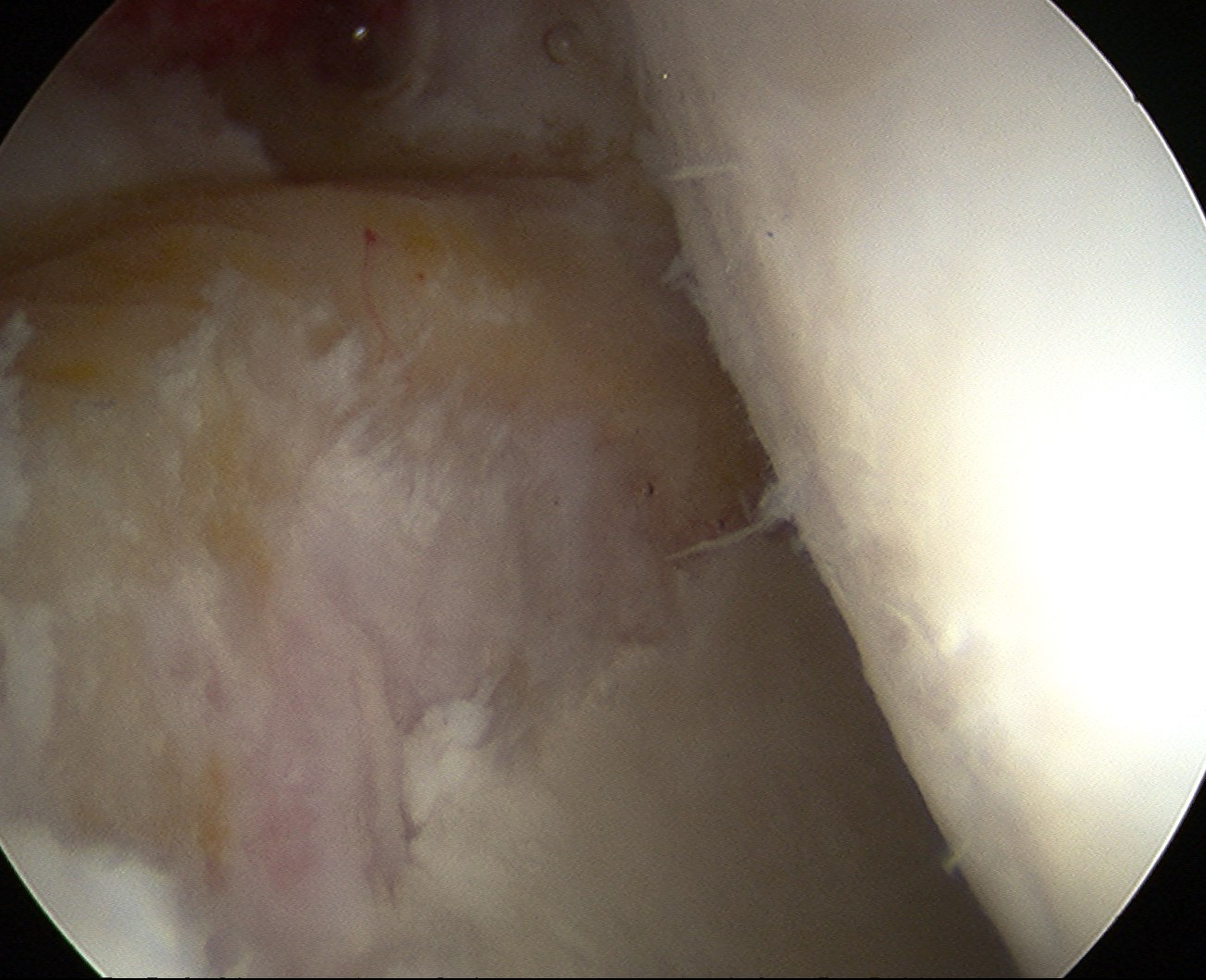
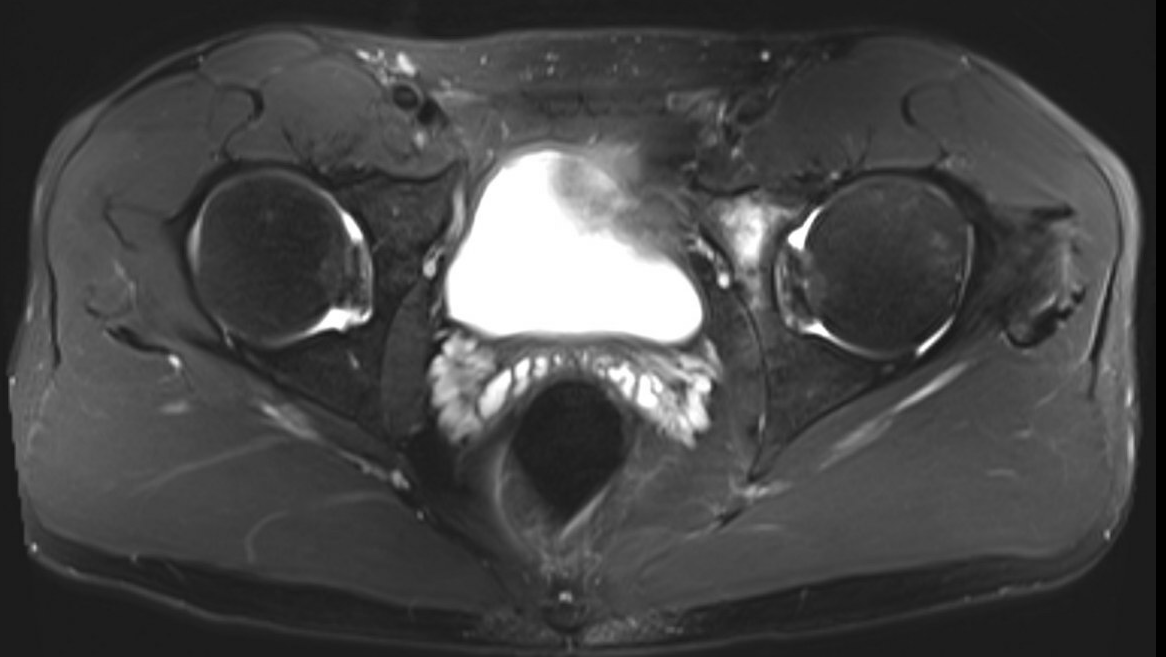
MRI
Labral tears
Best seen on coronal MRI

Saied et al BMC Musculoskeletal Disorders 2017
- systematic review
- labral tears: MRI sensitivity 86% and specificity 83%
- chondral lesions: MRI sensitivity 87% and specificity 72%
- labral tears: MRA sensitivity 91% and specificity 58%
- chondral lesions: MRA sensitivity 75% and specificity 79%
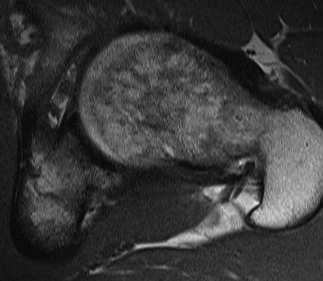
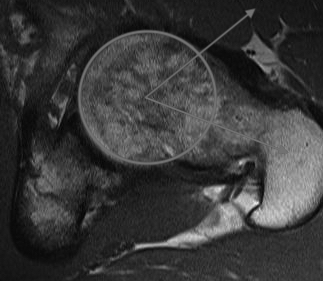
MRI alpha angle
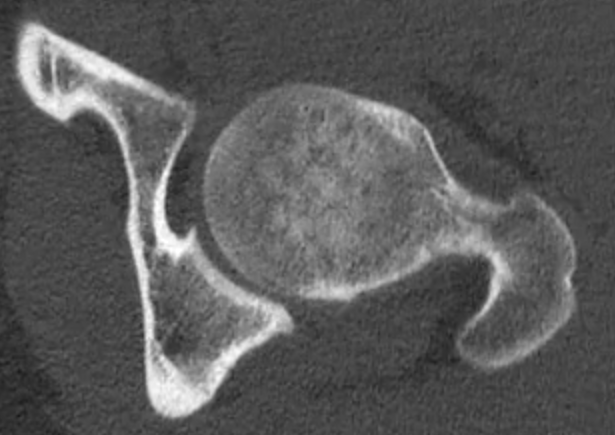
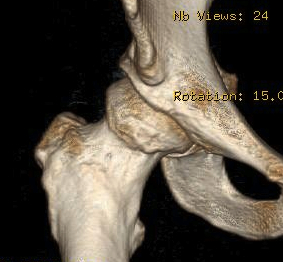
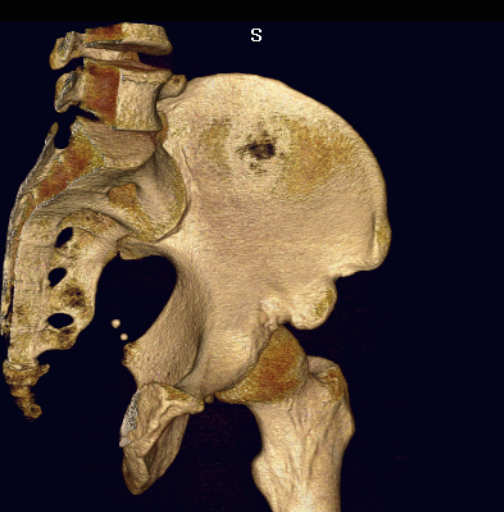
CT
Cam impingement


Pincer
Focal pincer
Os acetabuli
Subspine impingement

Enlarged AIIS likely from old partial avulsion
Osteoarthritis

Tonnis Grade
| Grade 0 | No sign of arthritis |
| Grade 1 | Sclerosis, slight narrowing of joint space |
| Grade 2 | Cyst, moderate narrowing of joint space, loss sphericity of femoral head |
| Grade 3 | Severe narrowing or obliteration of joint space |



Tonnis grade 0 Tonnis grade 1 Tonnis grade 1
Outcomes of hip arthroscopy and mild OA
- 2 year follow up of hip arthroscopy
- < 2 mm joint space 16% conversion to THA
- preserved joint space 2% conversion to THA
- 5 year follow up of hip arthroscopy
- < 2mm joint space versus > 2 mm joint space
- 86% with joint space < 2mm had THA at 5 years
- 16% with preserve joint space had THA at 5 years
- 62 Tonnis grade 0 versus 31 Tonnis grade 1
- minimum 10 year follow up
- 5% THA grade 0 versus 26% THA grade 1
Cam
Kowalczuk et al Sports Med Arthros Rev 2015
- systematic review
- Cam impingement and elevate alpha angles predispose to OA
Pelvic tilt / acetabular retroversion
Definition
Acetabular retroversion causes anterior overcoverage
Likely due to rotational abnormality of the hemipelvis
Xray diagnosis
1. Crossover sign - crossover of the anterior and posterior acetabular wall
2. Positive ischial spine sign - intrapelvic protrusion of the ischial spine
3. Positive posterior wall sign - the posterior wall runs medial to the femoral head center


Crossover sign - anterior wall in red, posterior wall in black
- CT versus xray for measurement of retroversion
- crossover sign and ischial spine sign not reliable
CT / MRI diagnosis
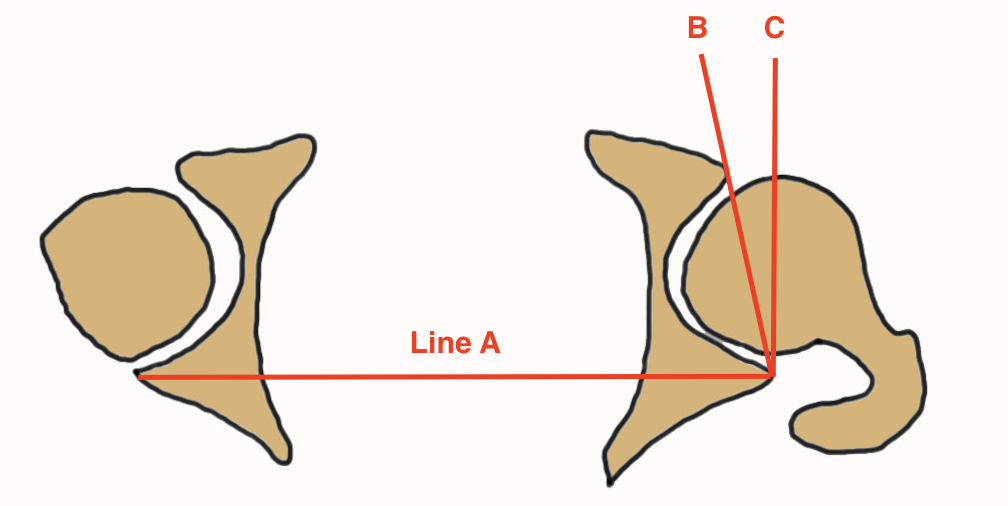
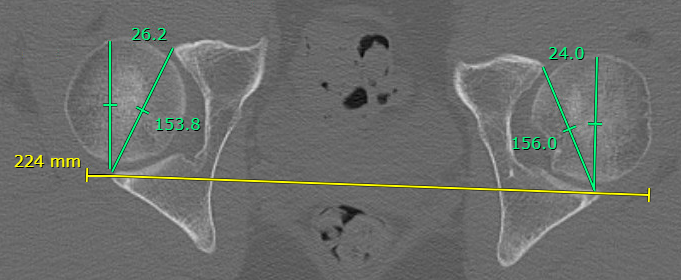
Acetabular version < 15 degrees between B and C
- affected by pelvic tilt and obliquity
- Line A: posterior acetabular walls
- Line B: posterior to anterior acetabular walls
- Line C: perpendicular to line A
Normal acetabular version > 15 degrees
Reduced acetabular version < 15 degrees
Management
Arthroscopy acetabular rim trim
Periacetabular Osteotomy (PAO)
- surgical treatment of acetabular retroversion
- 67 hips undergoing PAO and 57 underwent rim trimming
- no difference in outcomes at 5 years
- 80% 10 year survival for PAO, and 23% survival at 10 years for rim trim
Dysplasia
Borderline Dysplasia
- LCEA 18 - 25 degrees
- systematic review of hip arthroscopy in borderline dysplasia
- 6 articles and 400 studies
- at minimum 5 years follow up, 70% achieved MCID in at least one outcome
Nonoperative management
Physiotherapy
Probst et al J Orthop Sports Phys Therapy 2023
- meta-analysis of 16 studies of non-arthritic hip pain
- overall response rate to nonoperative treatment was 54%
- physiotherapy improved outcomes by average of 11 points on 100 point scale
Injections
- systematic review of 7 studies and 600 patients
- some association between responsiveness to injections and good outcomes after hip arthroscopy
Operative management
Operative versus nonoperative treatment
- meta-analysis of 3 RCTs and 650 patients
- improved outcomes with operative intervention
- 348 patients randomized to surgery v personalized hip therapy
- 1 year follow up, significant improvements in hip arthroscopy group
- mean iHOT-33 scores had improved from 39·2 to 58·8 for hip arthroscopy group
- mean iHOT-33 35·6 to 49·7 in the personalised hip therapy group
Operative outcomes
- systematic review of 91 studies and 10,000 hips
- > 90% met MCID
- 88% achieved PASS for mHHS but 25 - 30% for HOS
- 6% revision rate hip arthroscopy
- 6% THA
Factors associated with outcomes
Sogbein et al Orthop J Sports Med 2019
- systematic review of 39 studies and 9000 hips
- male, Tonnis grade 0, younger age, BMI < 25 and relief with intra-articular injections associated with good outcomes
- female, > 45, < 2 mm joint space, increase LCEA and labral debridement associated with poorer outcomes
Labrum Repair v Debridement
- 76 labral repairs matched to 76 labral debridement controls
- significant improvement in both groups
- no signficant difference between groups
Wirries et al Arthroscopy 2024
- German registry
- 963 labral repair versus 673 labral debridement
- no difference in outcome
- at 5 years > 90% arthroplasty free survival in both groups
- outcomes and THA influenced by cartilage status at time of surgery
Cam Resection
- systematic review
- correction postoperative alpha angle associated with improved outcomes
- 707 patients
- postoperative alpha angle associated with outcome
Capsular repair
Dasari et al Orthop J Sports Med 2023
- systematic review of capsular closure
- superior outcomes with complete capsular closure
Prevention of OA / Hip Preservation
- 100 patients with minimum 10 year follow up
- hip arthroscopy on one side only
- hip arthroscopy side: worse Tonnis grade 28%
- nonoperative hip: worse Tonnis grade 48%
- progression of OA associated with borderline dysplasia and alpha angle > 65 degrees