Ellman Classification
| Type | Depth |
|---|---|
|
Articular sided
Bursal sided
Intratendinous |
Grade 1: < 3mm
Grade 2 < 3-6 mm
Grade 3 < 6 mm |
Bursal, articular and interstitial partial tears
Etiology
External - subacromial impingement, internal impingement / throwing athlete, instability, overuse
Intrinsic - aging, tendinopathy, diabetes
Incidence
Normal population
- MRI of 96 asymptomatic shoulders
- partial thickness tears 20%
- < 40: 4%
- > 60: 26%
Overhead athlete
- MRI of 20 overhead athlete asymptomatic shoulders
- 40% of dominant shoulders had partial thickness RC tears
Natural history
Lo et al Open Access J Sports Med 2018
- 76 patients with partial tear on MRI
- follow up with repeat MRI at mean 4 years
- 76% no progression
- 8% developed full thickness tears
- > 50% depth: 55% progression
- < 50% depth: 14% progression
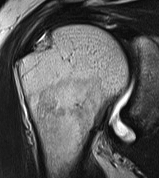
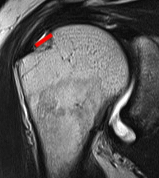
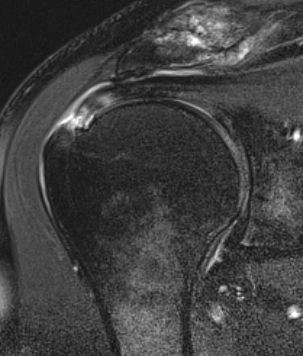
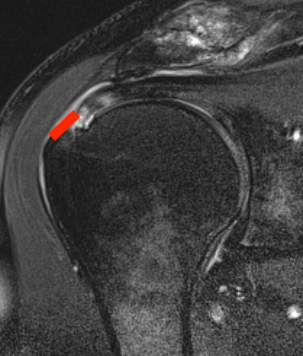
MRI
Articular Sided / PASTA (partial articular sided tendon avulsion)


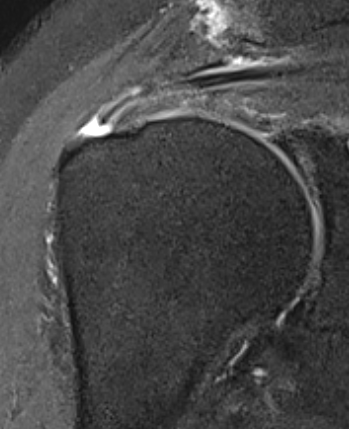
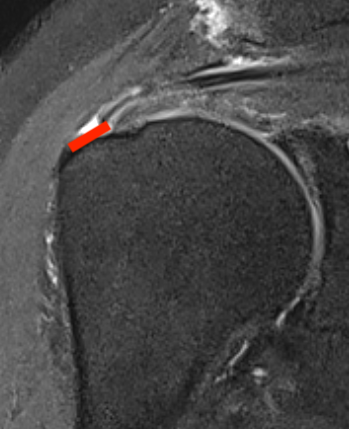
Bursal Sided
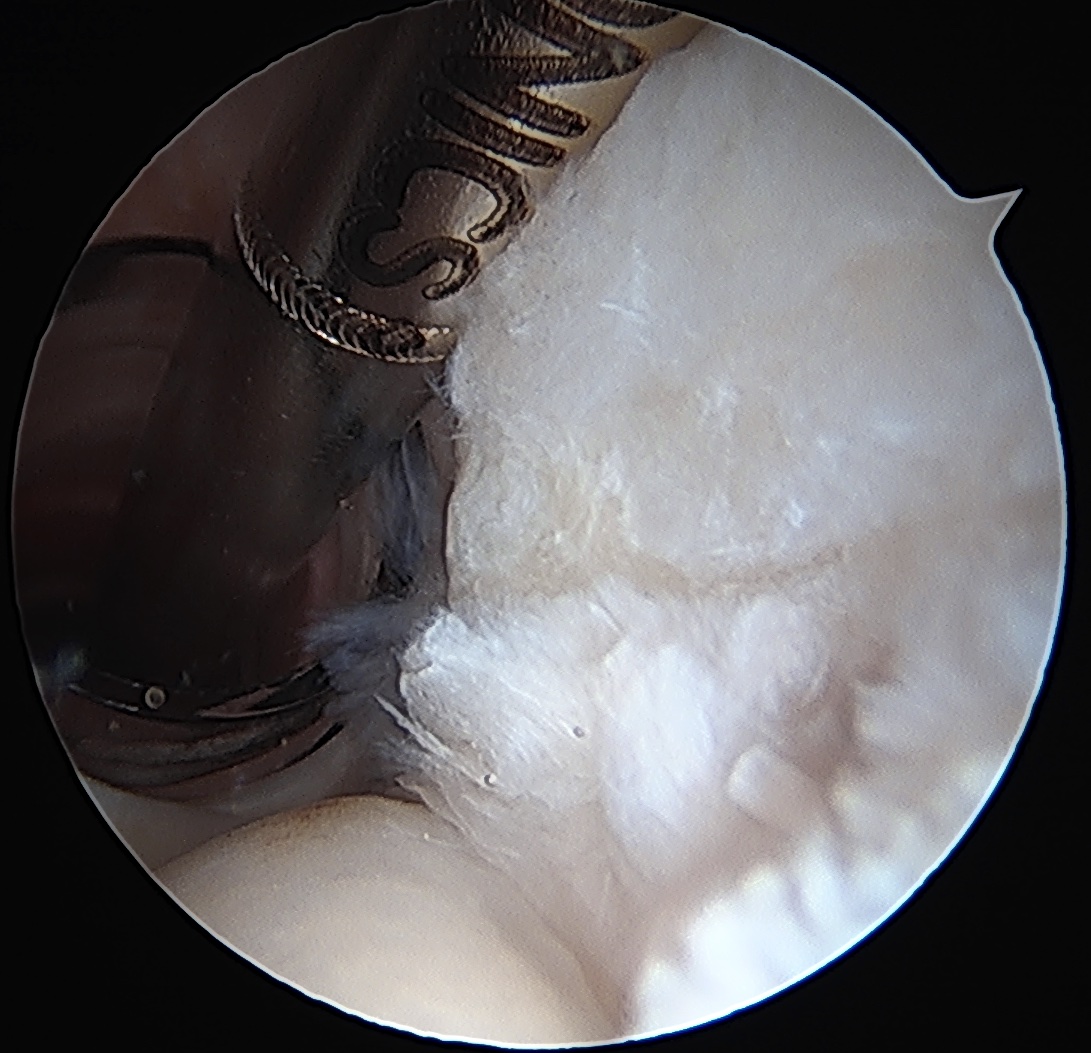
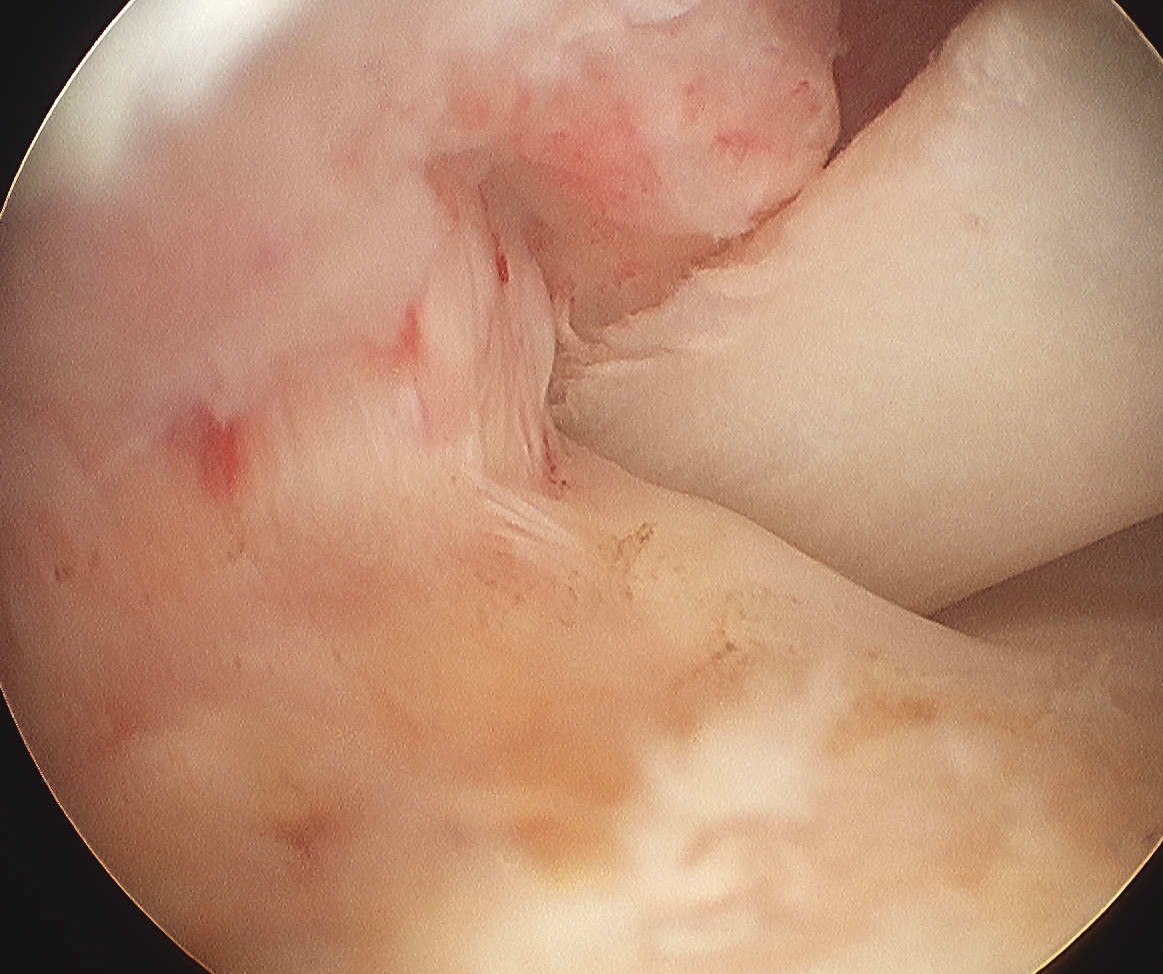
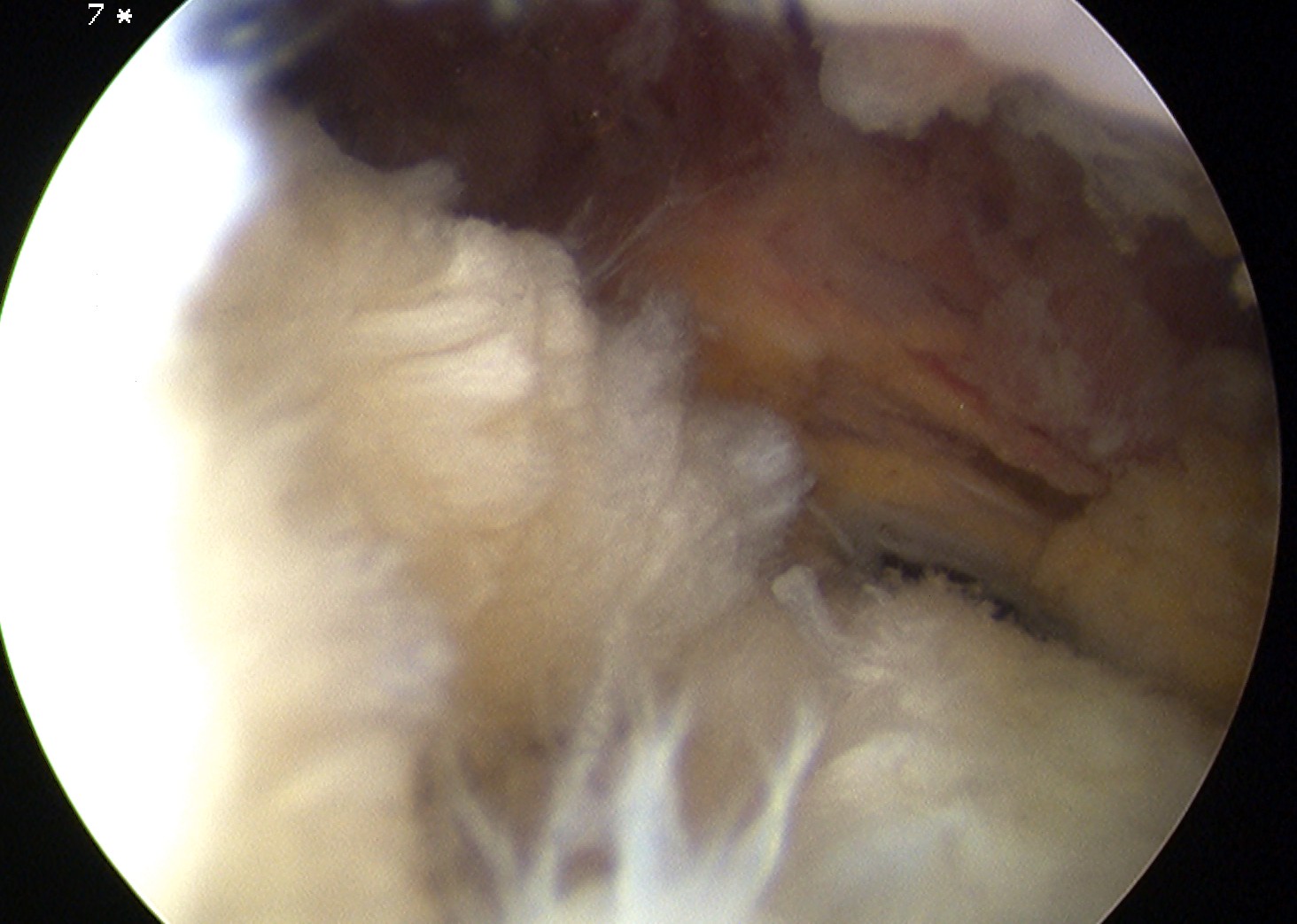
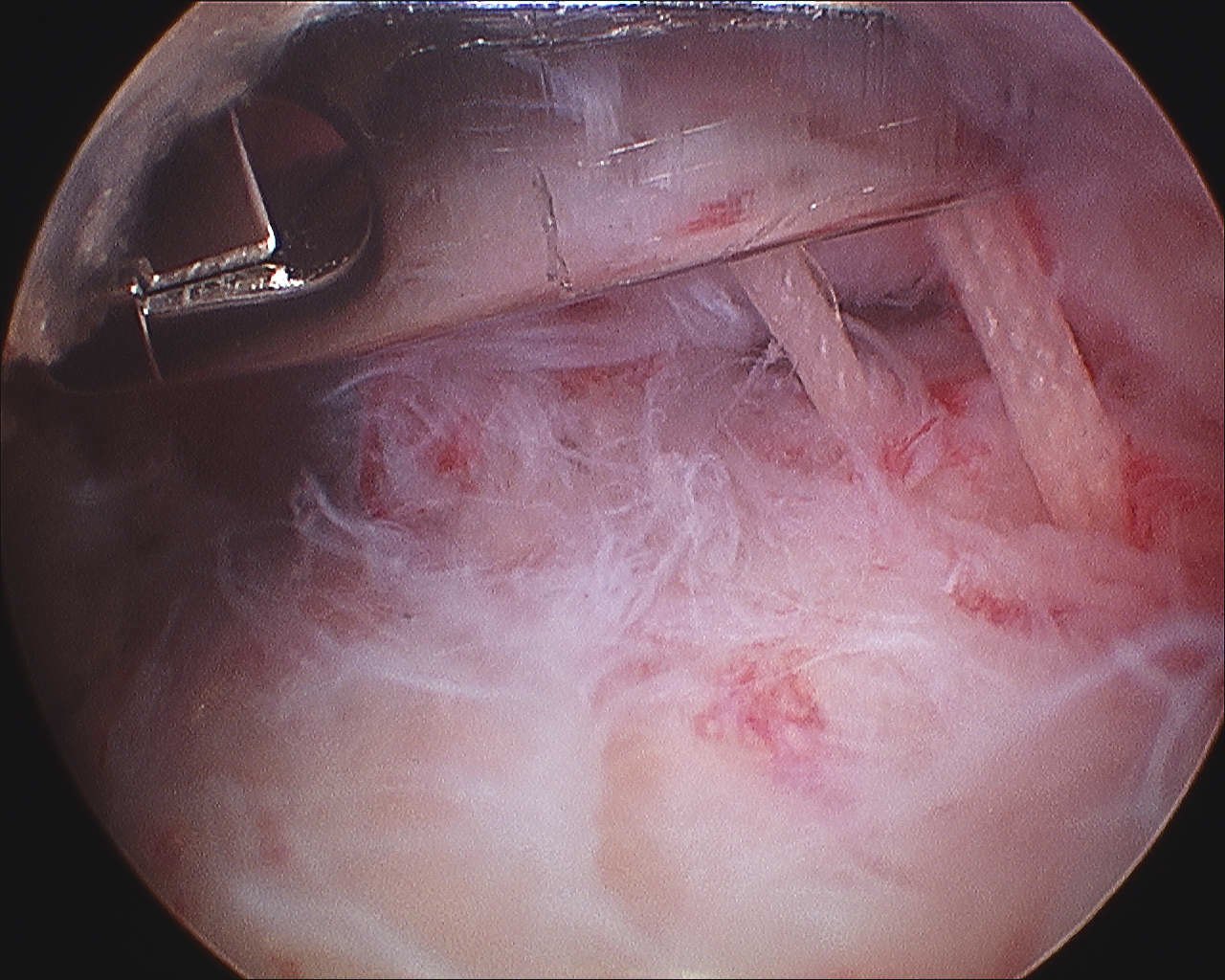
Arthroscopy
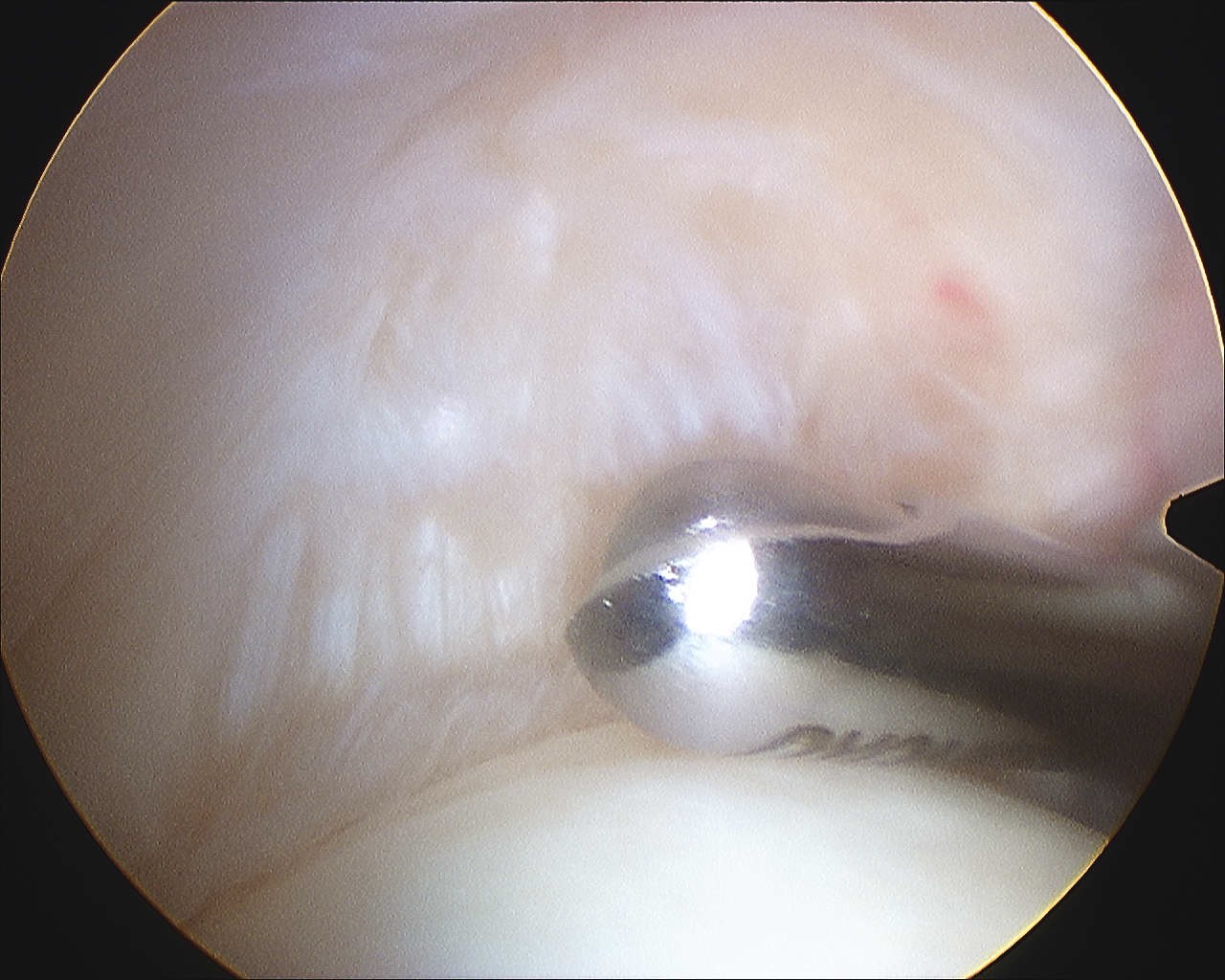
Articular side
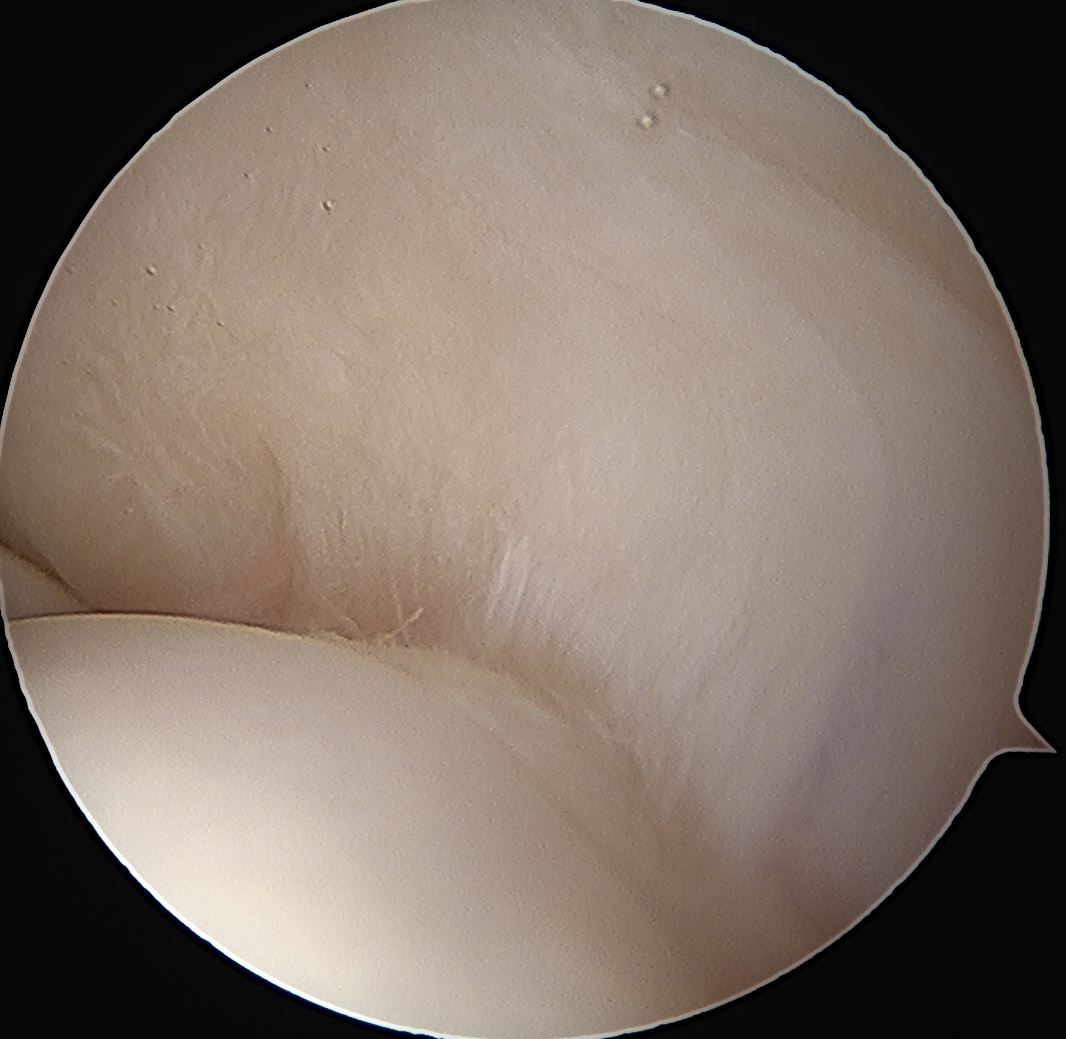
Normal insertion of undersurface of the rotator cuff onto the footprint, with camera in glenohumeral joint
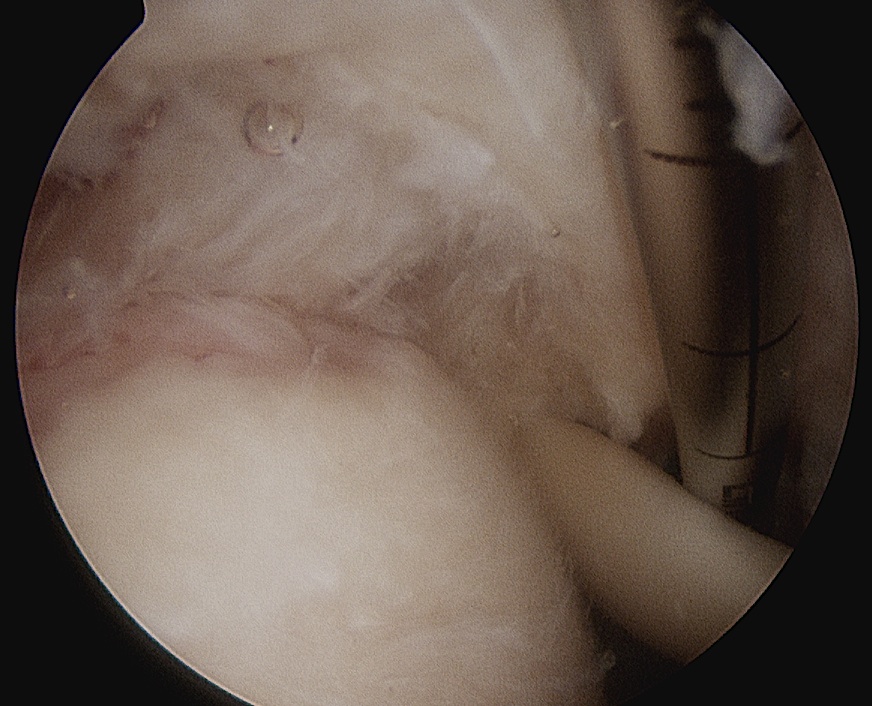

> 50% uncovering of footprint in glenohumeral joint
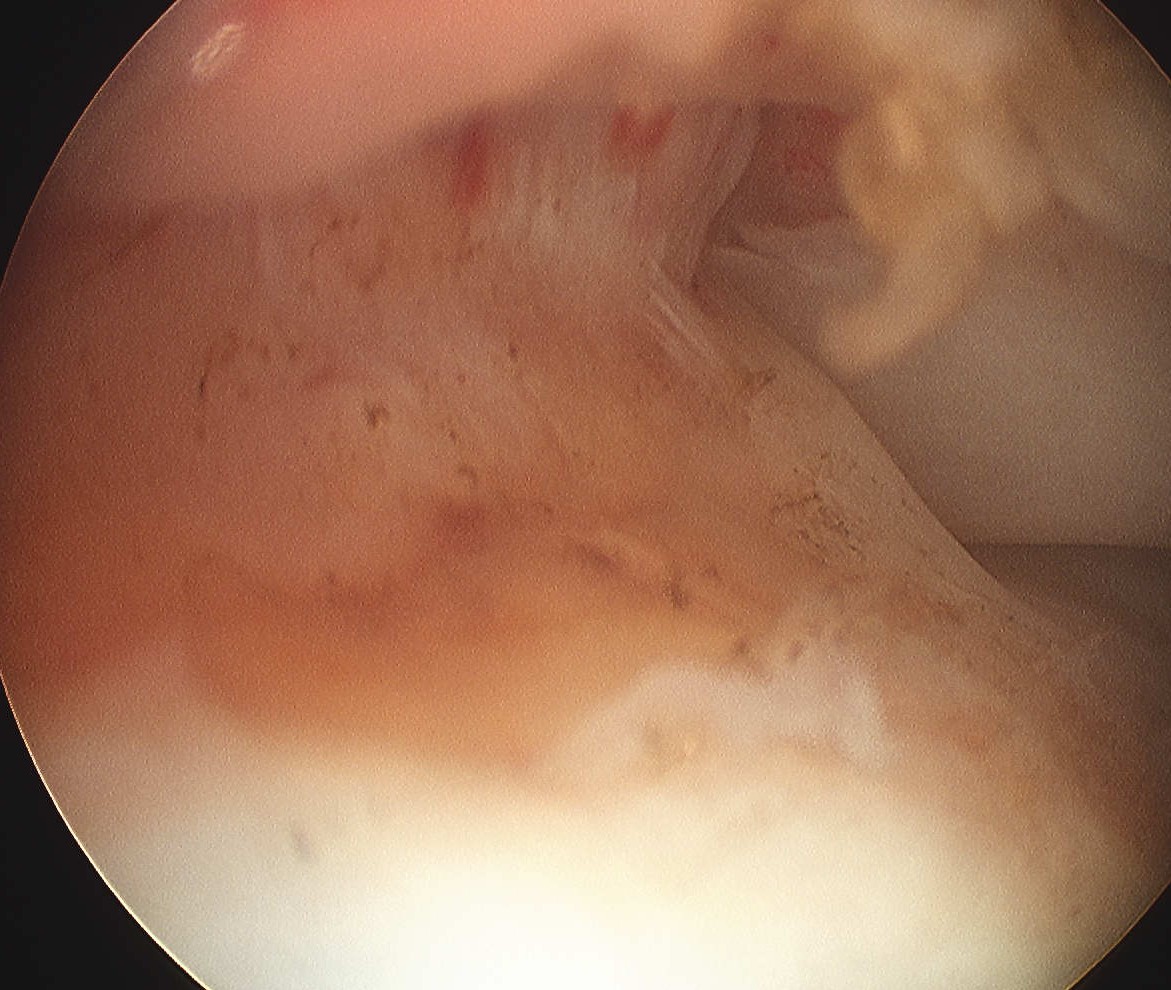
> 50% uncovering of footprint in glenohumeral joint
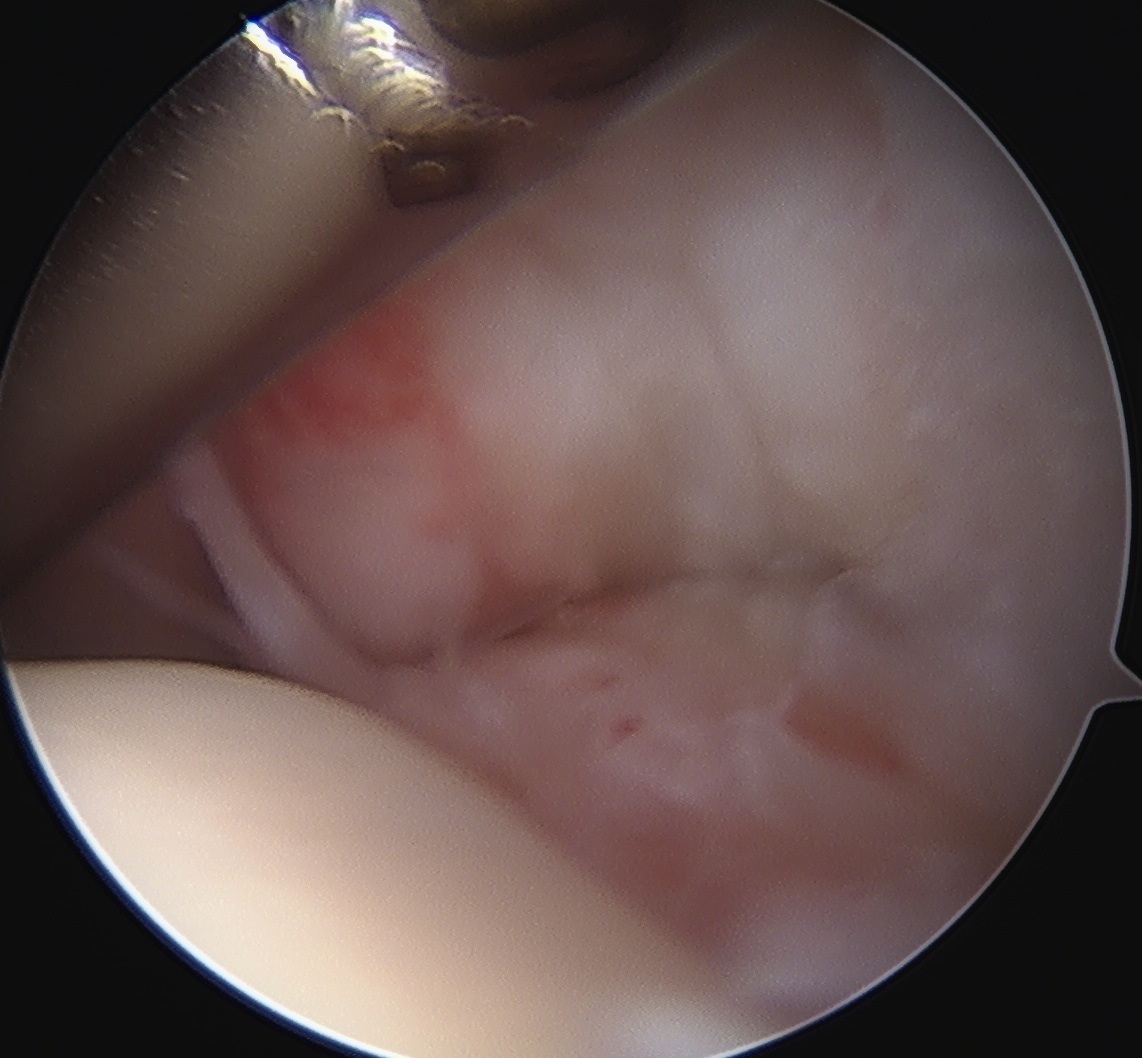
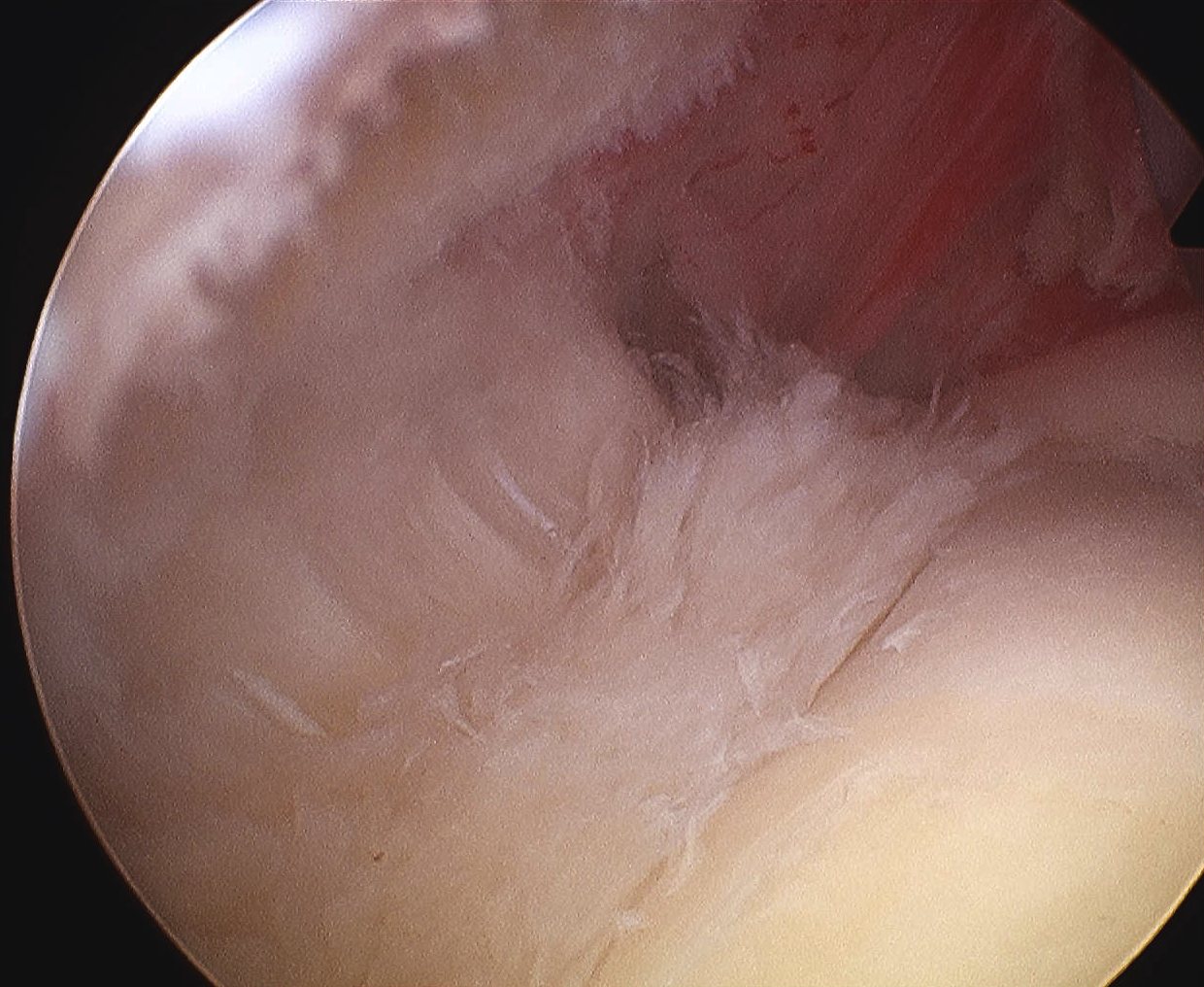
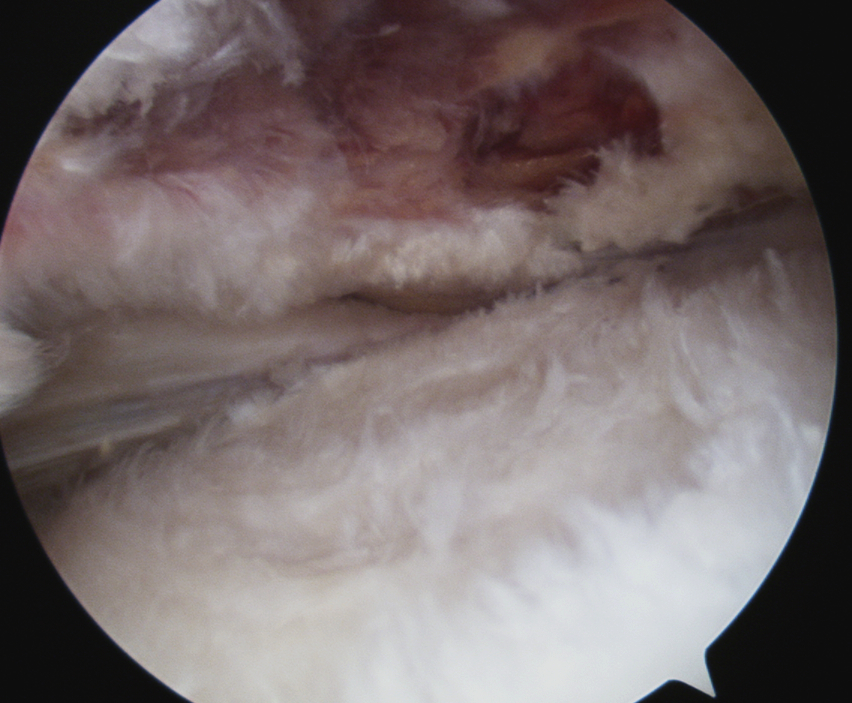
Bursal Sided
> 50% bursal sided tears with camer in subacromial space
Nonoperative management
PRP
- systematic review of PRP for partial thickness RC tears
- PRP superior to control at 6 months
Operative
Indications
Ongoing pain
Partial thickness > 50% of depth
Options
Repair in situ / transtendinous repair
Conversion to full thickness tear / tear completion and repair
Results
- RCT of 74 patients with PASTA lesions
- trans-tendon repair versus tear completion and repair
- no difference in functional outcomes
- increased strength with completion and repair
- RCT of 48 patients with > 50% PASTA
- trans-tendon repair versus tear completion and repair
- more pain and stiffness in trans-tendon repair for first 3 months
- 2 retears in tear completion group at 6 month MRI
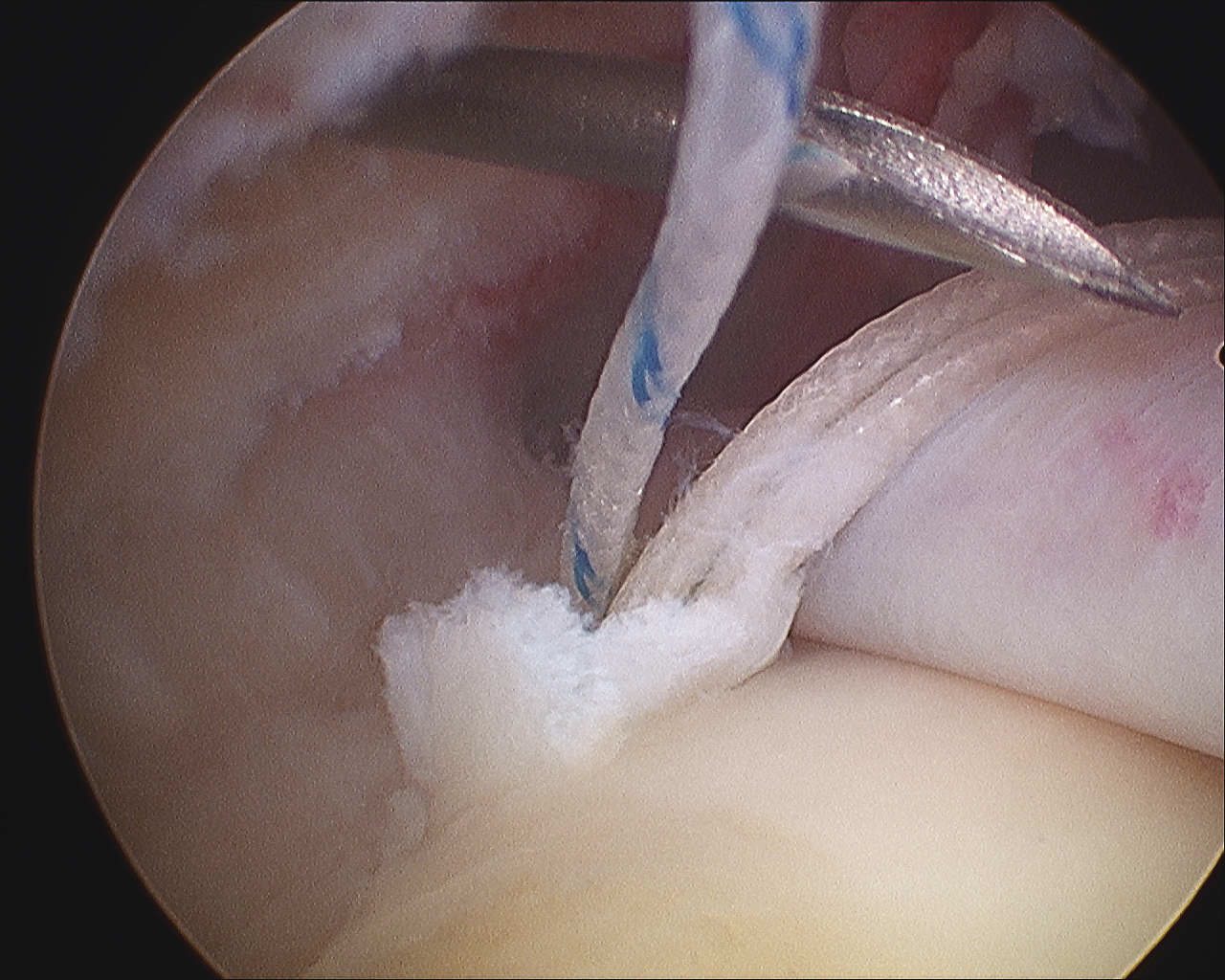
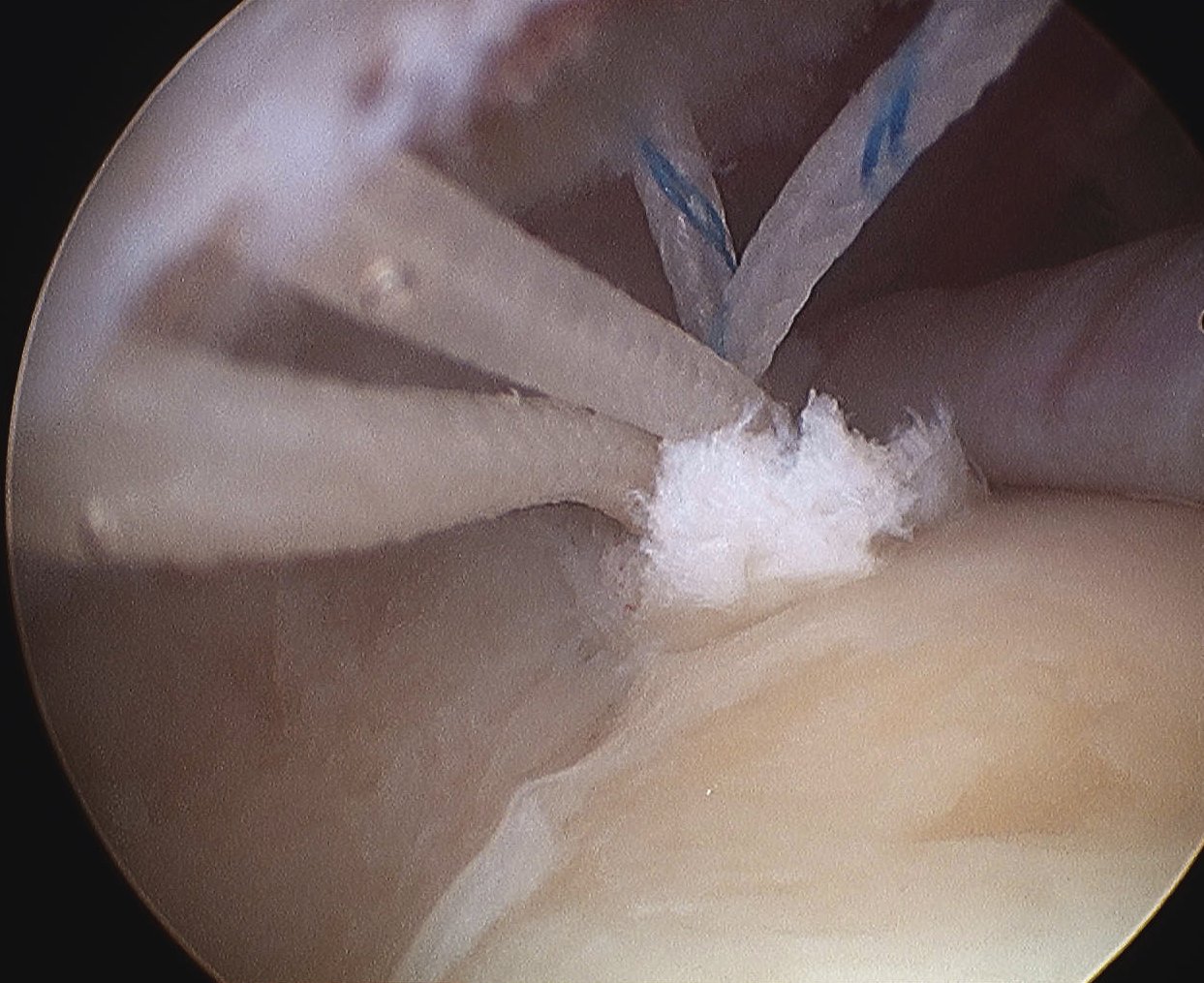
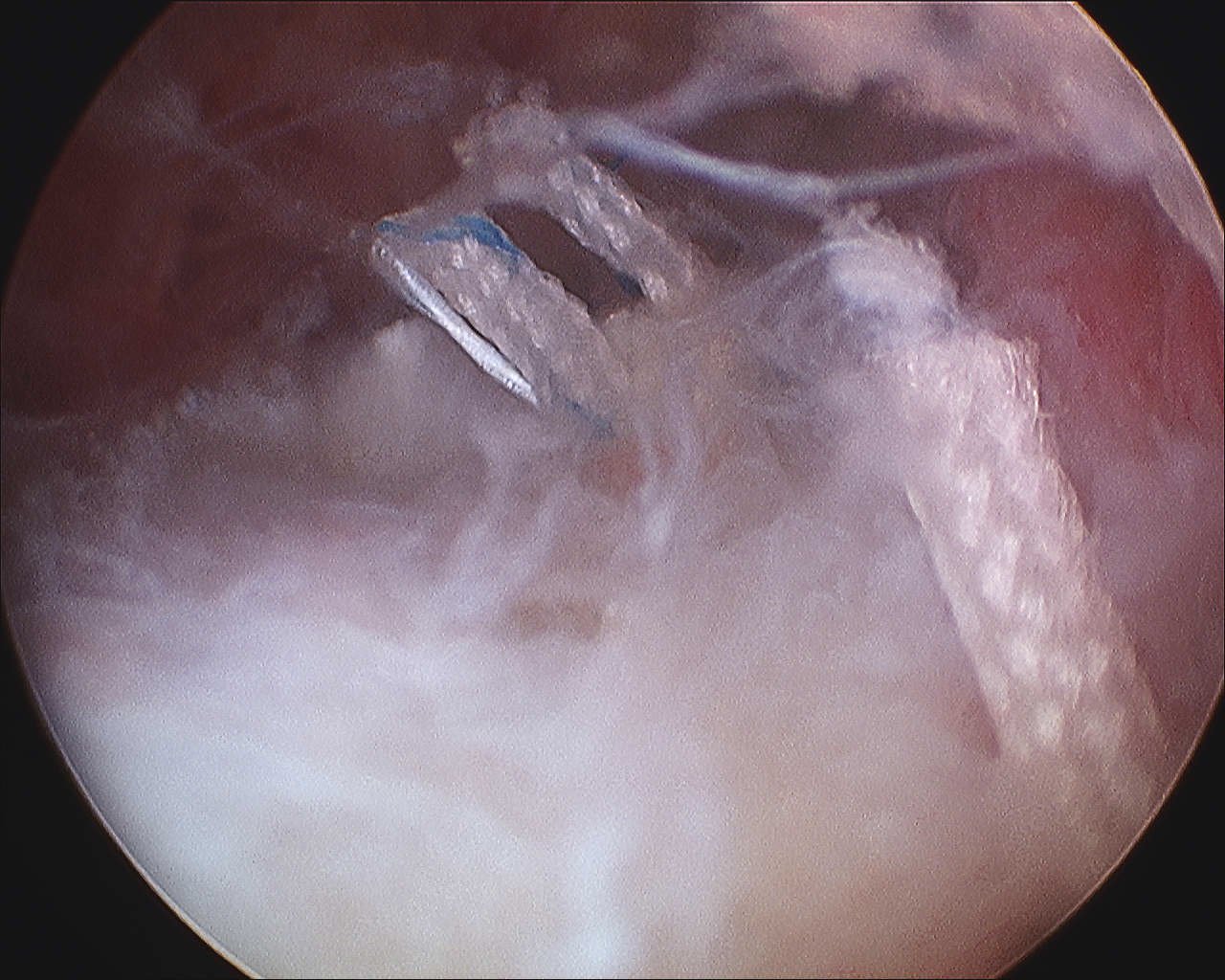
Trans-tendinous repair
Arthroscopic PASTA technique
Technique
Vumedi PASTA transtendon repair video
Vumedi PASTA transtendon repair video 2
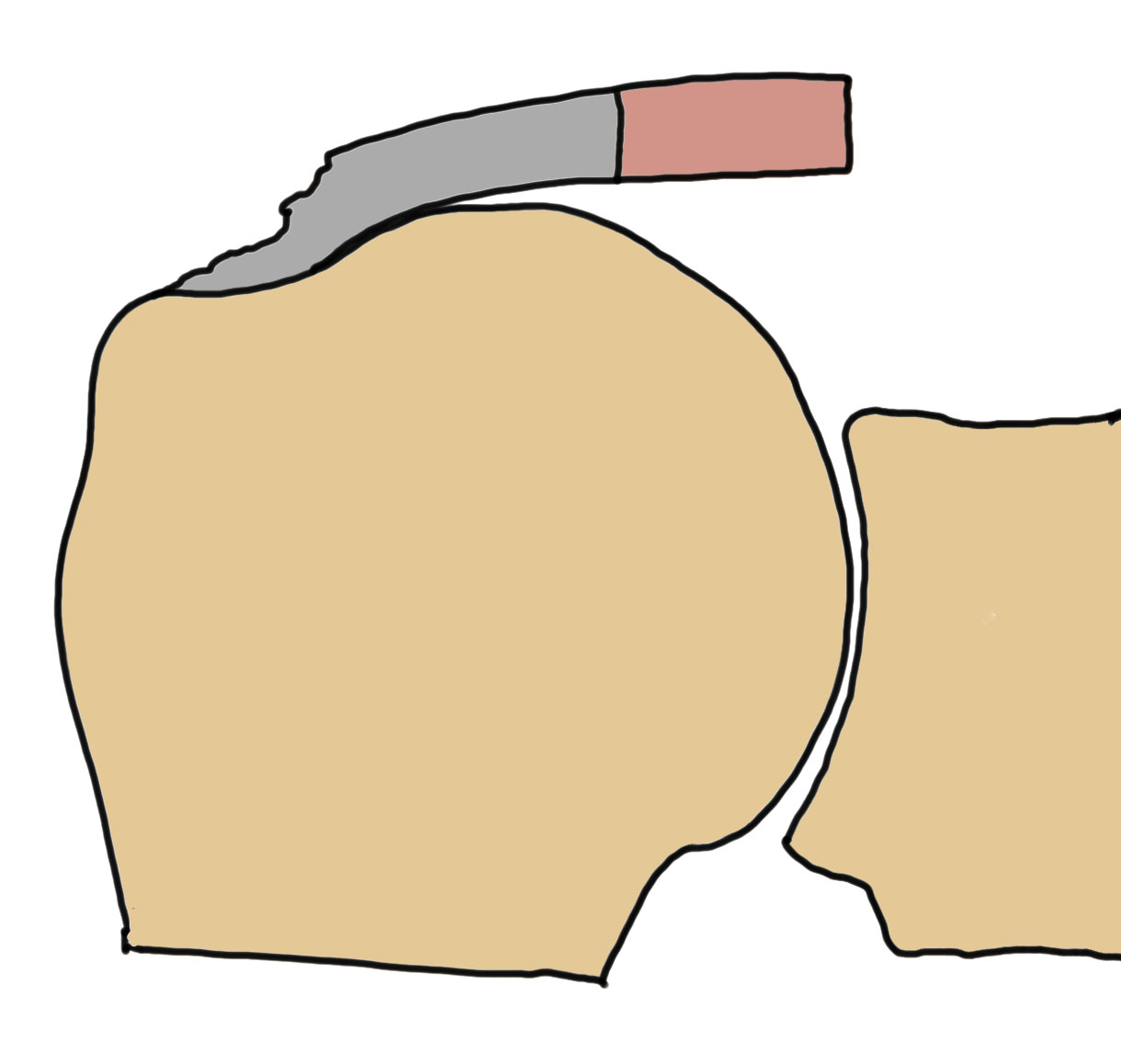
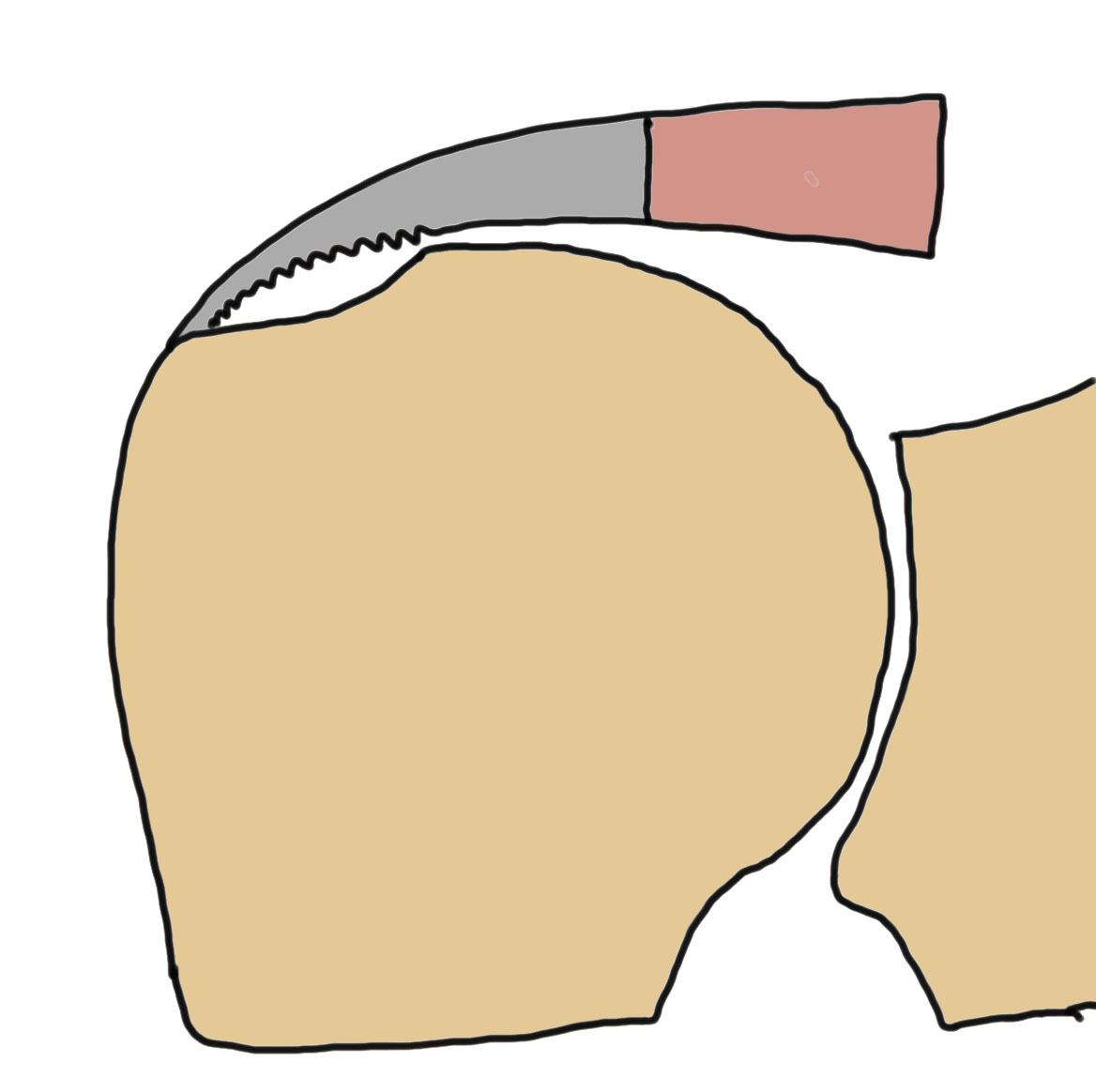
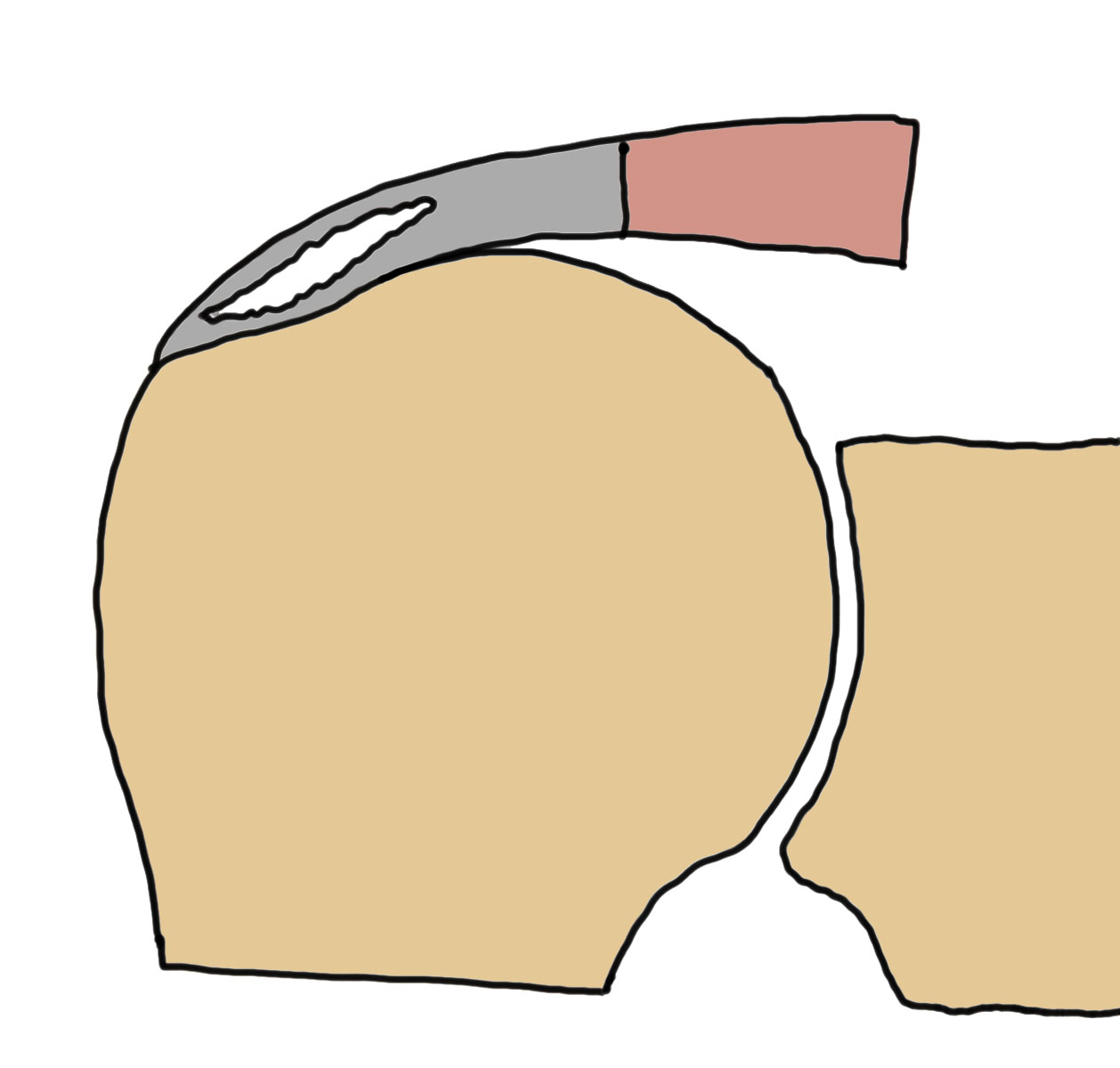
Camera in glenohumeral joint
- debride insertion onto footprint
- 5mm anchor passed through musculotendinoous junction into footprint
- use birds beak suture to retrieve sutures / suture shuttle using spinal needle
- tie in subacomial space
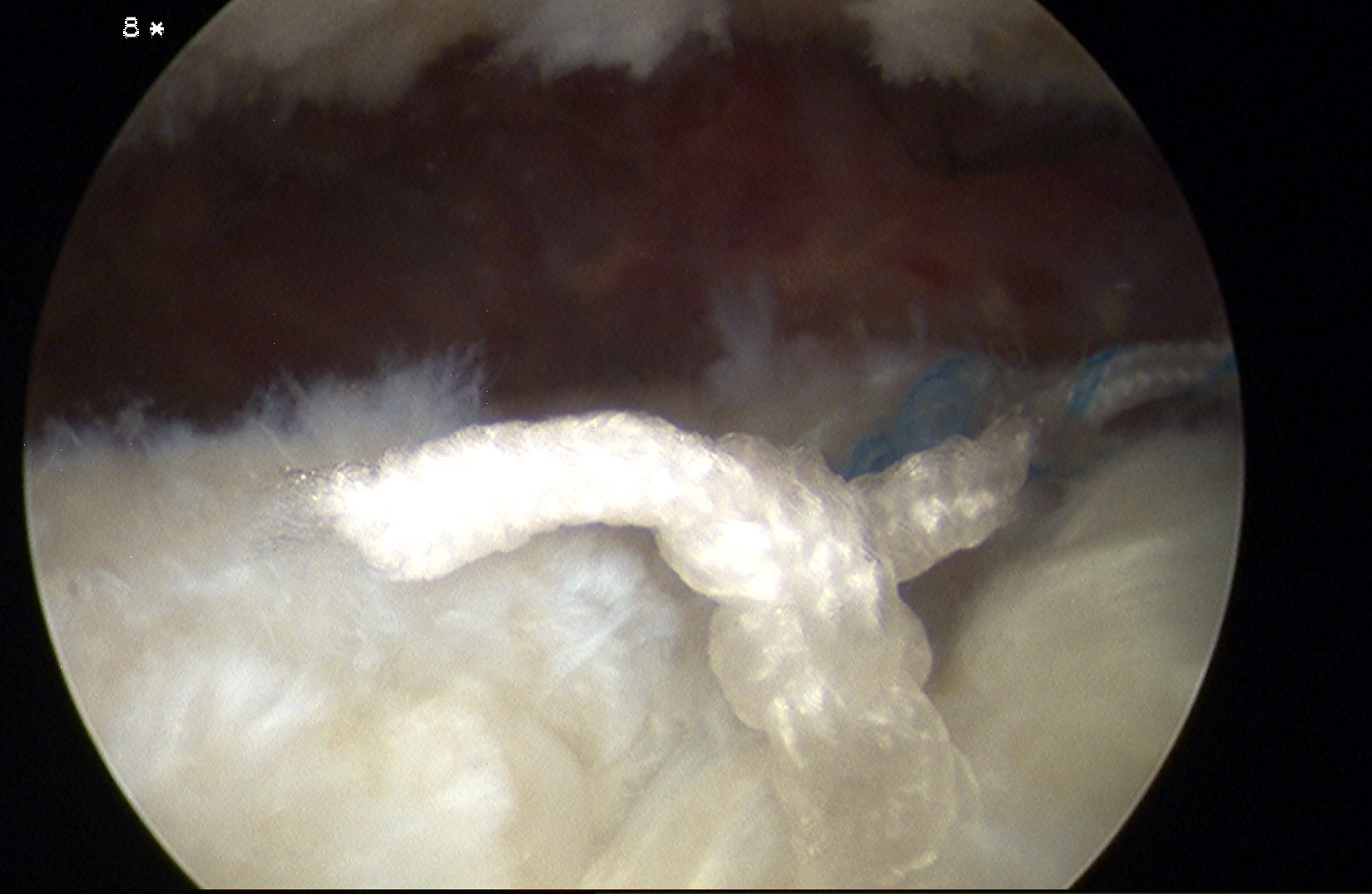
Arthroscopic bursal sided tear technique
Technique
Vumedi bursal sided tear repair
Vumedi bursal sided tear repair + scaffold augmentation
Camera in subacromial space
- identify bursal sided tear
- debride footprint
- repair top layer of tendon using anchor in footprint
Arthroscopic treatment of intra-tendinous tears
Arthroscopy techniques trans-tendinous repair of intra-tendinous tear PDF
Tear completion and repair
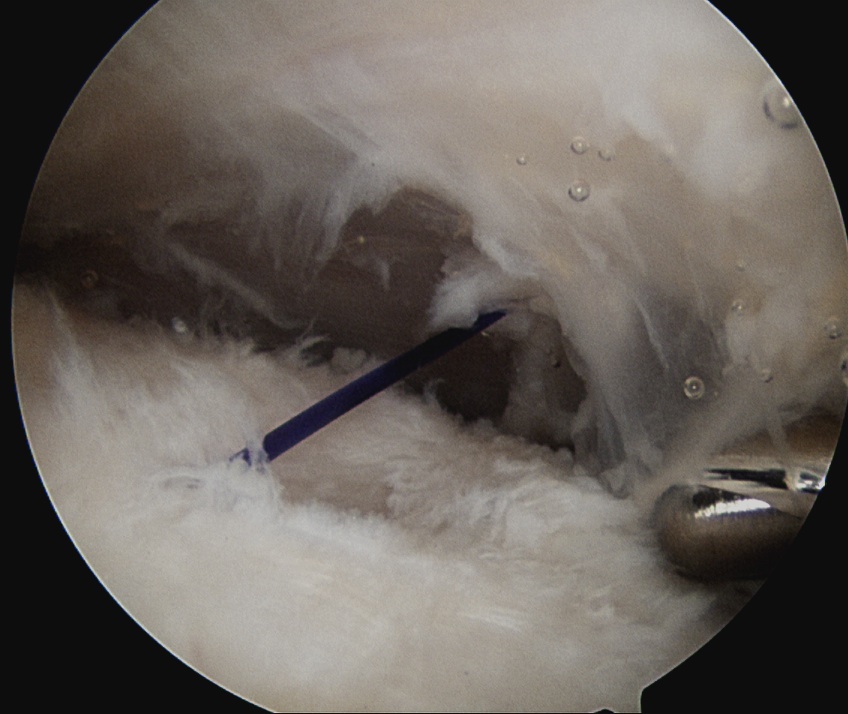
Articular sided tear / PASTA
Technique
Vumedi PASTA takedown and repair video
Camera in glenohumeral joint
- use spinal needle to identify center of PASTA
- pass 1 PDS to mark lesion
- camera into subacromial space
- use suture to identify area for tear completion
- cautery or knife to complete tear
- double row repair
Bursal sided tear
Technique
Camera in subacromial space
- identify bursal sided tear
- complete with cautery
- double row repair
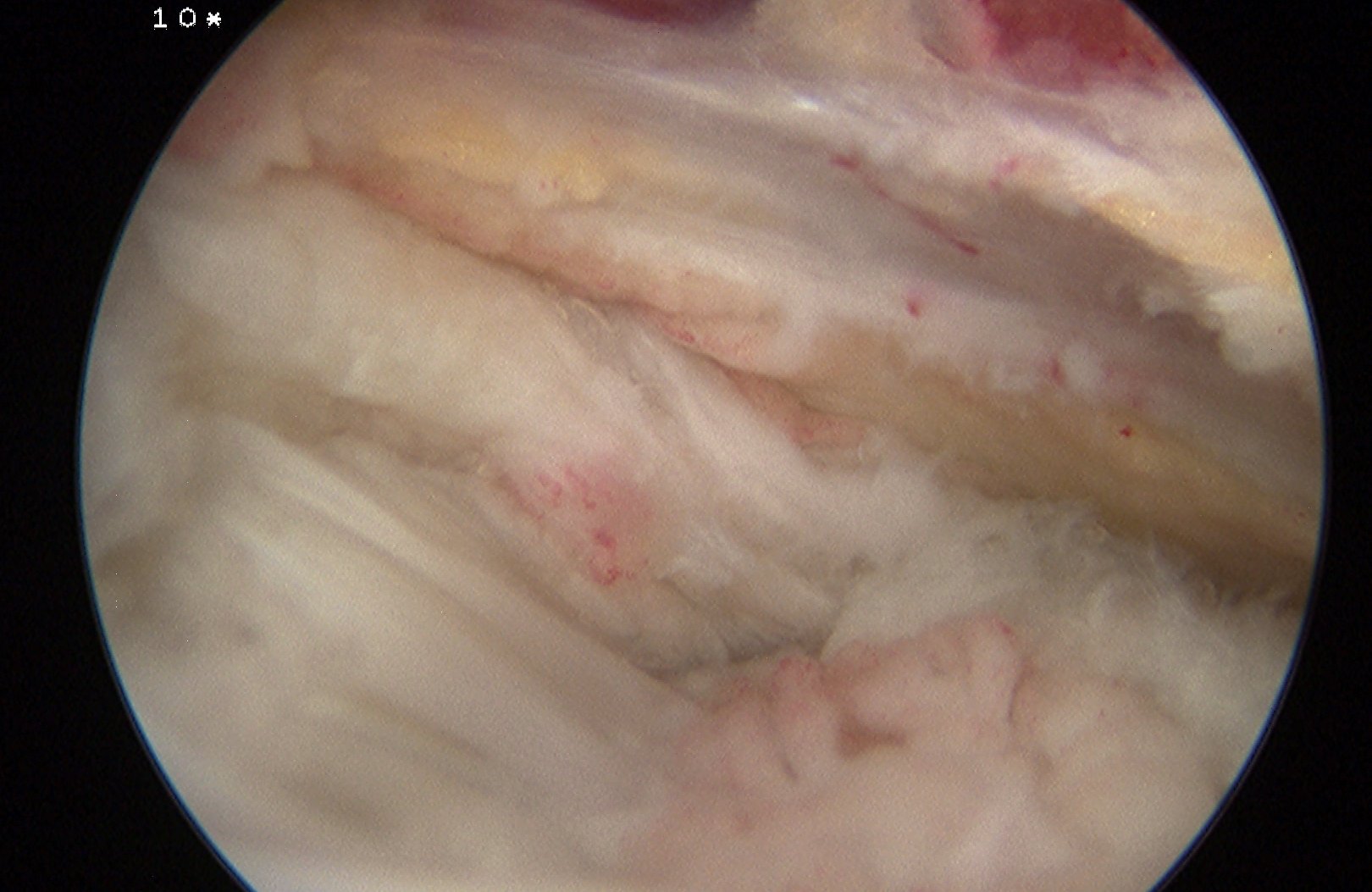
Acromioplasty + debridement
Indications
< 50% tears
Failure of nonoperative treatment
Results
- debridement for 40 articular sided and 36 bursal sided tears < 50%
- significant improvement in both groups at 2 years
Debridement of low grade PASTA Debridement of low grade bursal sided tear